
Abstract
Background:
Older autistic adults are at risk of social isolation and are more likely to experience physical and mental health conditions compared with non-autistic older adults. However, the needs and experiences of older autistic adults, and the perspectives of autistic adults (across ages) about growing older, are an under-researched area.
Methods:
We conducted a mixed methods online survey to explore factors that may help autistic people to do well in older age, what worries people about older age, changes in experiences of being autistic with age, and priorities for future research. We recruited 121 autistic adults aged 18–88 from the United Kingdom, mainly via social media. We employed quantitative and qualitative data analysis methods.
Results:
We generated three categories from participants’ free-text responses: (1) health, care, and wider societal support; (2) independence and autonomy; and (3) social connectedness. Qualitative findings supported the quantitative findings that maintaining physical and mental health, independence and autonomy, and social relationships were considered important. Participants worried about a lack of appropriate support from health and care staff, age-related health conditions such as dementia and menopause, and not having intersectional needs understood or met. Some participants reported their experience of being autistic became easier with age, and others found it more difficult. Participants suggested future research could include health and care staff and services (including care homes), health conditions (e.g., dementia), autistic-specific needs and concerns (e.g., changes in sensory sensitivities with age), social life and support, and independent living.
Conclusions:
This study highlights supportive factors and concerns in relation to autistic aging. Our findings support recent research and highlight underexplored areas such as care home experiences, dementia, menopause, and LGBTQIA+ aging needs. Findings will help to inform health and care provision as well as directing future research in line with the priorities of the autistic community.
Community Brief
Why is this an important issue?
We know that social support and relationships contribute to better quality of life in older autistic adults. However, we do not know enough about the experiences of older autistic adults, what might help autistic people to do well in older age, and what worries autistic people about growing older.
What was the purpose of this study?
To understand the experiences and support needs of autistic people as they age and identify priorities for future research about aging.
What did the researchers do?
We worked with autistic individuals to create an online survey about growing older. The survey asked participants to rate (between 1 and 5) certain aspects of aging and asked participants “open-ended” questions, where participants could write what they wanted. Open questions asked what might help people to do well in older age, what might worry people about older age, and whether their experience of being autistic has changed as they have grown older. We also asked people what aging-related topics they think future research should look at. In total, 121 autistic people took part, aged 18–88. We looked for patterns across the responses where participants wrote similar or different things.
What were the results of the study?
We found that participants had many concerns about “aging well.” These included concerns about health and conditions such as dementia and menopause, the suitability and quality of care, and wider support and understanding from across society as well as closer relationships. Participants also worried about losing their independence and autonomy, having to move to unsuitable care homes, isolation, and a lack of support and social connectedness. Given this, we suggest that future research could focus on health and social care staff and services (including care homes), health conditions (e.g., dementia), autistic-specific needs and concerns (e.g., changes in sensory sensitivities with age), social life and support, and independent living.
What do these findings add to what was already known?
Our findings confirm previous research about worries over losing independence and the need for health and care staff to be more aware of older autistic people’s needs. Our findings highlight the underexplored areas of care home living and health conditions such as dementia.
What are potential weaknesses in the study?
The study captures and reports the experiences of a small group of people compared with the wider autistic population, and these may not be relevant to everyone. Most participants were White British and had a degree, so views from the wider autistic population and particularly those with different backgrounds may not be reflected in this study.
How will these findings help autistic adults now or in the future?
These findings help to validate the experiences, hopes, and fears of autistic individuals; provide evidence to help people advocate for their needs; and provide information for health and care professionals to help them provide care and support for older autistic adults. Important topics for future research are also suggested.
Introduction
Research looking at the experiences and support needs of older autistic adults is limited. 1 Indeed, <1% of published autism studies over the past 10 years have focused on older adults. 2 This is important, as the age-related experiences of autistic adults are likely to differ from their non-autistic counterparts. Similarly, younger autistic adults may have different views or concerns about their future aging, given that the salience and self-relevance of social stereotypes about aging and older people change with age. 3 Expectations about aging also tend to be more negative at younger ages 4 and levels of anxiety about aging higher. 5 Qualitative research with autistic women has suggested that menopause may exacerbate some experiences, such as sensory sensitivities and communication difficulties, and could lead to poorer mental health. 6 Older autistic adults show an increased prevalence of many physical and mental health conditions compared with non-autistic older adults,1,7 suggesting a greater need for health and care services. Cognitive decline may be more common in autistic compared with non-autistic older adults, 8 and autistic people have expressed concerns about dementia, 9 although the evidence regarding the risk of dementia in autistic adults is conflicting.1,10,11 Despite this increased prevalence of health conditions, autistic adults across age ranges experience barriers to healthcare and subsequent adverse health outcomes. 12 The aim of this study was to explore the experiences and views of autistic adults across all ages, in relation to growing older.
Declining health in older age may impact the ability of autistic people to live independently, necessitating a move to residential care. There is currently a paucity of research regarding older autistic adults’ experiences of residential care. Research with non-autistic adults suggests that most people are reluctant to move to a care home, 13 and outcomes from meetings of a multidisciplinary expert group suggest the move to residential care should be carefully managed for autistic adults. 14 Crompton et al. 14 highlighted the need to consider and manage the sensory and built environment of residential care and noted the importance of autism training for residential care staff, which is currently lacking. They suggested training is needed to enable staff to recognize the support needs of older autistic adults, as well as how to support their well-being in a residential care setting. 14 Support for well-being is particularly important due to the higher rates of mental health problems experienced by older autistic adults.
The increased prevalence of mental health problems in older autistic adults may be understood in part through the minority stress model, whereby stigma, discrimination, and victimization contribute to poor mental health. 15 This may be particularly applicable if such experiences are accumulated over a lifetime. Later diagnosis of autism is also associated with poor mental health. For example, Atherton et al. 16 reported an association between diagnosis of autism in later life and lower quality of life and that prior to diagnosis, people may mask their autistic characteristics, which can be stressful and exhausting. Receiving a diagnosis can bring greater self-acceptance and lead to new social connections. 17 Relationships and social support are important predictors of quality of life for autistic adults across age ranges 18 and contribute to better quality of life in middle-aged and older autistic adults. 19 This points to the importance of addressing these issues throughout the life course.
A recent qualitative interview study with 17 autistic adults aged 46–72 years highlighted important ways that people’s autistic characteristics could change with age or interact with age-related issues and experiences. 9 For instance, some participants reported considerable dependence on parental and family support, which put them at increased risk of isolation with increased age. They also reported a lack of knowledge and role models relating to being autistic and aging, felt themselves to be at increased risk of some age-related health conditions, and yet also reported increased barriers to engaging in health-promoting behaviors. The study also showed that many age-related health and social care services are not well-suited to autistic people and that many of the health and social care staff that they engaged with lacked the knowledge and understanding of autistic people needed to support them. However, these findings were based on a relatively small number of participants who were limited in age range (with only 5 participants aged over 61) and gender (10 women, 7 men). Participant’s sexual orientation was not reported. The study only included people who were formally diagnosed as autistic. This is problematic as it means that valuable insights may have been missed from middle-aged and older people who identify as autistic but have never been given a diagnosis due to, for instance, a lack of knowledge about autistic people, masking of autistic characteristics, or lack of opportunity for a diagnosis. 20 There is therefore a need to explore these issues in a wider and more diverse sample of autistic people.
Aging is an important issue that affects everyone, yet little is known about how younger autistic adults feel about growing older or what they think could support them to age well. As participants in previous research have reported a lack of knowledge about aging, 9 we wanted to explore this topic in a larger sample of younger as well as older autistic adults. In the current study, we used a codesigned survey to explore some of the findings previously reported in a small qualitative study 9 in a larger, more diverse sample of autistic people. Our study is founded on respect for autistic people’s rights to determine what is important for their quality of life and provides participants with an opportunity to articulate what is important for them without relying purely on standardized measures, which may lack validity for autistic individuals. 21 The overall aim of the study was to identify the experiences, support needs, and research priorities of autistic people in relation to aging and to see whether these are related to participant age.
Methods
For this study, we employed a convergent mixed methods design 22 with parallel collection of quantitative and qualitative data using a codesigned online survey.
Community involvement
In accordance with guidelines for conducting research studies with the autism community, 23 we involved autistic individuals (researchers and stakeholders) throughout the project. Two autistic researchers/coauthors advised on the project throughout, including topic development, survey design, and data analysis. In addition, we designed the survey in consultation with members of the Autism@Manchester Expert by Experience group at the University of Manchester. This is a diverse group of over 50 autistic people and family members, including people with a range of different genders, sexual orientations, and ethnicities. See the Survey Development section for further details. We discussed the findings with autistic stakeholders throughout the analytic process to aid interpretation of the data, support category development, and situate the results in a wider context.
Participants
To be eligible for this study, participants had to be 18 years of age or older, living in the United Kingdom, and self-report being formally diagnosed as autistic, be waiting for a diagnosis, or self-identify as autistic. We recruited participants via social media (including Twitter/X with the hashtag #AutisticElders, and Facebook) and via online and in-person community groups. These included the Autism@Manchester Expert by Experience group, the Autism@Manchester email list of members of the public (including autistic people), Autism@Manchester social media channels, and a number of open and closed Facebook groups, including some for late-diagnosed and older autistic adults. We opened the study for participation between June 19, 2023, and July 11, 2023, due to the overall resource limitations of the project. The survey text advised participants that at the end they would have the opportunity to enter a prize draw to win one of eight £50 electronic shopping vouchers.
The final sample comprised 121 people (see Table 1) aged 18–88 (mean [M] = 45.50, standard deviation [SD] = 13.86), with most diagnosed as autistic (n = 100, 82.6%). A breakdown of participant age ranges can be found in Table 1. The majority of participants had a degree (n = 93, 76.9%), and just over half were employed full- or part-time (n = 67, 55.4%). Participants in the sample had a mean of 4.74 (SD = 2.75, median = 4.00) health conditions or neurological differences. This ranged from 0 condition (n = 2) to a maximum of 15 conditions (n = 1). The most prevalent being anxiety (n = 71, 58.7%), depression (n = 59, 48.8%), and being overweight/obese (n = 46, 38.0%). Forty-four participants (36.4%) reported having attention-deficit/hyperactivity disorder.
Participant Demographic Characteristics
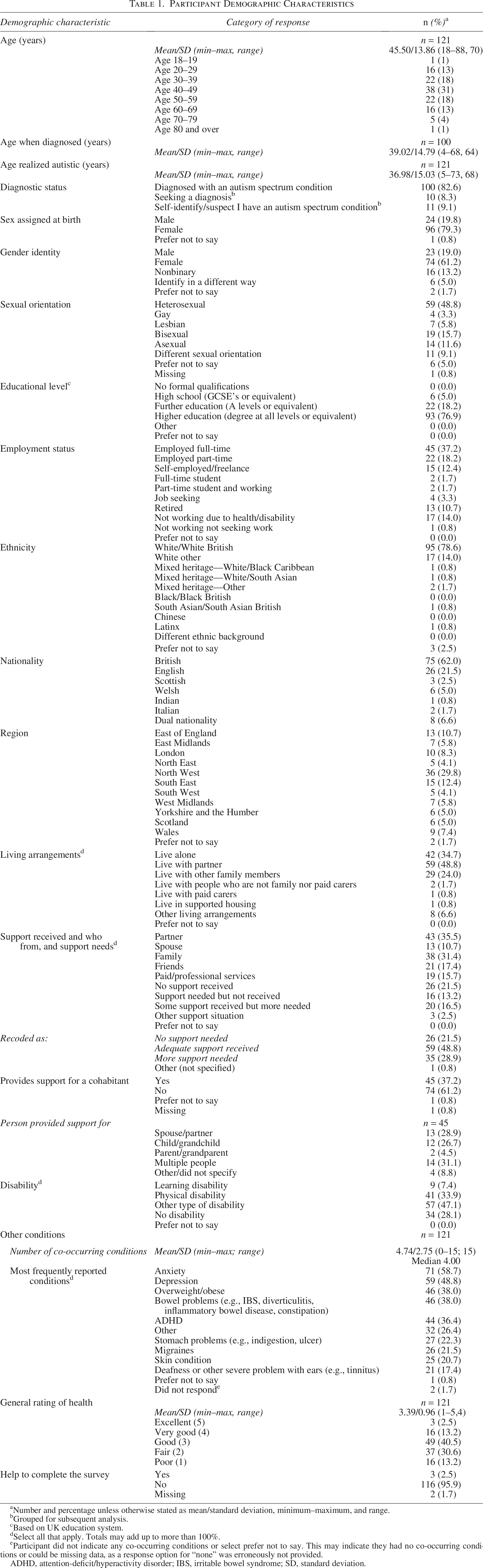
Number and percentage unless otherwise stated as mean/standard deviation, minimum–maximum, and range.
Grouped for subsequent analysis.
Based on UK education system.
Select all that apply. Totals may add up to more than 100%.
Participant did not indicate any co-occurring conditions or select prefer not to say. This may indicate they had no co-occurring conditions or could be missing data, as a response option for “none” was erroneously not provided.
ADHD, attention-deficit/hyperactivity disorder; IBS, irritable bowel syndrome; SD, standard deviation.
In response to a question about disability, some participants provided free-text comments about whether being autistic is a disability or not (Supplementary Data SA1). Reports of support given and received varied considerably, with people receiving support from friends and family, using paid/professional support, or not receiving any support (see Table 1). Seven participants stated they provided support for a person who also supported them (reciprocal support), and six participants stated they supported someone who lived elsewhere (e.g., an elderly relative). See Supplementary Data SA1 for further information about support.
Materials
Survey development
We created a list of candidate survey questions that included a number of open questions about aging. We circulated these to members of the Autism@Manchester Expert by Experience group, who provided feedback at an online meeting. Group members made the following suggestions: include reference to autistic people who support others in the demographic questions; remove two questions that asked about people who are aging well or not aging well, as these would be difficult to answer; add more concrete response options because the questions were too open; and add a question about whether autism has become easier or more difficult to cope with over time. We implemented all of these suggestions.
To provide more concrete response options, we added specific items for people to respond to when considering questions about doing well in older age and worries about aging. We compiled an initial list of these items based on our discussion with the Autism@Manchester Expert by Experience group and from the findings of a recent qualitative study on this topic. 9 We have summarized pertinent findings from this qualitative study in the introduction to the present article. This initial list comprised 28 items that could help people to do well in older age and 17 items that could worry people about older age. We circulated a draft of the survey, including these items, to the Autism@Manchester Expert by Experience group. We asked group members for feedback if they thought the worry items duplicated the doing well items and if they thought any items should be removed. Everyone who fed back said that no items should be removed. Some group members suggested additions, including items on work (paid, voluntary, support from managers, and occupational health) and items on sex life and menopause. The final list therefore comprised 35 items about doing well in older age and 17 items related to worries about aging. We made other changes to the survey based on feedback, including revising the participant information and instructions to be clearer and adjusting the survey structure and order of items.
Survey items reported in this article
The final survey was hosted via Qualtrics survey software and comprised demographic questions, open (qualitative) and closed (quantitative) questions about aging, and an open response question about future research topics. The questions cover three sections that address our study aim: aging well, changes in experiences of being autistic and aging, and research priorities. Participant demographics and findings from the questions listed in Box 1 are reported in this article.
Aging Well
(Closed question) Below you will find a list of items that some autistic people have said are helpful for doing well in older age. These items are based on the findings of a related study that interviewed older autistic adults, as well as discussions with autistic people advising on this project. Please tell us how important each item is to you. Thirty-five items were listed (“doing well items”; see Table 2) and response options were very important/fairly important/neither important nor unimportant/not that important/not important at all/prefer not to say (Open question) Is there anything not listed above that you think could be helpful for doing well in older age? If you have any comments on the above list of items you can also add those here. (Closed question) Below you will find a list of items that some autistic people have said might worry them in older age. These items are based on the findings of a related study that interviewed older autistic adults, as well as discussions with autistic people advising on this project. For each item, please tell us how much you agree (or not) that this item might worry you in older age. Seventeen items were listed (“worry items”; see Table 3), and response options were: completely agree/somewhat agree/neither agree nor disagree/disagree somewhat/disagree completely/prefer not to say (Open question) Is there anything not listed above that you think could worry you in older age? If you have any comments on the above list of items you can also add those here.
Changes in Experiences of Being Autistic and Aging
(Open and closed question) Thinking back over your life so far (whatever age you are now), has your autism become easier or more difficult to cope with as you’ve got older? If you would like to explain your answer, please leave any comments here. Participants were given a 5-point Likert scale with the following response options: much easier to cope with/a bit easier to cope with/about the same/a bit more difficult to cope with/much more difficult to cope with.
Research Priorities
(Open question) What topics related to aging are the most important to you, that you might like us to look at?
Procedure
The study was reviewed and approved by the University of Manchester Research Ethics Committee 2 (ref: 2023-16770-29474, 07/06/2023). Participants completed an online informed consent form prior to commencing the survey. After mandatory questions about age and diagnosis, questions either had a “prefer not to say” option or could be left blank if participants did not wish to answer.
To ensure the data were valid, we took the following steps: we used the “Bot detection” function in Qualtrics survey software to identify potential bots. This uses invisible reCaptcha technology, and all participant scores were 0.5 or above, indicating participants were likely human. All except five participants responded to the open questions in the survey. Three of our team (K.B., D.B., and L.H.) reviewed the qualitative responses, and we agreed the content suggested they came from genuine autistic participants. The five participants who did not respond to the open questions provided free-text responses to demographic questions. We (C.R. and K.B.) agreed the content of these responses suggested the participants were genuine.
Helpful Items for Doing Well in Older Age (Doing Well Items): Response Frequencies and Correlation Between Item and Age (N = 121)

Significant findings are shown in bold.
p ≤ 0.05, **p ≤ 0.01 (two-tailed).
CI, confidence interval.
Items That Could Worry People in Older Age (Worry Items): Response Frequencies and Correlation Between Item and Age (N = 121)
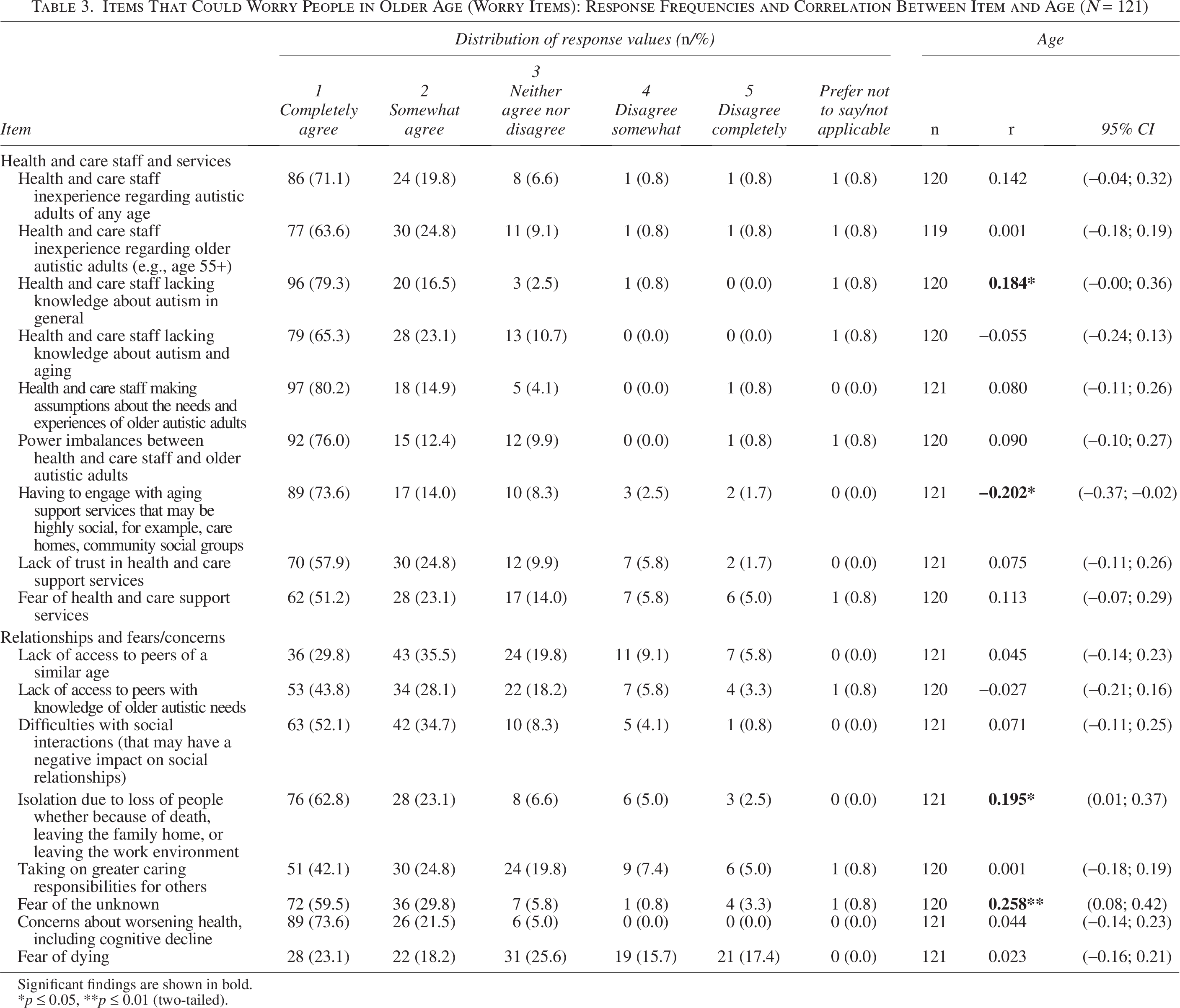
Significant findings are shown in bold.
p ≤ 0.05, **p ≤ 0.01 (two-tailed).
Data analysis
We conducted a quantitative analysis of data from closed questions using SPSS v28.0.1.1. We describe data using frequencies, percentages, range, mean, and SD where appropriate. Data were not normally distributed and resisted transformation. Therefore, we used Spearman’s correlation tests to explore the relationship with age for questions 1 (doing well items) and 3 (worry items).
We analyzed free-text responses descriptively using inductive qualitative content analysis, following the three phases described by Elo and Kyngas. 24 In the preparation phase, authors L.H., D.B., and K.B. read and reread the survey responses to become immersed in the data. We then discussed the participant demographics and example quotations with autistic stakeholders to inform the interpretation of the data and development of categories. In the categorization phase, we openly coded the data, question by question, at the manifest level, and then grouped the codes into categories. K.B. and D.B. discussed and refined the categories and then discussed these further among the wider research team. This was to assess the face validity of the categories. 24 In the reporting phase, we selected quotations to illustrate the categories. Returning to the categorization phase, we (K.B. and D.B.) discussed the categories and supporting quotations with team members and autistic stakeholders and further refined them. We then reviewed the codes and categories across questions, refined the categories further, and discussed these with the team before finalizing the report. In line with Elo and Kyngas, 24 we ensured the trustworthiness and reliability of the data by returning to the data several times and discussing the categories with team members and autistic stakeholders. K.B. and D.B. made the final decision on category names after reaching a consensus through discussion.
Results
We present the results in three sections: aging well (results from questions 1–4); changes in experiences of being autistic and aging (results from question 5, reported here and continued in Supplementary Data SA1); and research priorities (results from question 6). Throughout this section, we use italics to indicate the results sections, a survey question, item, or response option. Participant quotes are in quotation marks.
Aging well
In this section, we report findings from closed questions (1 and 3) and findings from open questions (2 and 4; Box 1). Analysis of responses to open questions generated three categories, which are described after the quantitative findings.
Survey participants rated most items that were listed as being potentially helpful for doing well in older age (question 1) as fairly or very important (see Table 2). We found significant correlations between age and importance for five of the items: having healthy, positive, social relationships with people you interact with at your own pace online [rs(119) = −0.209, p = 0.02]; being as physically healthy as possible [rs(119) = −0.293, p = 0.001]; maintaining cognitive health for as long as possible [rs(117) = −0.186, p = 0.04]; having good mental health [rs(119) = −0.228, p = 0.01]; and being able to cope with changes that come up with your physical, cognitive, or mental health [rs(117) = −0.258, p = 0.005]. For these items, importance ratings increased with increased age.
Most participants agreed that the items that were listed as being potentially worrying about older age (question 3) could be somewhat or completely worrying (see Table 3). The main exception was for the item fear of dying. Fifty participants (41%) agreed completely or somewhat that this could be worrying, 40 (33%) disagreed completely or somewhat, and 31 (26%) neither agreed nor disagreed that fear of dying could worry them in older age.
We found significant correlations between age and how much people were worried about four of the items. The item having to engage with aging support services that may be highly social, for example, care homes, community social groups felt more worrisome with increased age [rs(118) = 0.184, p = 0.05]. The following items were less worrisome with increased age: health and care staff lacking knowledge about autism in general [rs(119) = −0.202, p = 0.03]; isolation due to loss of people whether because of death, leaving the family home or leaving the work environment [rs(119) = 0.195, p = 0.03]; and fear of the unknown [rs(118) = 0.258, p < 0.01].
Forty-five participants provided free-text comments in response to the follow-up question about what helps people to do well in older age (question 2). Forty-five participants left free-text comments about what might worry people in older age (question 4). We generated three categories from analysis of these comments: (1) health, care, and wider societal support; (2) independence and autonomy; and (3) social connectedness. We found no apparent differences in the patterns of response by participant age. Information in parentheses indicates participant ID number, age, and gender identity (M = male; F = female; NB = non-binary; D = different gender identity; and P = preferred not to state gender). Additional supporting quotes can be found in Supplementary Data SA1.
Health, care, and wider societal support
This category describes participant concerns about changes in health, the quality and suitability of healthcare, healthcare staff, and support and understanding from across wider society.
Participants highlighted the need for support throughout the lifespan, including for autistic people who may have caring responsibilities for older or younger autistic family members. It was thought provision of information about aging and health-related changes (e.g., menopause) could help to alleviate fears about aging in some autistic people: “I think more information for ‘autistic’ people specifically regarding the menopause and aging would be helpful as it can feel a bit scary and overwhelming sometimes” (M024, 40, F). Participants expressed concerns about a decline in health as they aged, particularly in physical and cognitive health: “Health wise my biggest fear is losing my sight, and losing capacity enough to know I’ve lost it, or losing enough memory that the world is scary because I don’t know where I am, who people are, who I am” (M041, 55, F). Neurodegenerative conditions were a particular concern, and some participants were afraid of the impact on gender identity and gender-affirming care: “My biggest fear is dementia, and forgetting why I transitioned” (M115, 74, F) and “Being without access to essential medication resulting in detransitioning” (M034, 43, NB).
Participants expressed concerns about the quality and suitability of healthcare. This included concerns about accessing timely care, communicating healthcare needs, and the suitability of screening services: “Having uncontrollable pain and not being able to get timely care or fight for/communicate my needs” (M077, 49, NB). And “Cancer screening services which account for autism. Mammograms and cervical cancer screening are not something I can tolerate. I feel judged, excluded and discriminated against for not being able to access them and it can only have a detrimental effect on my health. The NHS has a monolithic and inflexible approach—I speak as a very senior manager in the service” (M038, 60, F). This extended to hospital care and the impact on end-of-life care: “Dying I’m not afraid of. The method of dying and the potential for being forced to stay in hospital (which is pure torture) in addition to being in great pain and having other horrors and indignities inflicted on mind and body—all those things terrify me” (M013, 61, D). This pragmatic approach to death may explain the variation in attitudes to death from the quantitative findings. The manner of death and lack of suitable end-of-life care rather than a fear of death itself may be worrisome.
Participants highlighted the lack of understanding about autistic people among healthcare staff: “Would like healthcare staff to have a better understanding of autism—starting with the realisation that it doesn’t mean I have a learning disability!” (M023, 61, M). It was felt a lack of understanding could lead to “masking” aspects of identity: “The discomfort of externally provided support work often means autistic masking, tolerating expressed attitudes and outlooks from staff that are bigoted, or incorrect” (M081, 51, P). This reflects the quantitative finding that the survey item health and care staff having good knowledge about the needs of older autistic adults was rated very or fairly important by 117 participants (97%). Participants expressed fears about being reliant on staff, and the challenge of recruiting and retaining good quality care staff was seen as leading to inconsistent and unpredictable care: “What I fear (at any life stage) is having to be dependent on staff. It’s complete pot luck, hit or miss. I don’t see the pay rate attracting people with a largely compatible life view, at least not in a longer term basis. Care is like a job of last resort. Bad care and lack of power to challenge detrimental practice is what I fear most” (M100, 41, D). Power dynamics were a concern too, with fears of abuse from staff: “Being abused by professionals. It already happens now when I have full capacity so being more vulnerable is frightening” (M109, 40, F). This reflects the quantitative finding that 107 participants (89%) somewhat or completely agreed that the survey item power imbalances between health and care staff and older autistic adults could be worrying in older age.
Participants also expressed concerns about intersectional needs not being recognized or respected by health and care staff. It was thought this could have a detrimental impact, particularly if people have experienced past difficulties with acknowledging and expressing their gender, sexuality, and/or neurodivergence. As the quote in the title of this article indicates, participants wanted to be seen and respected as whole individuals: “Many of us are gender fluid and have grown up in a time when that was actively repressed or even illegal. Coming to terms with gender, sexuality and neurodivergence is very difficult and often traumatic against that background. We are now faced with a future in which expressing requirements for understanding of autism and gender from health care staff is heavily politicised. … Our existence as whole individuals does not evaporate at age 50” (M038, 60, F).
Beyond healthcare participants thought that information for organizations across society including employers and Occupational Health departments, could help to better support autistic employees, customers, clients, and freelance workers: “My experiences at work since disclosing my autism have been absolutely awful. … I have been appalled at how bad it has been trying to get reasonable adjustments, and the total lack of knowledge of our Occupational Health service about autism. The line manager being interested, willing to learn, and supportive is vital” (M073, 44, F). Some participants highlighted that autistic people who live independently are in need of support, but this may not be readily available or suitable: “Services for autistic people are poor and designed for the priorities of neurotypical people. They seemingly think all autistic adults are on benefits or renting and have no appropriate services for people in work, people struggling to manage their own house or pensions or anything like that. Help is only available privately and is very expensive. I have zero confidence in some neurotypical ‘advocate’ being of the slightest help” (M008, 56, F).
Independence and autonomy
This category describes participants’ fears about losing independence and autonomy, and their suggestions for supporting independence and autonomy. These qualitative findings reflect the quantitative finding that 116 participants (96%) rated the survey item having autonomy—being able to act on your own values and interests as fairly or very important.
Fears included losing financial independence: “Financial vulnerability and coping badly with an overwhelming benefits system” (M043, 59, F) and fears about who would make decisions in relation to capacity: “Worry about who would make decisions about my capacity, and if I did not have capacity due to e.g., dementia who would make those decisions around my care and finances” (M062, 36, NB). Participants expressed concerns about not being able to remain in one’s own home, the suitability of care homes, and the impact of this on autonomy: “The main thing that worries me about ageing is the possible future prospect of not being able to look after myself in my own home. I’ve visited several care homes and I don’t think I could tolerate living in anything I’ve seen. Too many people, too much noise, enforced communal living, etc.” (M101, 58, M). Participants raised concerns about no longer being able to do, or being prevented from doing, things they enjoyed and that brought joy and being prevented from keeping valued possessions: “Being prevented from having the things I value because someone in a position of power can’t see why I value them. This could be things like pets, but also specific items, tools or sports equipment. Being made to sell bikes I designed and made because I can’t ride them anymore would be heartbreaking but is very common” (M005, 33, M).
Participants considered access to transportation and support with communication as being helpful for retaining independence and autonomy: “Access to public transport/the ability to drive safely still” (M117, 36, F) and “Help with communication, verbal, writing, other types of communication” (M112, 40, F). Participants thought support from professionals such as Occupational Therapists could help: “Access to nd [neurodivergent]/autism specific supported living services—or the sort of OT [Occupational Therapist] that would allow someone to retain independence/remain in their own home with familiarity as long as possible. New environments are hard for autistic people to settle into so being moved in and out of home/hospital/residential care would be distressing and leads to worse health outcomes across all factors” (M042, 40, NB). Participants suggested retirement communities specifically for autistic people could be a way to support independent living and offer privacy as well as provide peer support: “Relationships with neighbours can be very challenging. I would really like the option of being co-located close to other autistic people in some kind of intentional community where we could have separate living space and privacy but peer support when needed” (M070, 63, NB). Participants also suggested that autistic people are supported to prepare advance directives and related documents and have these wishes respected by health and social care staff: “Health and Social Care staff honouring wishes in advance directives, advance statements and power of attorney documents” (M109, 40, F).
Social connectedness
In this category, participants described the importance of social and digital inclusion, and fears of isolation and a lack of support. Participants felt that social contact with autistic people across age ranges, and based on interests, was important for doing well in older age: “Access to socialising based on needs rather than age and diagnoses. Being able to socialise with people with common interests” (M044, 54, M) and “Having social groups to access, helping to reduce loneliness” (M065, 30, F). Participants also considered having meaningful ways to spend time to be important. This included activities that stimulate the mind and physical activities in suitable environments: “Access to lifelong learning and suitable enjoyable physical activities” (M111, 40, NB) and “Access to quiet safe spaces” (M063, 67, F). This reflects the quantitative finding that 116 participants (96%) rated the survey item being able to do things you enjoy as very or fairy important for doing well in older age.
Participants described a range of important relationships and the role of technology in supporting these: “texting relationships are far more relevant as that is how I communicate with most people, but the small number of in person relationships I have are also very important” (M069, 37, F). While some participants thought that technology could support social connections, some feared that it could also be a barrier and that it was important that people were supported to use it: “Access to technology and support to learn about and use it” (M005, 33, M), and “Technology presenting too many barriers” (M033, 40, M).
Participants also expressed concerns about not having family members and feeling isolated or lacking support in older age as a result: “Not having any family at all. No one caring. It’s terribly frightening to think about” (M026, 56, D). Some of those who did have family were concerned about how their family members would be supported after they died: “Support for my autistic daughter—after I have died, how will others be able to support her needs” (M040, 41, F). Some younger survey participants indicated they were experiencing loneliness already: “I live in constant dread. I feel like my life goes nowhere. I’ve been cheated on, taken advantage. … I am very lonely I have a handful of friends and of them I rarely see them if at all. Life is hard” (M108, 28, M). This may explain the quantitative finding that the survey item isolation due to loss of people whether because of death, leaving the family home or leaving the work environment was more worrisome for younger participants.
Changes in experiences of being autistic and aging
In response to the Likert-scale question Thinking back over your life so far (whatever age you are now), has your autism become easier or more difficult to cope with as you’ve got older? (question 5), 23 participants (19%) said this was about the same, 52 (43%) said this was a bit easier or much easier, and 46 (38%) said a bit more difficult or much more difficult. There was no statistically significant correlation between responses and age [rs(119) = −0.158, p = 08 (−0.33; 0.03)]. Ninety-six participants left free-text comments to explain their response. Participants described developing greater self-understanding and awareness, either as the result of a diagnosis in later life or as a result of aging and getting to know themselves better. Participants also described the challenges of trying to fit into a neurotypical society, including the impact of societal demands, poor treatment from others, and the toll of long-term masking. Participants highlighted negative impacts of life changes in relation to being autistic, such as bereavement and the loss of family support, menopause impacting the ability to mask, and sensory sensitivities worsening with age. The full results of the qualitative analysis, including response categories and supporting quotations, can be found in Supplementary Data SA1.
Research priorities
Participants were asked to suggest topics related to aging that they considered important for future research (question 6). Ninety-five participants responded, and we generated nine categories from the comments: healthcare services and staff, specific health conditions and concerns, needs and concerns specific to being autistic, social life and support, independent living, intersectionality, abuse and discrimination, social care and other support services, and cross-cutting concerns. Some participants made multiple suggestions, which fit into several different categories. Category descriptions and supporting quotations can be seen in Table 4.
Research Priorities Suggested by Participants, Qualitative Findings

Information in parentheses indicates participant ID number, age, gender identity.
M, male; F, female; NB, non-binary; D, different gender identity; P, preferred not to state gender.
Discussion
In this study, we used a codesigned mixed methods survey to explore experiences, support needs, and research priorities related to aging in a diverse group of autistic adults. We generated important insights about what autistic adults across a range of ages think would help them to do well in older age, what worries them about older age, and changes in experience of being autistic with aging. We also identified topics for future research from participant responses.
Physical and mental health
In line with existing research,1,7 participants reported a high prevalence of physical and mental health conditions. The most frequently reported conditions were anxiety and depression. Minority stress may contribute to poor mental health, 15 and participants in our study described a lack of support and experiences of stigma, discrimination, and abuse, which are in line with this model. Indeed, participants recommended future research should focus on abuse and discrimination and its impact on autistic people. The impact of minority stress may be even more marked for people with additional intersecting identities, who may experience multiple marginalization. Our sample included people identifying as non-binary and people with a range of sexual identities. The need to be recognized and accepted as whole individuals was highlighted in our qualitative findings, reflecting this diversity within our sample. Importance ratings for the item having good mental health increased with age, indicating older respondents thought this was particularly important for doing well in older age. The qualitative data did not fully explain this finding, as there were no apparent differences across participant comments by age. However, it may be the result of older participants reflecting on a lifetime of minority stress and masking, and late diagnosis for some. In the 100 participants diagnosed as autistic, the mean age at diagnosis was 39 years old. Atherton et al. 16 reported later diagnosis is associated with poorer mental health and quality of life, and this could be a contributory factor in our findings. It should be noted, however, that Atherton et al.’s 16 study has been criticized for not controlling for additional variables aside from age of diagnosis. 25 In their study of 300 autistic adults, Leung et al. 25 found that poorer quality of life was predicted by having more autistic traits and other factors such as mental health conditions. They also reported an association between better quality of life and an earlier diagnosis of autism, which is in line with Atherton et al. 16 and, as above, could help to explain our findings.
Social and digital inclusion
Novel findings from this study that were not identified from the previous qualitative study on this topic 9 relate to social and digital inclusion, particularly around technology. Technology was seen as being useful for helping people to live independently and to facilitate social connectedness. This is supported by literature, which suggests that technology can help mitigate against loneliness. 26 However, it was emphasized that people may need support to keep up with changing technologies, and having a variety of means to facilitate social connectedness is important.
Our findings on the importance of social connectedness support existing research relating to non-autistic older adults and autistic adults across age ranges. For example, research in the general population has found social isolation from friends can negatively impact the mental health and quality of life of older adults.27,28 Older autistic adults report experiencing loneliness and a longing for connection, 17 and social inclusion is important for suicide prevention in autistic adults. 29 A recent systematic review reported associations between autistic–autistic contact and several domains of quality of life. 30 Furthermore, engaging with autistic peers can support the development of autistic self-identity. 20 This is important because having a positive personal and social autistic identity is associated with improvements in aspects of psychological well-being and mental health.31,32 In line with these findings, support for social inclusion in older age was suggested as a priority for future research by our participants. Along with social connections, participants highlighted meaningful ways to spend time as important. However, it should be noted that what is considered meaningful will differ across individuals. Individual differences should be acknowledged and respected in order to support autonomy and well-being. Indeed, Watts et al. 30 noted individual differences and suggested that autistic contact with other autistic people, while undoubtedly important, should not be considered a panacea.
Independent and autonomous living
Both the quantitative and qualitative findings of this study highlighted the importance of support to live independently and autonomously. This included remaining in one’s own home, as well as retaining autonomy within a care home setting. This reflects the findings of research with autistic and non-autistic adults.9,13 For example, in a study of 1514 non-autistic adults aged 30+, almost 90% of the survey respondents said they would prefer to stay in their own home. 13 While this seems to be a universal issue for autistic and non-autistic populations, participants in our study raised specific concerns relating to being autistic. For example, participants expressed concerns about the sensory environment of a care home, and about care home staff lacking knowledge about autistic people, not understanding their sensory needs, and infantilizing them. There is currently a paucity of research regarding autistic adults’ experiences of care homes. Topics that have been highlighted as key priorities for future residential care research have included autism training for residential care staff, recognizing and respecting autistic differences and understanding autistic well-being, the sensory environment and sensory processing, and autonomy and choice. 14 Participants in our study suggested researching similar topics, such as adaptations to environments including care homes, and training for staff in a range of settings, again including care homes. A novel finding from our study was the suggestion of retirement communities specifically for autistic older adults. Participants thought this could offer privacy and independent living while also offering peer support and opportunities for socializing when needed and wanted. Retirement communities based around an affinity group already exist, for example, there are LGBTQ+ retirement communities across Europe and the United States, with long waiting lists for accommodation. 33 The potential for similar communities for older autistic adults could be worthy of further research.
Aging-related health changes, cognitive decline, and support plans
Participants in this study were concerned about aging-related health changes and the lack of information available to them. Menopause and neurodegenerative conditions such as Parkinson’s and dementia were a particular concern. Participants suggested information could help assuage people’s fears and help them to manage these health issues. This builds on the findings of a previous qualitative study, in which participants expressed similar concerns, including a perceived greater risk of dementia. 9 The current evidence is unclear as to whether autistic people are more or less likely to experience dementia.1,10,11 However, recent research reported increased rates of cognitive decline in middle and older age autistic adults compared with non-autistic adults, which could be a risk factor for future mild cognitive impairment or dementia. 8 Relatedly, participants in this study were concerned about capacity and decision-making should there be a loss of capacity. Participants highlighted the need for health and care staff to honor advance directives, advance statements, and power of attorney documents as something that could support people to do well in older age. More research is needed regarding the risk and prevalence of dementia, as well as how autistic people experience dementia and how they can best be supported.
Survey participants suggested the recording of future support plans as a research priority (in the category Social care and other support services). Support plans could include descriptions of what dysregulation (e.g., shutdown and burnout) looks like for an individual so that appropriate support can be provided. This could be important as ways of processing distress and the time needed to do so may be different among autistic and non-autistic individuals. 34 Participants also referred to fluctuating needs and difficulties in the research priority about staff training and in descriptions of being autistic as a fluctuating disability (see Demographics section, Supplementary Data SA1). Participants described support needs that vary at different points in time and under different circumstances. Such descriptions are in keeping with the “Episodic Disability Framework,” originally developed to conceptualize experiences of disability from the perspective of people living with HIV. 35 Uncertainty is a key component of episodic disability, and the term was coined to account for the fluctuating and inconsistent nature of disability as experienced by people living with HIV. The framework consists of three main components, which describe (1) dimensions of disability, (2) contextual factors, and (3) triggers of major episodes of disability. 35 The Episodic Disability Framework would be worthy of investigation to see if it could be applicable (or not) for autistic people and whether it could help to inform support and care.
Changes in experiences of being autistic and aging and research priorities
Regarding changes in experiences of being autistic over time, participants described a range of different experiences: positive, negative, and little change. The experiences described in our study reflect those of existing research9,17 and speak to the importance of holistic approaches to support autistic people throughout the lifespan. Intergenerational peer support may be helpful so that experiences and learning from older autistic people can be used to inform and support younger autistic people as they age. Indeed autistic peer support can have a positive impact on several domains of quality of life. 30 The changing experiences described by participants point to directions for future research and reflect some of the research priorities suggested by participants. These included stigma and discrimination, improving understanding of others, intersectional identities, adjustments and adaptations, access to appropriate healthcare, and physical and mental health. These topics are similar to priorities identified by autistic adults in relation to employment research, 36 topics relating to research on the intersection of transgender and non-binary identities, 37 and research priorities identified by autism community members across domains. 38 There are also similarities with research priorities identified for other groups of older adults. For example, research priorities identified for older adults living with HIV include social participation, engagement and relationships, and the role of digital technologies to support healthy aging. 39 This indicates common needs and concerns across autistic and non-autistic populations in relation to aging.
Strengths and limitations
Autistic people were involved at all stages of this research, including development of the survey, interpretation of the data, and writing up the findings. This helped to ensure the study focused on issues that matter to the autistic community.
Participants in this study were diverse in terms of sexual orientation and gender identity. Almost 50% of participants identified collectively as gay, lesbian, bisexual, asexual, and a “different sexual orientation” (not heterosexual). Over 60% of participants identified as female (79.3% assigned female at birth). This higher prevalence of female respondents is similar to other online surveys of autistic adults.15,40 In contrast, this is a strength, as the experiences of autistic women have historically been under-represented in autism research. However, this can also be considered a limitation as our sample does not reflect the wider autistic population. Almost 20% of participants identified as nonbinary or a different gender identity. This was not seen in the previous qualitative study on this topic, 9 perhaps due to the smaller sample size, and reflects the higher rates of gender diversity reported in autistic populations.41–43 In addition, our study included participants who self-identified as autistic, whereas the previous qualitative study did not. This led to a range of experiences and opinions being expressed, including needs around intersectionality and gender-affirming care.
Participants were entirely United Kingdom based, so findings may not be transferable to autistic adults in other countries. Most participants (78%) were educated to Bachelor’s degree level or higher, which may not be representative of the autistic population. People from minoritized ethnic backgrounds and autistic people with learning disabilities were under-represented, which may mean that certain experiences and priorities for future research may not have been captured in this study. The study included participants with a range of ages (18–88), so it should be noted that the concerns, experiences, anticipated support needs, and research priorities in relation to aging identified in this study reflect those of autistic adults generally and not exclusively older adults. In addition, we generated the research priorities from categorizing free-text comments from participants rather than following an established framework for research priority setting, as used in other autism research 44 and described by Deering et al. 45 This limits the robustness of the conclusions that can be made.
Our methods of recruitment and data collection would have impacted the sample of participants in this study. For example, participants were self-selecting and recruited via digital methods (email, social media, and online community groups), which means participants needed to be connected to particular networks and would have needed a certain level of digital literacy to find out about the survey as well as take part. The recruitment and data collection methods favored those who are comfortable using digital technology to communicate, and who could understand and respond to the types of questions asked, in the format they were presented. This may explain the high levels of education in participants in this study.
Conclusions
This study contributes to the growing evidence base describing the aging-related experiences and needs of autistic individuals. The findings highlight a number of universal concerns that are relevant to quality of life for older adults generally, reflecting the shared experiences of autistic and non-autistic older adults. These findings help to validate the experiences, hopes, and fears of autistic individuals and provide evidence to help people advocate for their needs. Our findings build on recent qualitative research and highlight underexplored areas such as care home experiences, dementia, menopause, and LGBTQIA+ aging needs. Novel findings include the suggestion of autistic retirement communities and the role of technology as a potentially useful tool for support. Findings will help to inform health and care provision in order to support autistic adults to do well in older age, as well as directing future research in line with priorities of the autistic community. Future work could involve refining and prioritizing the topics for future research identified in this study using an established framework for research priority setting. 45
Footnotes
Acknowledgments
The authors would like to thank the individuals who contributed to the design and development of the project including members of the Autism@Manchester Expert by Experience group, along with Benjamin Thompson for assisting with the early setup of the project, and all of the study participants for giving their time and sharing their thoughts and experiences.
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
This article presents independent research funded by the
Authorship Confirmation Statement
K.B. and C.R.: Conceptualization, funding acquisition, methodology, formal analysis, writing—original draft, and writing—review and editing. D.B.: Conceptualization, funding acquisition, methodology, formal analysis, and writing—review and editing. E.G., L.J.E.B., and E.C.: Conceptualization, funding acquisition, methodology, and writing—review and editing. L.H.: Formal analysis and writing—review and editing.
Disclaimer
The views expressed are those of the authors and not necessarily those of the National Institute for Health and Care Research or the Department of Health and Social Care.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.