
Abstract
Background:
Adaptive behavior skills are a significant predictor of adult outcomes. However, few studies have examined developmental trajectories in autistic individuals from early childhood into mid-adulthood and how these trajectories are associated with adult outcomes.
Methods:
This study uses a longitudinal sample (n = 266) to investigate age-related adaptive behavior developmental growth trajectories across ages 1–55 years. The study investigated clinic records, including questionnaires, interviews, and diagnostic assessments. Caregivers completed the majority of questionnaires.
Results:
A linear spline model best fits the data, suggesting that from early childhood to young adulthood (ages 1–20; autistic individuals gained adaptive behavior skills, but scores declined from young adulthood to mid-adulthood [ages 21–55]). Higher IQs and fewer clinician-endorsed autism characteristics across childhood into mid-adulthood were associated with greater adaptive behavior skill growth over time. Caregiver reports of a higher quality of life and daily living skills in adulthood were related to adaptive behavior growth over time.
Conclusion:
Overall, the growth of adaptive behavior skills is positive from young childhood to young adulthood but begins to decline during adulthood. It appeared that there was a potential decline in adaptive behavior towards mid-adulthood. Results confirm the importance of adaptive behavior in caregiver perceptions of quality of life for autistic adults and suggest adaptive behavior is essential to support throughout the lifespan.
Community Brief
Why is this an important issue?
Adaptive behavior skills are tasks that support an individual in their everyday lives. Autistic individuals often have difficulties with these skills from childhood to adulthood, regardless of their cognitive skills. There is not much longitudinal research measuring adaptive behavior beyond young adulthood.
What was the purpose of this study?
The study aimed to look at how adaptive behavior changes from childhood to mid-adulthood and how the quality of life, experiences in employment and postsecondary education, and cognitive skills such as flexibility, memory, and organization support adaptive behavior skills in adulthood.
What did the researchers do?
The researchers analyzed data from a sample of 266 autistic individuals who lived in North Carolina. Some participants had first been diagnosed with autism spectrum disorder in the late 1960s–1970s at the University of North Carolina TEACCH Autism Program. Participants had multiple evaluations done over time in the clinics. A follow-up survey was sent to caregivers for autistic adults diagnosed before 2000 and who were ages 21–55. Caregivers reported on the autistic adults’ daily life activities, such as if they had jobs or went to school and where they lived. The researchers measured changes in adaptive behavior skills in early childhood (age 1 year) into adulthood (age 55). The researchers also examined the relationship between adaptive behavior, daily activities, quality of life, and participation in employment and postsecondary education.
What were the results of the study?
In this sample, autistic individuals gained adaptive behavior skills from early childhood to adulthood. They gained adaptive behavior skills at a slower rate once they turned 21, and abilities may have declined into later adulthood. Individuals with higher IQs and fewer clinician-rated autistic traits from childhood to adulthood made higher gains in adaptive behavior. Caregiver reports of adaptive behavior during childhood (ages 1–20) were related to a higher quality of life, higher daily living skills, and more vocational or educational experiences in adulthood. Caregiver reports of a higher quality of life and higher daily living skills were related to adaptive behavior skills gained during adulthood (ages 21–55).
What do these findings add to what was already known?
Longitudinal research on adaptive behavior across the lifespan is limited. Less is known about how the growth of adaptive behavior skills is related to quality of life and what predicts adaptive behavior skill growth during adulthood. This study has provided helpful information on how adaptive behavior changes across the lifespan.
What are the potential weaknesses in the study?
The majority of adaptive behavior measures were from caregiver reports; thus, the study lacked self-report measures.
How will these findings help autistic adults now or in the future?
The findings in this study identified how important adaptive behavior is for autistic adults. Adaptive behavior during childhood was related to quality of life, daily living skills, and vocational and educational experiences in adulthood. Adaptive behavior growth during adulthood was related to quality of life and daily living skills, suggesting the importance of supporting adaptive behaviors across the lifespan and continuing into middle adulthood. Furthermore, we hope that caregivers and clinicians will work to consider the priorities of autistic adults with whom adaptive behaviors may be targeted.
Background
Adaptive behavior is a critical indicator of employment, living situation, overall health, and quality of life in autistic adults, especially in middle and older age, ages 25 and greater.1–3 Adaptive behavior is defined as conceptual, practical, and social skills to support an individual’s everyday life, which is age and context-specific, representing different demands across development and getting more complex in adulthood.4–8 One of the most used measures of adaptive behavior skills from birth to older adulthood is the Vineland Adaptive Behavior Scales, which includes communication, socialization, and daily living skills.9–11 Communication includes receptive, expressive, and written skills related to comprehension and providing information. Socialization includes individuals’ relationships with others, leisure time, and coping skills. Daily living skills include personal, domestic, and community skills such as hygiene, cooking, cleaning, and managing finances. 9 While the importance of adaptive behavior has been well documented in autistic children and young adults (ages 2–25),12–17 there is less research on adaptive behavior in autism in middle and older adulthood from ages 25 and older. However, limited research suggests that better daily living skills in middle-aged and older autistic adults are associated with employment and postsecondary outcomes such as having a paid job or being in school1,18,19 and independent living,1,18 in addition to having a good quality of life, 18 better overall physical health, 3 and better mental health outcomes.2,20 Challenges with daily living skills are associated with increased anxiety and depression in autistic young adults 20 and increased stress in middle-aged and older autistic adults. 2
Many autistic individuals experience difficulties in adaptive behavior throughout their lifespan regardless of their intellectual functioning,20,21 and adaptive skills are frequently reported as below age expectations throughout adulthood.20,22,23 Differences between adaptive skills and intellectual functioning are known as a gap between IQ and adaptive skills, with the gap increasing with higher IQ 13 and over time.24,25 Given that IQ is not a reliable indicator of independence or support needs in autistic adults with average or above average intelligence,26,27 adaptive behavior may better represent the consistency of an individual’s skills and support needs.
Given the importance of adaptive behavior and daily living skills in predicting functional outcomes for autistic adults and being more reflective of independence, the current study focused on adaptive behavior as the outcome of interest in middle-aged and older autistic adults. Developmental trajectory research on adaptive behavior skills has been steadily growing to capture how adaptive behavior development changes over time but has predominantly focused on children. 28 Studies extending to early adulthood have included examination of trajectories of characteristics of autism,29–31 emotional and behavioral problems,32,33 and adaptive behavior.22,33 Studies focused on childhood and adolescence have typically identified two homogenous subgroups that reflected differences in patterns of growth. The subgroups include a subgroup where autistic children showed growth in skills through early adulthood and another subgroup where children showed lower adaptive behavior skills with a slower gain in adaptive behavior skills.34–37 Individuals in higher adaptive behavior growth groups had fewer autism characteristics on autism measures and higher scores on language assessments.34–37 Higher adaptive behavior growth over time was also predictive of participation in postsecondary education. 22 These studies support heterogeneity in adaptive growth over time and the importance of adaptive behavior in transition to adulthood but did not extend into middle-aged or older adulthood.
Some cross-sectional studies examining daily living skills and adaptive behavior through middle and older ages have not found age-related differences in daily living skills,3,23 although evidence varies. 18 One cross-sectional study of autistic individuals (age range 16–55 years, 19% with intellectual disability) found a low (mean, standard scores <70) and stable profile of daily living skills across adolescents and adults, 23 while another study of autistic adults (age range 30–73 years, 84% with intellectual disability) also found similar levels of independence across ages. 3 Another study found greater independence in daily living skills in young adults compared with middle-aged adults. However, this may have been because of a higher co-occurrence of intellectual disability in middle-aged adults. 18
Few studies have examined trajectories of adaptive behavior beyond young adulthood into middle adulthood using a longitudinal design.21,38–40 However, those studies suggest a plateau or decline may be present at some point during adulthood. In longitudinal studies examining daily living skills from childhood through early adulthood, there is evidence of a plateau or decline after adolescence.21,38 For example, in a study by Smith and colleagues, 39 daily living skills began to plateau in the late 20s before declining in the early 30s, 39 and a study by Hong and colleagues 40 reported that rather than plateauing, individuals gained skills through early adulthood, but decreased in midlife and beyond. 40 When comparing samples by cognitive level, all groups showed similar trajectories, although the intellectual disability groups had a flatter trajectory with reduced gains across time.38–40 The current study is among the first to examine developmental trajectories in individuals diagnosed with autism spectrum disorder from toddlerhood to adulthood using a longitudinal design and the first to explore how the growth of adaptive behavior skills is associated with outcomes in adulthood.
Support with adaptive behaviors is consistently described as an area of service need in autistic adults from early to later adulthood.41–43 Research with young and middle-aged autistic adults has identified associations between adaptive behavior and autistic traits. Autistic traits, including restricted and repetitive behaviors, 20 social communication differences,20,21 and overall autistic trait ratings, 22 are associated with daily living skill outcome, with higher ratings of restricted/repetitive behaviors and social communication differences related to more daily living skill challenges. While studies have shown associations between adaptive behavior skills, postsecondary education participation, and employment,22,44 autistic adults often still live with their families and have high support needs.41,44
While employment, postsecondary education, and living situation are objective factors of adult outcomes, the subjective well-being of autistic adults is essential when identifying how service providers and caregivers can support autistic adults in self-determined decisions for their adult lives. 45 One area of subjective well-being is quality of life, which refers to an individual’s or a proxy reporter’s perception of their position in life.46,47 Stakeholders have indicated that research priorities should include the identification of support needs and the development of skills across the lifetime. 48 Notably, autistic individuals report lower quality of life than the general population,49,50 and better daily living skills are associated with objective quality of life 18 and maternal proxy reports of subjective quality of life. 51 These studies focus on prediction rather than incorporating within the developmental trajectory, suggesting the importance of examining both objective and subjective aspects of quality of life when examining the development of adaptive behavior through adulthood. Furthermore, stakeholders have noted that the majority of studies on quality of life include autistic adults without intellectual disability, indicating that those with intellectual disability are not well-represented in the current literature 46 ; thus, the current study includes autistic adults with co-occurring intellectual disability. We note that proxy reports of subjective quality of life are in the literature for autistic adults with co-occurring intellectual disability.
In this article, we describe adaptive behavior change in a sample of 266 from ages 1 to 55 diagnosed with autism spectrum disorder and seen for developmental evaluations at multiple time points at the TEACCH Autism Program beginning in 1968. Observing adaptive behavior over time can lead to identifying potential intervention targets at specific developmental periods to support outcomes in autistic adults. This study uses a longitudinal design to capture age-related change of adaptive behavior over time, how intellectual functioning and autism characteristics throughout childhood and adulthood influence adaptive behavior change, and how daily living skills in adulthood, postsecondary education and vocational activities, and quality of life are associated with adaptive behavior.
Methods
Participants
Participants for the current study were 266 individuals diagnosed with autism by clinicians at the University of North Carolina (UNC) TEACCH Autism Program, part of the UNC School of Medicine, between 1969 and 2000. See Table 1 for participant characteristics. At the time of their first evaluation, participants had an average childhood IQ of 61.81 (standard deviation [SD] = 25.74, range = 39–138). While the autistic individuals represented the full range of IQ scores, a majority of the sample had low IQ, with 63% having IQ scores below 70. Estimates of intellectual disability among autistic individuals in the general population before 2000 were estimated between 61% and 75% and between 33% and 40% from 2000 to 2020.48,52–55 The TEACCH Autism Program was founded in 1965 and has been providing clinical services for autistic individuals across the lifespan since then. The participants recruited for this study were 20 years or older at the time of recruitment and received an autism diagnosis by TEACCH during childhood before the year 2000.
Participant Demographics
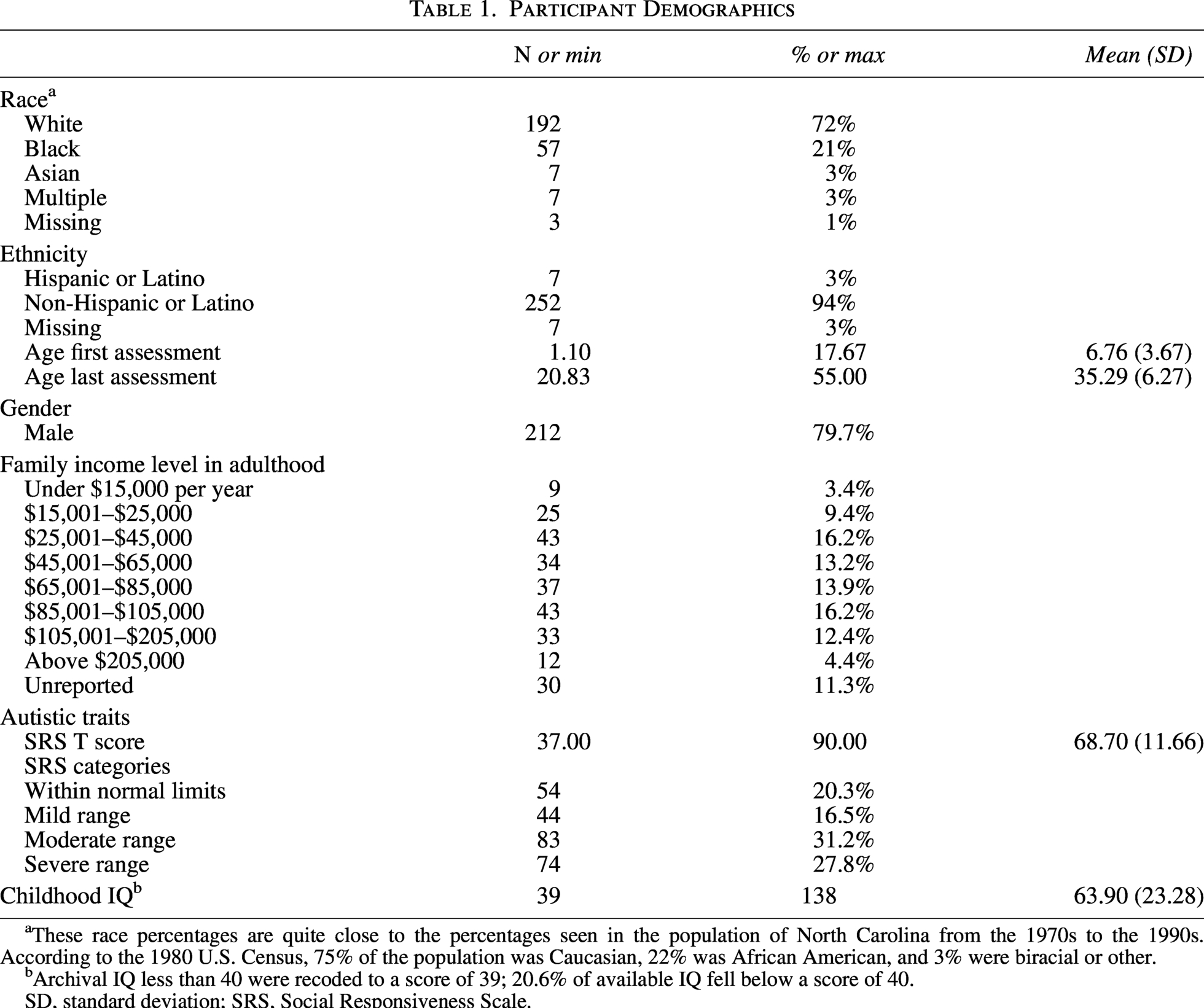
These race percentages are quite close to the percentages seen in the population of North Carolina from the 1970s to the 1990s. According to the 1980 U.S. Census, 75% of the population was Caucasian, 22% was African American, and 3% were biracial or other.
Archival IQ less than 40 were recoded to a score of 39; 20.6% of available IQ fell below a score of 40.
SD, standard deviation; SRS, Social Responsiveness Scale.
Procedure
Data included archival clinical records from the UNC TEACCH Autism Program (n = 266), a survey collected in mid-adulthood (n = 266), and in-person mid-adulthood assessments one to two years following the survey (n = 55). The study team contacted participants in 2014 and 2015 from a clinical database of individuals who were seen for an evaluation during childhood at the UNC TEACCH Autism Program between 1969 and 2000 to complete a survey about outcomes in mid-adulthood. The archival clinical data were only pulled from records for families from the clinical database (n = 7,000) for those who were able to be re-contacted (n = 432). Of those who were re-contacted, there were no differences between those who completed the study (n = 274), those who were enrolled but did not complete their participation (n = 80), and those who we were able to contact but declined to participate (n = 78) in childhood IQ, autism characteristics as measured by the Childhood Autism Rating Scale (CARS), or adaptive behavior measured by total Vineland composite score. Institutional review board’s approved consent and assent procedures were followed, and researchers obtained informed consent from all participants in this study. See Dudley et al. 41 for a complete description of the survey recruitment methods, consort diagram, and a comparison between those who completed the study, those who were enrolled but did not complete their participation, and those we were able to contact but declined to participate, with no significant differences in childhood IQ, autism characteristics, or adaptive behavior between the groups. We combined childhood evaluation data and survey response data. For individuals with multiple childhood evaluations, we included all data. In 2016, the study team contacted a purposive sample of 103 families who still lived in North Carolina to recruit a subset of participants for in-person mid-adulthood assessments. Members of the research team, including psychology graduate students, clinical psychology postdoctoral fellows, clinical psychologists, and research assistants, traveled to each of the seven UNC TEACCH outpatient clinics and assessed individuals at the clinic closest to their residences. In total, 55 adults and their caregivers completed the in-person mid-adulthood assessments. t-Tests and chi square tests were performed to examine if there were significant differences between the total sample from the survey (n = 240) and those who completed in-person mid-adulthood assessments (n = 55). There were no significant differences in autism characteristics, t(257) = 1.01, p = 31, sex, χ2 (1) = 0.57, p = 0.57, ethnicity χ2 (1) = 2.03, p = 0.58, race, χ2 (4) = 1.45, p = 0.84, or income, χ2 (8) = 7.11, p = 0.53. Those who completed mid-adulthood assessments were significantly younger at their first visit, with a difference of 16 months between the groups, t(98.16) = 2.41, p = 0.02. In addition, those who completed a mid-adulthood assessment had a higher childhood IQ score (mean [M] = 73.0, SD = 24.0), compared with those who did not (M = 61.3, SD = 22.5), t(229) = 3.2, p = 0.001. Finally, those who completed mid-adulthood assessments had higher initial childhood adaptive behavior evaluation (M = 61.5, SD = 20.1) compared with those who did not (M = 50.7, SD = 18.7), t(231) = 3.5, p < 0.001. Given the timing of the evaluations in childhood (between 1969 and 2000) and the records review nature of the study, this research relied on current versions of updated measures.
Measures
Adaptive behavior in childhood and mid-adulthood (Vineland scales9–11,56)
The Vineland scales are caregiver interviews designed to assess adaptive behavior skills in children, adolescents, and adults with a developmental disability. Since its original publication as the Vineland Social Maturity Scale (VSMS 56 ), it has seen three revisions: the Vineland Adaptive Behavior Scale (VABS 11 ) the Vineland-II, 10 and the Vineland-3. 9 Archival clinical records of the childhood evaluations included the overall adaptive behavior composite (ABC) score on either the VSMS or the VABS. Assessments in mid-adulthood utilized the Vineland-II Caregiver Interview (2005), also providing a Vineland ABC score. The Vineland ABC standard score captures adaptive behavior skills in daily living, communication, and socialization. To better measure developmental change over time (rather than accounting for chronological age using standard scores) and to account for multiple versions of the Vineland across decades, Vineland age equivalence scores were derived from the ABC score and used for analysis using the formula: Age Equivalence Score = (IQ/100) × Age in Months. The total number of Vineland assessments for each participant ranged from 1 to 9, with an average of 4.5 (SD = 3.6). Adult Vineland scores were available for 23% of the sample, including the 55 autistic adults who all completed the Vineland as part of in-person evaluations.
Cognitive abilities in childhood (IQ)
Children evaluated at TEACCH clinics from 1965 to 2000 typically completed an IQ or developmental test during their childhood assessment. Participants in the study received a Stanford–Binet Intelligence Scale, 57 Bayley Scales of Infant Development, 58 Leiter International Performance Scale, 59 or Merrill–Palmer Scale of Mental Tests. 60 Each of these tests was appropriate based on the child’s developmental level at the time as judged by the clinician. These tests provided a standardized IQ score with a mean of 100 and a standard deviation of 15 or a mental age score in months. We included IQ scores from each evaluation visit. When standardized IQ scores were unavailable, we calculated an estimated IQ score as the ratio of mental age divided by chronological age times 100.
Autism characteristics in childhood and mid-adulthood (CARS 61 ; CARS, Second Edition 62 ; Social Responsiveness Scale, Second Edition, Adult Scale 63 )
The CARS is a clinical measure of autism characteristics completed by a clinician after directly observing an individual. The CARS 61 and CARS-Second Edition (CARS2) 62 comprise 15 items rated with a score from 1 to 4. The score assigned represents how closely the individual’s response matches the responses of typically developing children—the more closely aligned the reaction to that of typical development, the lower the score. Higher scores on the CARS and CARS2 indicate a higher likelihood of an individual being on the autism spectrum. Items on the CARS and CARS2 measure areas impacted by autism, such as verbal communication, nonverbal communication, imitation, difficulty with change in the environment, and relationships. The authors of the CARS developed the measure at TEACCH and utilized the CARS in clinical evaluations before its publication in 1988. Retrospective records review of childhood evaluations between 1969 and 2000 used the CARS and included total scores. Evaluations in mid-adulthood in 2016 utilized the CARS2, including the standard (CARS2-ST) and high functioning (CARS2-HF) forms. The CARS2-ST is for individuals under age 6 or with cognitive abilities in the intellectual disability range (i.e., IQ < 70). The CARS2 maintained the original format of the CARS with the CARS2-Standard (CARS2-ST). The CARS2-HF is utilized for individuals over age 6 with low-average to above-average cognitive abilities. The CARS2-HF allows raters to incorporate clinical observations of an individual and caregiver or secondary reporter information into scores. The internal consistency of the CARS and CARS2 measures range from 0.93 to 0.96,61,62 with high levels of sensitivity and specificity for the CARS-2 when using DSM-IV-TR or DSM-5 criteria for a diagnosis of autism. 64 CARS scores were used from clinic records when available.
The Social Responsiveness Scale, Second Edition (SRS-2) is a 65-item questionnaire that assesses individual autism spectrum characteristics and provides five subscales and a composite score of total autism characteristics. This scale has excellent internal consistency (α = 0.94–0.96) and test-retest reliability (r = 0.88–0.95). 65 Caregivers of autistic adults completed the Relative/Other Report version of the SRS-2, Adult Form, through the outcomes in the mid-adulthood survey. In the current sample, the Cronbach’s α was 0.95.
Daily living skills in mid-adulthood (Waisman Activities of Daily Living Scale 19 )
The Waisman Activities of Daily Living Scale (W-ADL) measures current levels of independence in performing activities of daily living in adolescents and adults with developmental disabilities. It lists 17 activities rated from 0 (does not do at all) to 2 (does independently). Examples of activities of daily living assessed include mixing and cooking simple foods, washing/bathing, doing errands, and banking and managing daily finances. All items are summed to yield a total score, with higher scores indicating higher participation and independence in daily living skills. Validation of the W-ADL involved individuals with Down syndrome, Fragile X syndrome, autism, and intellectual disability with high internal consistency (α = 0.88–0.92) and reliability between respondents (r = 0.88 19 ). The Cronbach’s α in the current sample was 0.91. While the Vineland is more comprehensive than the W-ADL because it captures daily living skills, communication, and socialization, previous research with adolescents and adults with developmental disabilities has established criterion validity with the Vineland Screener Adaptive Behavior Composite (r = 0.78) and the Daily Living Skills subdomain score (r = 0.82). 19 Caregivers of autistic adults completed the W-ADL through the outcomes in the mid-adulthood survey.
Quality of life in mid-adulthood (Quality of Life Questionnaire 66 )
The Quality of Life Questionnaire (QOL-Q) assesses the quality of life of individuals with intellectual and developmental disabilities. The QOL-Q has four scales with ten questions each: Life Satisfaction, Competence/Productivity, Empowerment/Independence, and Social Belonging. Questions are rated from 1 to 3 points and summed to derive a scale score. Omissions were coded following norms from the original authors, with the respondents’ average answers in the corresponding subscale and excluding scales with four or more omissions. If an individual is unemployed, the maximum Competence/Productivity subscale score is automatically 14. Due to the current sample’s 54.5% unemployment rate, we excluded the Competence/Productivity subscale from the analysis. The internal consistency of the subscales ranges from 0.66 to 0.83, with a total alpha reliability coefficient of 0.83. 66 The Cronbach’s α was 0.91 in the current sample. Caregivers of autistic adults completed the QOL-Q through the outcomes of the mid-adulthood survey.
Vocational and education activities in mid-adulthood (Vocational Index 67 )
The Vocational Index (VocIndex) is an index of vocational and educational activities meant to capture the full range of outcomes autistic adults may experience after they exit secondary education. It is a 9-point scale ranging from no vocational/educational activities (1) to competitive employment and/or postsecondary educational programs at least 10 hours a week (9). We derived the data for coding the VocIndex in this sample from the outcomes of mid-adulthood survey responses (see Dudley et al. 41 ).
Analysis plan
Utilizing an age-heterogenous sample, we investigated the developmental trajectories of adaptive behavior from early childhood to mid-adulthood. This allows for the inclusion of individuals who visited TEACCH at multiple time points and are of different ages.40,68–70 The present study spanned 41 years between 1969 and 2016, including individuals as young as 13 months and as old as 17 years at the first evaluation. We used multilevel modeling to estimate growth trajectories of adaptive behavior to examine age-related changes from early childhood to mid-adulthood. Multilevel modeling allows for the ages, number of measurements, and the intervals between measurements to vary between participants.
71
In addition, multilevel models allow for the inclusion of all participants with at least one measurement occasion if the missing data is assumed to be missing at random, assuming that missing values are related to observed variables in the dataset.
72
We performed all analyses in the nlme R statistical package.
73
The first step was to determine the shape of the growth model, linear or nonlinear. A linear growth model is as follows:

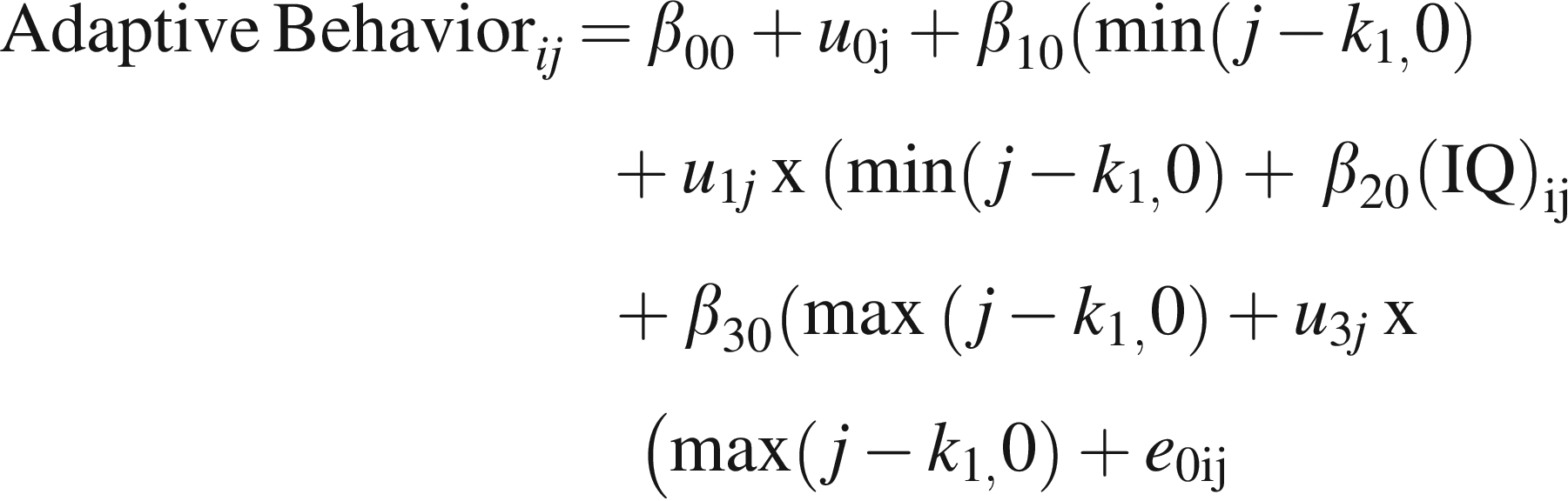
Fit statistics determined the best fitting model, −2 × Loglikelihood, Akaike Information Criteria, and Bayesian Information Criteria. We used the L ratio test to determine whether fit was statistically different among models. Next, we added a time-varying covariate of CARS scores over time to the best-fitting model. Then, we examined time-invariant covariates of daily living skills, caregiver perceptions of quality of life, and vocational index measures in adulthood. All covariates were centered to represent the mean of the sample. The best-fitting model was selected based on the L ratio test for the final model and inclusion of covariates. The statistical analyses addressed missing data by using Maximum Likelihood Estimation (ML). ML is advantageous over deletion methods, which produce biased estimates. 74 ML uses all available data to identify parameters that most likely represent the sample data.
Results
The quadratic and spline models were the best-fitting models for adaptive behavior equivalency over time, controlling for IQ (see Table 2). Additional polynomial models (i.e., cubic and higher) did not converge. The quadratic model fit significantly better than the linear model, L. Ratio = 108.41, p < 0.001. We tested spline models after visually inspecting the scatter plots, including quadratic and polynomial trend lines (see Fig. 1). Based on the trend lines, we tested knot points in adolescence (15), young adulthood (18–21), and mid-adulthood (33, 38). Thirty-three and 38 were potential points where the curves appeared to trend downward. Models did not converge at age 15, 18, or 38. Models converged at age 20 and age 33. The spline models did not statistically differ in fit statistics from the quadratic model. In the quadratic model, there was an average linear rate of change over time of 0.25 years (about 3 months) and a significant negative quadratic effect, suggesting a deceleration in adaptive behavior growth over time. In the spline model with the knot at 20 years, from 1 to 20 years, the average rate of change in adaptive behavior equivalency scores was 0.27 years (about 4 months) per 1 year in chronological age, and from 20 to 55 years, it was —0.14 years (about 2 months). In the spline model with the knot at 33 years, from 1 to 33 years, the average rate of change in adaptive behavior age equivalency scores was 0.43 years per year, and from 33 to 55 years, it was 0.05 years.

Developmental trajectories of adaptive behavior over time with overlaying trend lines. Trend Lines of Growth Models: Green = Linear; Red = Quadratic; Purple = Cubic; Blue = Quartic; Orange = Quantic.
Parameter Estimates for Adaptive Behavior Trajectories of Autistic Individuals from Early Childhood to Middle Adulthood
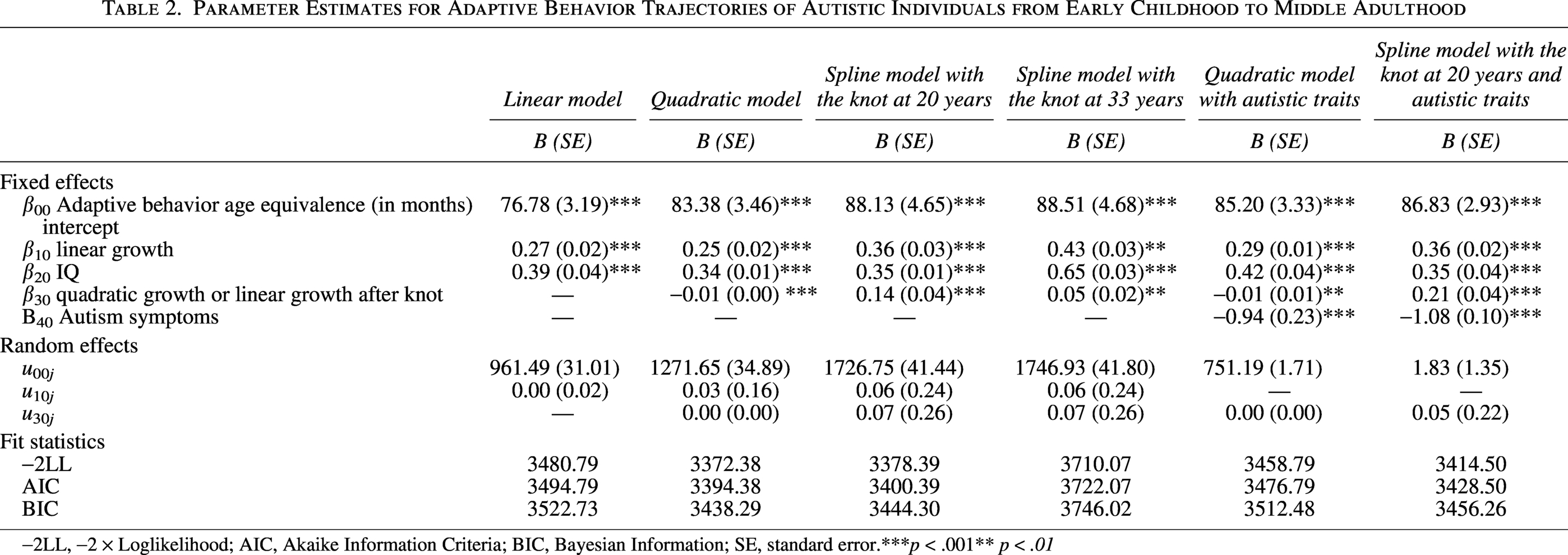
−2LL, −2 × Loglikelihood; AIC, Akaike Information Criteria; BIC, Bayesian Information; SE, standard error.***p < .001** p < .01
IQ was positively associated with adaptive behavior over time, suggesting that individuals with higher IQs in childhood had higher adaptive behavior age equivalency scores (see Table 2 for parameter estimates). The average effect of IQ was statistically significant, suggesting that for every 1-point increase in IQ, an individual increased their growth rate of adaptive behavior by 0.25 in the quadratic models and 0.36 in the spline models. Since most studies have examined IQ regarding the diagnosis of Intellectual Disability Status (IQ <70), we conducted analyses with models to determine whether intellectual disability status was significantly associated with adaptive behavior growth. Intellectual disability status was not a significant predictor of the growth of the models, suggesting that IQ across childhood was a more salient predictor than intellectual disability in the current study.
CARS scores were added to each model to examine how autism characteristics were associated with adaptive behavior over time. The average effect of CARS scores was statistically significant, suggesting that for every 1-point increase in CARS scores, an individual decreased their growth rate of adaptive behavior by 0.94 in the quadratic model and 1.08 in the spline model.
While the fit statistics did not significantly differ between the two spline models and the quadratic model, the time-invariant covariates of daily living skills, caregiver perceptions of quality of life, and vocational index from adulthood across ages 21–55, so the spline model with the knot point at age 20 was selected to examine how these covariates were associated with adaptive behavior scores at age 18, the growth of adaptive behavior during childhood (ages 1–20), or the pre-knot slope, and the growth of adaptive behavior during adulthood, or the post-knot slope, controlling for IQ and CARS scores (see Fig. 2 for the final selected spline model).
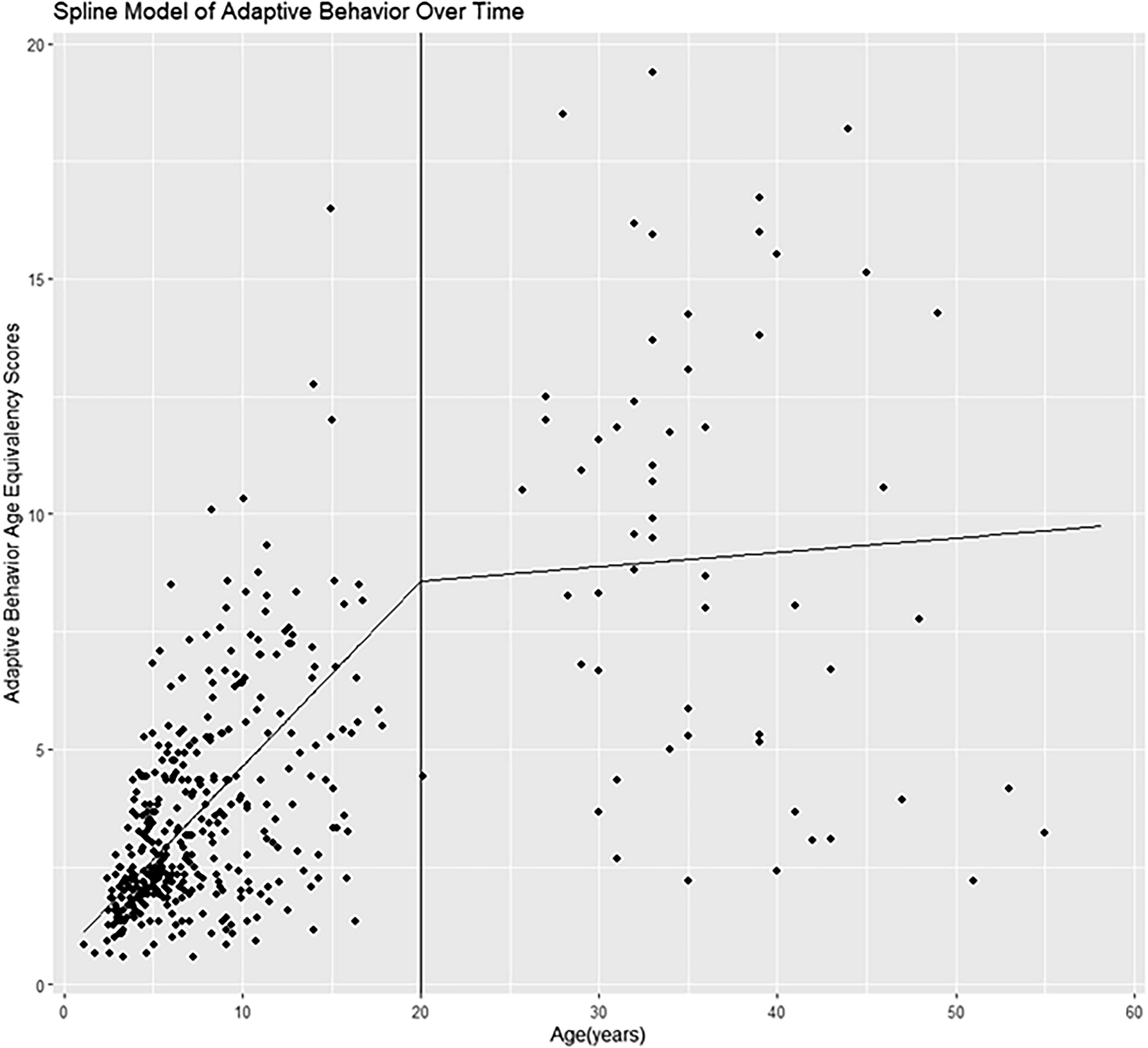
Spline model of adaptive behavior over time.
Daily living skills, quality of life, and vocational index scores were associated with the adaptive behavior scores at age 18 (intercept) and the rate of change in adaptive behavior age equivalency scores from childhood to young adulthood (1–20) or the pre-knot slope. Higher adaptive behavior scores at age 18 were associated with higher daily living skills in adulthood, Est = 0.96, standard error (SE) = 0.19, t(436) = 4.95, p < 0.001. Higher adaptive behavior scores at age 18 were associated with higher vocational index scores in adulthood, Est = 3.61, SE = 0.91, t(436) = 3.99, p < 0.001. Higher adaptive behavior scores at age 18 were associated with higher quality of life scores in adulthood, Est = 0.54, SE = 0.15, t(436) = 3.61, p < 0.001. The pre-knot slope was positively associated with daily living skills, Est = 0.01, SE = 0.01, t(436) = 4.04, p < 0.001, vocational index scores, Est = 0.02, SE = 0.01, t(436) = 3.27, p = 0.001, and quality of life, Est = 01, SE = 0.01, t(436) = 3.21, p = 0.01.
Daily living skills and caregiver perceptions of quality of life were statistically significantly associated with the rate of change in adaptive behavior, age equivalency scores during adulthood (21–55), or the post-knot slope. There was no statistically significant association of the vocational index with the post-knot slope, Est = 01, SE = 0.01, t(436) = 1.25, p = 0.22. Daily living skills were positively associated with the post-knot slope, Est. = 0.01, SE = 0.01, t(436) = 3.94, p < 0.001, suggesting that adaptive behavior growth in adulthood was associated with daily living skills. Caregiver perceptions of quality of life were positively associated with the post-knot slope, Est = 0.01, SE = 0.00, t(436) = 4.65, p < 0.001, suggesting that increased adaptive behavior growth in adulthood was associated with improved caregiver perceptions of quality of life.
Discussion
This study described age-related trajectories of adaptive behavior from early childhood to adulthood. It drew from data collected over 48 years from individuals aged 1–55 with a full range of intellectual abilities, including 63% of the sample having a co-occurring intellectual disability. The analysis provided insight into patterns of adaptive behavior change through early adulthood and midlife in autistic adults and how these patterns of change are associated with daily living skills, caregiver perceptions of quality of life, and vocational and educational experiences.
We investigated the extent to which age-related change of adaptive behavior was linear or curvilinear and how intellectual functioning and autism characteristics over time and adult outcomes are associated with the growth of adaptive behavior skills through adulthood. We extended the findings of Meyer and colleagues 38 to include individuals between 20 and 55. Findings suggest that adaptive behavior growth is curvilinear over time, with different growth rates between childhood, adolescence, and adulthood. Rather than a plateauing of skills during early adulthood, 38 skills are grown across early adulthood from 20 to 35 to 40. There appears to be a potential for decline following mid-adulthood, which is like findings reported by Hong and colleagues, who examined trajectories of activities of daily living and found a pattern of discontinuity, with improvements of skills during adolescence and adulthood, a plateau, and eventual worsening. 40 Clarke and colleagues 22 found that participants after high school had declined their daily living skills at age 26, and similarly, they did not find that daily living skills were associated with employment. The current study did not examine classes of individuals within the sample and examined only one inflection (i.e., knot) point. Future studies should continue to include older adults 30 and older to explore the potential decline in adaptive skills in adulthood and examine whether there are potential subgroups that have differential patterns of growth over time.
While IQ was significantly associated with adaptive behavior, adaptive behavior age equivalency scores were much lower than would be expected for chronological age. For example, at the first childhood evaluation, children were, on average, 7.34 years old compared with their adaptive behavior mental age equivalency scores of 3.0 years. Across the entire sample, the average age is 17 years, and the average Vineland age equivalency score is 6.0 years. These findings support previous research findings regarding discrepancies between IQ and adaptive behavior.13–17 In addition, average adaptive behavior at age 18 and adaptive behavior growth from early childhood to young adulthood correlated with daily living skills, vocational and educational experiences, and quality of life in mid-adulthood. These findings highlight the importance of adaptive behavior during childhood impacting these outcomes during high school. To support the continued growth of adaptive behavior skills over time, there is a critical need for the evaluation of evidence-based strategies that support autistic adults. Currently, there is limited literature on what supports might be most helpful for adaptive behavior. One program, Surviving and Thriving in the Real World, has demonstrated efficacy in supporting gains in daily living skills for adolescents without an intellectual disability, 75 and another study found preliminary evidence for an executive function intervention in promoting adaptive behavior for adults without an intellectual disability. 76 More research is needed to include individuals with intellectual disability to engage in community participatory development of adaptive behavior supports for autistic adults.
Findings did suggest that increased adaptive behavior growth in adulthood was associated with improved caregiver-reported quality of life. This finding indicates that when individuals gain adaptive behavior skills during adulthood, they have increased overall quality of life as measured by the QOL-Q domains of Life Satisfaction, Empowerment/Independence, and Social Belonging. The Empowerment/Independence domain includes how an individual can make decisions in their adult life, such as being able to choose how they spend their money and who they live with. Social Belonging includes times spent with friends and having supportive neighbors. Making decisions and advocacy are components of self-determination, identified as essential strategies to help adults enhance their advocacy skills and social participation. 77 Self-determination is also associated with adaptive behavior.78,79 Future studies should continue to examine adaptive behavior and quality of life and consider the role of self-determination.
This article has several limitations. Measurements were highly variable among the sample due to being a records review, and a small subset completed in-person follow-up visits. We handled missing data using maximum likelihood methods to reduce bias. However, a larger sample of adult ages would allow for greater precision in estimating the potential decline of adaptive behavior into adulthood. The sample includes individuals diagnosed in the late 1960s and 1970s, which does not reflect autism referrals in current clinics. This study did not investigate differences in adaptive behavior trajectories by sex, gender, race/ethnicity, or other sociodemographics. Future studies should examine the cultural and social contexts of adaptive behavior trajectories to identify potential environmental factors that may support autistic adults. The use of the Vineland Adaptive Behavior Scales may not accurately capture the experience of adaptive behavior for autistic adults and their support needs when completed by a proxy reporter. Additional measures and self-reporting of adaptive behavior will ensure that future research adopts a neuroaffirmative approach. Proxy-reported QOL-Q was used rather than self-report in the current analysis. Previous studies have found that proxy reports are associated with skills, such as adaptive behavior, whereas self-reports have focused on environmental factors, such as stress and bullying. 51 While the quality of life scores tend to be correlated,51,80 the unique perspectives of autistic adults, including those with intellectual disability, are critical to include to support the understanding of their perceptions and support needs. 45
Conclusion
Adaptive behavior is an essential area of support for autistic adults regardless of intellectual functioning and autism characteristics. Our findings suggest that adaptive behavior plateaus and potentially declines during adulthood. Given the importance of adaptive behavior on quality of life, this study reflects the importance of adaptive behavior as a potential support area for autistic adults. It may be that existing interventions and programs do not focus on adaptive behavior skills. Importantly, research has highlighted mental health interventions,81,82 but an emphasis on adaptive behavior is warranted. Future research is needed to support the identification of adaptive behavior support and intervention during adulthood.
Footnotes
Acknowledgments
The authors are grateful to the families who participated in this study. The authors also acknowledge the work of the clinicians at TEACCH for recording these data and the larger study team that reviewed records for the archival data used in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding was provided for this study by the Foundation of Hope, Autism Speaks, and the Department of Defense.
Authorship Confirmation Statement
The article has been submitted soley to Autism in Adulthood. B.T.: Conceptualization, methodology, formal analysis (lead), writing—original draft, and visualization. C.B.K.: Writing—original draft. A.T.M.: Investigation and writing—reviewing and editing. E.L.: Data curation, investigation, writing—original draft, and project administration. L.G.K.: Conceptualization, funding acquisition, investigation, writing—reviewing and editing, and supervision.