
Abstract
Background:
Literature indicates that mental health of autistic individuals is substantially poorer than that of the general population. Mental illnesses, such as depression and anxiety, which contribute to high suicide rates, feature prominently in research. Few studies, however, have considered the lived experience of mental health across the lifespan, which includes the experience of positive mental health. This research investigated the lived experience of mental health of autistic adults.
Method:
We used reflexive thematic analysis, underpinned by a coproduction framework, to explore mental health experiences. Through coproduction with a steering group of autistic adults to inform the questions, we conducted semi-structured interviews with 20 Australian autistic adults, diagnosed in adolescence or adulthood.
Results:
The thematic analysis identified four main themes, including discovering autistic identity, body and mind, connections to family and community, and choice and control. Participants reported highly heterogenous life experiences, with intense experiences of mental health, both positive and negative. All participants experienced mental health challenges, and most had experienced a diagnosed mental illness. Protective factors that mitigated against mental illness included supportive environments, relationships, and positive societal attitudes.
Conclusion:
While some of the themes are universal, some of the subthemes, such as the significance of sensory input and adaptive morphing to hide autistic traits, do not feature in non-autistic mental health literature. These factors, which frequently interrelate, may be overlooked by mental health care providers. The findings of this research emphasize that in order to support positive mental health outcomes, there is a strong need for therapies and disability supports to be targeted and tailor-made to the individual.
Community Brief
Why is this an important issue?
Many autistic people experience mental illness at rates much higher than the general population. This area had been overlooked for many years. While we know that rates of mental illness are very high, not much is known about the personal autistic experiences of mental health or what can support positive mental health.
What was the purpose of this study?
Researchers wanted to hear and understand the stories of autistic adults to learn about their experiences of mental health. We especially wanted to know what helped improve participants
What did the researchers do?
This coproduction project included two autistic researchers, including the first author, and a steering group of five autistic community members. Twenty autistic adults volunteered to take part in interviews, sharing their experiences of mental health, both positive and negative, from across their life. The researchers analyzed and organized the stories into themes.
What were the results of the study?
All participants had very different life and mental health experiences. Even though there were differences, similar factors or themes could be seen. The project found 4 main themes and 16 subthemes. These themes could have a positive or a negative impact on an individual depending on the personal circumstances of that individual at any given point in time. The first theme, discovering autistic identity, included the impact of autism diagnosis on identity, adaptive morphing to hide autistic traits, interests providing purpose and connection, and a passion for social justice. The second theme, body and mind, included the significance of sensory input, the importance of physical health, sleep, diet and exercise, co-occurring conditions exacerbating mental health challenges, executive functioning challenges, coping mechanisms for daily life, and the long-term impact of trauma and grief. The third theme, connections to family and community, included supportive relationships as a protective factor, parenting as a double-edged sword, and the challenges of interacting with professionals. The final theme, choice and control, included the personalization of therapies, affordability and life choices, and disability support mechanisms.
What do these findings add to what was already known?
Some of the subthemes, such as the significance of sensory input and adaptive morphing to hide autistic traits, do not feature in non-autistic mental health literature. These factors may be overlooked by mental health care providers.
What are potential weaknesses in the study?
Participants were all Australian, with a majority being Caucasian, and even though verbal communication was not a requirement, all participants communicated by speaking for the interviews. All participants who volunteered were diagnosed as teenagers or as adults. More research is needed for groups not represented in this study.
How will these findings help autistic adults now or in the future?
It is hoped the findings of this research will contribute to encouraging therapists and disability service providers to ensure mental health therapies and supports are tailor-made for the individual, taking unique autistic traits into account.
Background
The Autism Spectrum is a lifelong, heterogenous, neurodevelopmental disposition that can cause significant social, behavioral, and communication challenges. 1 Globally, it is estimated that the current prevalence of autism is 1 in 100 people. 2 In 2018, there were over 205,000 autistic people living in Australia, the majority of whom were under the age of 25. 3 Autistic individuals account for 31% of all individuals receiving disability support through the National Disability Insurance Scheme (NDIS). 4
In recent years, mental health has come to the forefront of autism research as a result of examining community priorities 5 ; however there is still much to be explored. According to the World Health Organization, mental health is not simply an absence of mental illness but rather a “state of mental well-being,” which includes a person’s ability to cope with stress, to learn, work, and contribute to their community. 6 There is growing evidence detailing the poor mental health outcomes of autistic individuals.7,8
A recent review of the autistic mental health literature by Lai highlighted not only the prevalence of mental health challenges but also the complexities of co-occurring conditions experienced by autistic people. 8 While many studies vary on the prevalence of mental health conditions, a systematic review and meta-analysis by Hollocks found that the global lifetime prevalence for an anxiety disorder was 42% and 37% for a depressive disorder. 9 In comparison, in Australia the lifetime prevalence for an anxiety disorder is 28.8% and 16% for affective disorders such as depressive episodes. 10 Another systematic review and meta-analysis, by Blanchard, determined that autistic children and adults are three times more likely to engage in self-harm than the general population, 11 and a systematic review by Sanomauro found that autistic people are three times more likely to die by suicide than the general population. 12 To better understand the high prevalence of poor mental health outcomes for autistic people, studies have investigated the association between autistic traits and suicidality,13,14 while others have looked at risk markers 15 and identified risk factors, such as rumination, poor self-esteem, 16 thwarted belonging, perceived burdensomeness, trauma, 17 and camouflaging of autistic traits. 18
Camouflaging, otherwise known as adaptive morphing, 19 describes how autistic people, either consciously or subconsciously, alter their behaviors for safety and to be accepted by their peers. Adaptive morphing is a mechanism that arises from a challenging social environment and communication differences that are often seen by others as deficits and has been found to be a significant predictor of mental illness and suicidality. 20 While many autistic individuals experience social anxiety 21 and bullying,22,23 and struggle with developing and maintaining friendships, 24 the impact of these experiences is reduced when autism acceptance is promoted. 25
A factor that does not often feature in mental health research for the general population is that of sensory processing. Studies in both autistic and non-autistic groups have demonstrated a connection between interoception, (i.e., the body’s ability to interpret inner sensory input) and emotions and anxiety.26,27 Studies have also connected the intolerance of uncertainty, sensory sensitivity, and repetitive behaviors with anxiety in autistic individuals.28,29 Another study furthers this outcome to demonstrate that for autistic children, being sensory seeking is associated with external mental health indicators, while hyperreactivity to sensory input is associated with internal mental health indicators, such as anxiety and depression. 30 Furthermore, a recent study found a positive association between sensory processing differences and an increase in depression and anxiety, which becomes more prominent with age. 31
In considering the brain’s processing mechanisms, another factor to consider is that of executive functioning. Executive functioning may impact autistic ability to complete everyday tasks and has a significant effect on mental health. 32 Executive dysfunction has a potential flow on effect with employment 33 and quality of life, 34 which has been shown to be significantly poorer for autistic individuals.35–37
The social communication and cognitive processing challenges, which so many autistic individuals face compared with the non-autistic population, reveal the uniqueness of the autistic experience. For example, anxiety presents atypically for many autistic individuals, with 15% of individuals presenting with exclusively atypical symptoms, such as fear of change or social fearfulness 38 and unique variances from social anxiety. 39 Autistic individuals frequently experience a unique form of burnout, called autistic burnout, which has distinct differences from occupational burnout. 40
While the majority of research focuses on the poor mental health outcomes for autistic individuals, the concept of mental health also encompasses the positive experiences. 41 The role of self-compassion has been associated with improved mental health outcomes. 42 A similar finding, of feeling good about oneself, was reported to improve quality of life by a recent qualitative study, which examined the experience of quality of life for autistic individuals, along with that of being accepted for themselves. 43 Another recent qualitative study found that connection with family, peers, and pets, along with engaging in meaningful activities, contributed to good quality of life. 44
While various aspects and factors of autistic mental health have previously been studied, the unique experiences of autistic individuals’ overall mental health need to be explored and understood given that each of the aspects relating to mental health discussed above does not exist in isolation from one another. The aim of this study was to explore the lived experiences of autistic mental health. From this it is hoped that the results of this study may be used to identify and provide appropriate interventions, therapies, and supports aimed at improving the mental health of the autistic community.
Methods
This study utilized reflexive thematic analysis, 45 underpinned with a coproduction framework. 46 Reflexive thematic analysis is used to create themes that represent patterns of shared meaning. 47 This approach is undertaken from a critical realism positionality and enables the acknowledgment of the subjective influence of the researchers. 45
Coproduction is the process of conducting research in partnership with those who use it 48 and has particular utility in research involving minority or disability groups, giving weight to the opinions and wishes of the community being researched, ensuring their voices are heard and represented.49–51 This research was fundamentally coproduced with two of the authors, including the first author, identifying as autistic, and the overall research project being directed by a steering group of five autistic individuals. 52
Participants
Participants in the present study were aged 18 years or above, requiring a diagnosis of being on the Autism Spectrum according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) or earlier equivalent. Participants were also required to complete the Autism Quotient (AQ-50) questionnaire and obtain a score of 25 or higher.53,54 With the goal of limiting adverse reactions to this study, autistic adults who were currently experiencing, or had experienced in the last 30 days, suicidal ideation were excluded from the study. This was determined using the Suicidal Ideation Attributes Scale. 55 Participants were required to be residents of Australia at the time of the study, able to communicate verbally in English, or via an alternative form of assisted communication, and provide informed consent. Recruitment took place through local autism support organizations, professional networks, social media, and word of mouth.
Data collection
Interviews were conducted both in person, using an audio recorder, and via a recordable video platform depending on the preference of the participant and Curtin University Covid-19 protocols. 56 The interview explored the person’s lived experience with mental health across their lifespan. Topics ranged from childhood experiences through to current experiences, including both positive and negative contributing factors, and the impact and mental health outcomes resulting from those experiences, including but not limited to anxiety, depression, suicidality, burnout, and thriving. Interviews ranged from one to two and a half hours, depending on the participant’s contribution. The interview guide was developed through community consultation in the form of a steering group. The principal researcher first prepared a draft interview guide informed by literature, which was then presented to the steering group for discussion. Based on the outcome of this discussion, the interview guide was then expanded to include more possible items. Also discussed was the way the interviews would be undertaken in terms of question styles and clarity.
Analysis
Reflexive thematic analysis was used to analyze the data, following the six-phase process set out by Braun and Clarke. 45 The first phase is data familiarization. All interviews were conducted and transcribed verbatim and read multiple times by K.B. (an autistic researcher), with the de-identified transcription being imported into the NVivo software for analysis. 57 The second phase of reflexive thematic analysis is systematic data coding. K.B. coded and grouped the data into preliminary categories as each interview was added. With each additional interview, the data were reflected upon, the categories were refined, and the data underwent reflective revision. Throughout the process, K.B. used a reflexive journal with the goal of examining the influence of their personal lived experience on the research and establishing trustworthiness of the data. 58 During the third phase, generating initial themes, K.B. grouped codes that shared similar characteristics, creating the initial themes. The fourth phase was to develop and review the themes, which was conducted by K.B. with the support of the supervision team, B.M., W.L., S.M., and S.G. W.L. provided both professional and personal insight as an autistic researcher, and the non-autistic authors provided their professional insight. The fifth phase, in which the themes were refined, defined, and named, was again conducted by K.B., B.M., W.L., S.M., and S.G. In line with coproduction, the members of the autistic community actively contributed to the final interpretations and decisions regarding the results 59 prior to the final phase of writing the report. The findings were presented to the steering group for consultation, and member checking, to ensure confirmability, was conducted by providing the results’ summary to all participants for feedback. Seven participants responded confirming their agreement with the results. An audit trail has been kept ensuring dependability.
Results
In total, 20 adult participants on the Autism Spectrum were recruited to the study. The age of participants’ autism diagnosis ranged from 15 to 52 years (mean 38.45, standard deviation [SD] 10.18) with all but two participants being diagnosed within 6 years of the interview, while 14 had been diagnosed within the previous 2 years (mean age at diagnosis 35, SD 11.74) (see Fig. 1). Participants reported a wide variety of life experiences, with half of the participants being parents and half currently in a romantic relationship. Participants also reported a variety of employment and education statuses, including full-time, part-time, casual, contractor, and disability pension (see Table 1).
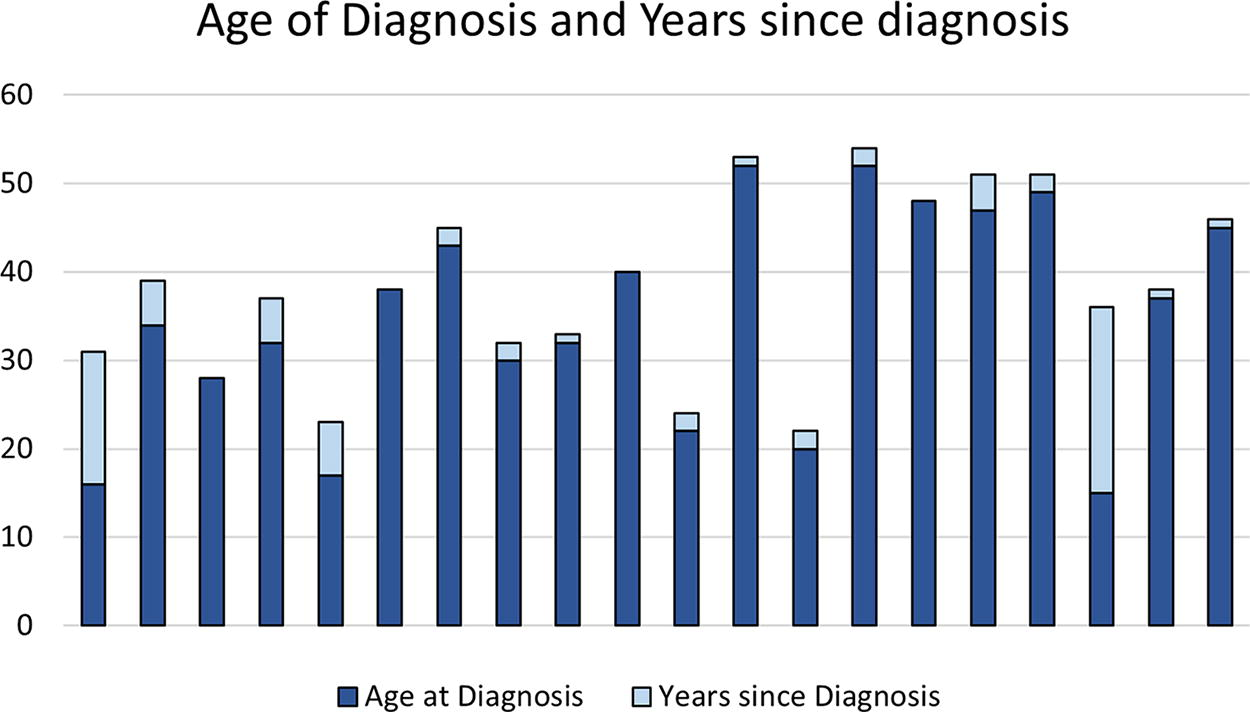
Age of diagnosis and years since diagnosis.
Demographic Information for Participants
ADHD, attention-deficit hyperactivity disorder; cPTSD, complex post-traumatic stress disorder.
Dominant themes identified through the data analysis process related to the lived experience of autistic mental health included discovering autistic identity, body and mind, connections to family and community, and choice and control (see Fig. 2 and Table 2).
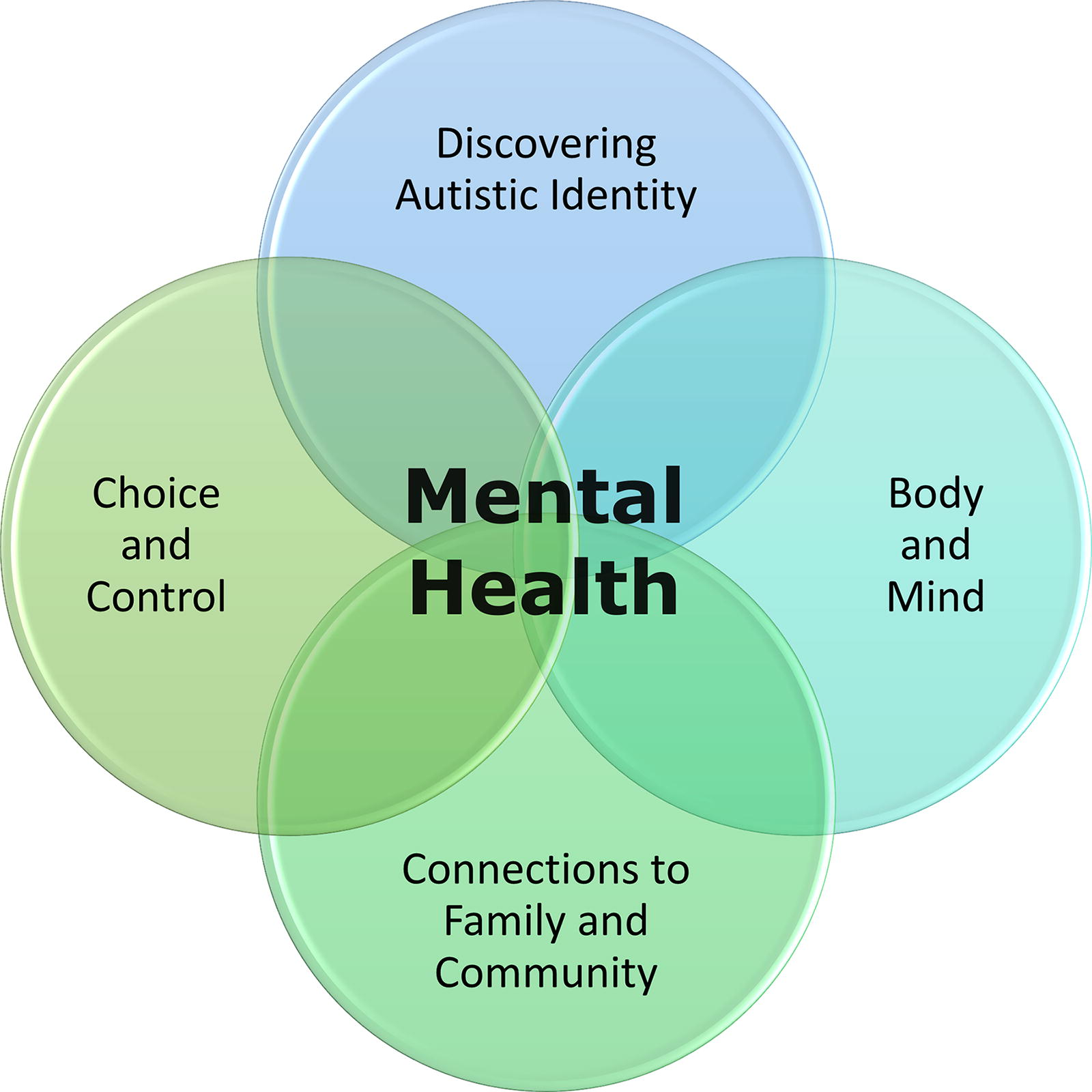
Autistic experiences of mental health.
Themes and Subthemes
Theme 1: Discovering autistic identity
Subtheme 1: Impact of an autism diagnosis on identity
Participants expressed how having an autism diagnosis was ultimately a positive factor contributing to their mental health. This positive impact was felt more strongly the later in life the diagnosis was received. For many participants it provided a sense of clarity, answering their question as to why they had struggled throughout their lives:
Having that diagnosis was actually … it’s like that Tetris game where everything sort of just falls into place … everything got answered in the one hit.—Nicole* (all participant names used are pseudonyms)
Participants described how they often struggled with their mental health because of what they felt they “ought” to be capable of achieving, compared with their actual performance. Many participants reported feeling “broken,” “lazy,” and “useless” prior to their autism diagnosis because they did not understand why they experienced challenges completing tasks in their everyday lives. In contrast, participants who reported being diagnosed autistic in their adolescence expressed a negative impact of having a diagnosis during those adolescent years.
Autism was described to me … everything that I was struggling with, I was incapable of doing … difficulty making friends … Year 12 was just a horrible year for me mental health wise.—Emma
Participants also described the benefits and importance of belonging to the autistic community to their mental health:
It’s given me the blessing of belonging to the Autistic community where there are just some such amazing people.—Gabby
Subtheme 2: Adaptive morphing to hide autistic traits
Adaptive morphing, or attempting to hide their autistic traits, was a frequent coping strategy utilized by participants and contributed to their experiences of isolation, bullying, and being ostracized, even prior to their diagnosis. Many participants expressed that, over time, hiding their autistic traits, whether conscious or subconscious, was detrimental to their mental health. Adaptive morphing often led to burnout, and shutdowns, and the required recovery time varied.
It’s not the work, it’s the social and it’s … the office environment and having to speak to people and … I would put on a mask, or I’d leave the house, put on a mask, I’d get home at the end of the day … I couldn’t even cook food, my brain would just be scattered.—Nicole
Embracing their autistic identity allowed some participants to reduce their adaptive morphing around family, friends, and professionals. This has enabled them to accept their different sensory profiles and communication styles that may require adjustments, and in doing so, they now experience improved mental health outcomes.
Subtheme 3: Interests provide purpose and connection
Participants reported that engaging in their interests and passions brought purpose and joy, enhancing their experience of mental health. Interests were frequently strongly connected with the participant’s identity, their sense of self, and their choice of vocation. Often, those interests provide a mechanism through which the participants are able to connect with others and develop friendships.
So, when I have access to them, it doesn’t matter what else is going on in my life . . . . Everything else can be turning to crap, but I’ve got that constant thing to hold on to … My special interests are the bedrock of my life.—Betty
Conversely, when the participants were unable to engage in their interests, their mental health was negatively impacted.
It’s that long since I’ve done anything hobby wise because it feels, how can you do that when you can’t look after your household? … Defeating, because I’m never gonna get to the point where I’m free to do those things.—Tina
Subtheme 4: Passion for social justice
Many participants expressed a strong sense of social justice, which impacted their mental health. Often this was derived from the personal experience of having suffered forms of injustice or bullying for being themselves, whether their autism diagnosis was known or not. Witnessing injustices around them without acting inhibited participant’s ability to experience positive mental health, such as peace of mind.
I’m interested in helping others … I know what it was like to be so alone, crying in the corner and not having anyone there and maybe … I can be there for someone else on the spectrum.—Nicole
But I think as Autistics we have to stand up, because otherwise we become victims and … when we have experience being a victim of something, making sure it doesn’t happen again, either yourself or witnessing someone else be a victim.—Quinn
Theme 2: Body and mind
Subtheme 1: Significance of sensory input
Many participants recalled the impacts of sensory overload. Pre-diagnosis, the impact of too much sensory input on their well-being was severe as they lacked the understanding of why their body reacted in the way it did. Some participants described somatic reactions to their environment, which caused distress, impacting negatively on their mental health.
[Pre-diagnosis incident] But sound, the echoes, just all of the stuff happening … And then I’d go into a panic attack where I couldn’t breathe. And then I thought I was having a heart attack … Until the whole autism like lightbulb moment … I just thought I was mental.—Betty
The signs of sensory overload varied greatly between participants, and the recovery process varied depending on the duration and intensity of the sensory input.
So, in the last burnout that I had … I actually became nonverbal. Because I my brain just could not. I can’t really explain it … I didn’t want to write any words or read any words … the sensory input was too much.—Nicole
Post-diagnosis, participants described how they were better equipped to recognize the negative cumulative effects of sensory and social input. This allowed them to seek accommodations in the workplace or adjust their lifestyle to prevent adverse reactions, such as burnout or meltdowns. Understanding their sensory profiles allowed participants to budget their “energy reserves” and empowered them to avoid situations that they recognized as “just something that [they] can’t do”—Paula and “it moves from something being something that [they] can’t control to something that [they] can control”—Emma.
Subtheme 2: Importance of physical health, sleep, diet, and exercise
Many participants expressed the concept that their physical health was directly linked with their mental health. Common topics included the importance of good sleep, a healthy diet, and exercise. Participants were usually particularly focused on one of these areas, though their focus and their strategies were all vastly different.
I still have problems with my executive functioning if I don’t sleep enough.—Ken
Joined the gym … I still go to group classes, and that’s like a really big part of my coping strategy.—Fiona
I’m very mindful of the actual, from personal experience of how important it is to actually have healthy food. By healthy I mean, really healthy, which is organic, free range… these are no luxuries, right. To me, this is the basic thing you need to have to be healthy in this world.—Liam
Subtheme 3: Co-occurring conditions exacerbate mental health challenges
Seventeen participants reported being diagnosed with conditions in addition to their autism diagnosis impacting their mental health. Thirteen participants had a diagnosis of attention-deficit hyperactivity disorder (ADHD), 2 had bipolar, 3 reported having post-traumatic stress disorder, 3 reported experiencing eating disorders, and 12 had a variety of physical conditions. These conditions complicated their mental health experiences.
A big part of it is exhaustion, the fatigue and constant pain, the sleep difficulties, all of it makes it harder to regulate. It [complex chronic physical health conditions] increases my stress which makes my executive functioning skills worse.—Sarah
But I do think that ADHD definitely adds to it. And just the feeling of being a total incompetence as a person. But I’m also very resourceful, as well. So, I have definitely found some ways around it, and to still get by.—Fiona
Subtheme 4: Executive functioning challenges
Many participants reported having challenges with their executive functioning skills, which then impacted on their mental health, particularly those also diagnosed with ADHD. Prior to their diagnosis participants saw their executive functioning difficulties as “character deficit,” negatively impacting their self-esteem.
Most of the negative experiences were before I realised that I have autism. And before I had strategies to manage my executive function.—Harry
Subtheme 5: Coping mechanisms for daily life
In order to mitigate negative mental health impacts of their various sensory and executive functioning challenges, participants utilized a range of strategies, supports, and assistive technologies. Sensory tools, such as fidget toys, assistance animals (including guinea pigs [Irene] and birds [Jane]), escapism through books or video games, hobbies, strict routines, planners, and organizational apps were utilized in managing their challenges.
Sometimes if we’re in the car I might knit, even if I don’t, just knowing I have that there, it’s almost like a safety blanket.—Nicole
And then you need time to calm down. So that’s where I started playing video games and doing RC (remote control) cars and going fishing a bit more, just to just to give myself that break.—Owen
Subtheme 6: Long-term impact of trauma and grief
Many participants reported experiencing trauma, abuse, and/or grief in their lives. These experiences negatively impact the participants’ mental health many years after the adverse events.
I developed trauma responses, which became strategies in which I was keeping myself safe, but they also worsened my well-being.—Paula
I have spent many years of therapy on this recently … I think I’m coming out … much better out of this … Just the therapy to deal with the stress and the trauma really.—Liam
Theme 3: Connections to family and community
Subtheme 1: Supportive relationships as a protective factor for positive mental health
This theme focused on how having at least one supportive relationship had a positive impact on participants’ mental health. The relationship could be with a parent, a sibling, a spouse, or a friend. Participants described how the support person provided guidance and safety, physically, socially, and emotionally. Participants reported these relationships made them feel “accepted,” and they found comfort in feeling understood by someone.
I think, having a wife there who not only understands you because she’s done so much research into this, but also supports and has it herself so she can be empathetic is a really big positive for me as well.—Harry
While many participants mentioned having few friends, if any, in primary school, most described how they were able to make strong, “safe” friendships in high school or beyond. The impact of these relationships in high school mitigated the effects of bullying, and it “just really breaks up the loneliness”—Reg. Friendships also provided an alternative support system separate from the family unit.
[Friends] I don’t think I would have gotten through high school without them. … I would have just been alone in the library by myself quite easily. But I had the luck of finding those people that I connected quite well to … that was a big impact on my self-confidence and just willingness to participate and come out of my shell.—Chloe
Not all family relationships were supportive, with participants reporting some relationships as negatively impacting their mental health. Several participants reported how they were content to no longer have contact with unsupportive family members, while others simply accepted that the relationships would not provide emotional support for them.
Subtheme 2: Parenting—a double-edged sword
While most of the participants who identified as parents reported good relationships with their children, the majority of whom were also autistic, they also described the impact of parenting on their mental health as both positive and negative. The phrase “double-edged sword” was used by multiple participants when referring to the impact of parenting on their mental health. Parenting brought the most joy, even to the point for one participant attributing parenthood to saving her life from a downward spiral into negative mental health and addiction. Fiona reported that she was “in such a good place” after accepting her child’s autistic identity, which was a “key factor” to overcome “all these things that [I’m] ashamed of.”
I think it’s been, it’s a double-edged sword. For me the parenting thing, it has been the hardest thing I’ve ever done, the most damaging thing for my mental health, undoubtedly. But without it, I wouldn’t know who I am. [Child] really brought me into this journey of finding out about myself.—Paula
One of the major factors that was consistently shared by the participants was the negative impact of sensory overload. For example, one participant (Harry) described their experience of sensory overload caused by the children being noisy causing the participant to “retreat to [their] room in complete meltdown,” which could then cause their child to get “upset” and which, in turn, would cause a “negative spiral,” resulting in “a very major negative impact on [their] mental health.” Multiple participants reported that the strategies that had helped prior to parenthood were no longer available to them once they had children.
Subtheme 3: Challenges of interacting with professionals
Participants reported a variety of interactions with professionals, which would impact their mental health accordingly. While there were some positive interactions reported, overall interactions with professionals were difficult, with most demonstrating a lack of understanding of the individual and autism. Awareness of their autism diagnosis, at times, resulted in the participant being patronized and undermined, particularly in medical settings, resulting in incorrect or delayed diagnoses.
I don’t feel comfortable disclosing that I’m autistic to the doctors I see. Because I actually don’t think they have a good understanding of autism either. And I think you get a lot of that. I mean, other health professionals where I have disclosed, allied health professionals, and I’ve got, “Oh, there’s no way you’re autistic.” Yeah. Because of that preconceived idea about what autism looks like, and it doesn’t look like us.—Quinn
In school settings, especially prior to an autism diagnosis, there was a wide variety of experiences, which impacted participants’ mental health. Even though there wasn’t a diagnosis, participants reported that teachers would misunderstand them or actively dislike them. For some participants though, they were able to build a rapport with their teachers as a result of their academic achievement in certain subjects, though even then the participants would be left feeling as though they were “letting them down in that time by struggling”—Emma.
For autistic parents interacting with the school system, participants reported a variety of interactions, ranging from a very positive and supportive school environment to teachers disregarding the parents’ lived experience, “being spoken over because they believe they’re the expert at every, at everything”—Quinn. Four participants homeschooled their children because of their negative experiences with the education system impacting both the participant’s and their children’s mental health.
Theme 4: Choice and control
Subtheme 1: Personalization of therapies
Participants reported having personal therapies or strategies that were helpful in managing their mental health. While no specific therapies were universally helpful to all participants, variations of talk therapy were described as beneficial by some. Therapies, such as cognitive behavioral therapy, were frequently described as ineffective unless the therapist adapted the therapy to the individual. One participant (Alex) described therapy as being “patronising” due to being told by therapists that certain strategies “aren’t what [they] should be doing” even though they were working.
Therapies described by participants as the most helpful were participant led and adapted to their unique cognitive styles. Participants described that when the therapist listened to the participant and understood their unique cognitive style, the participant had much greater success in developing personal strategies for managing their mental health.
I don’t feel like it’s all about the strategies that therapist uses. It’s actually about the relationship that the therapist has built with me before using the strategies.—Diana
Subtheme 2: Affordability and life choices
An important theme that arose was that of finances. Finances are a means to be able to make life choices that can enhance well-being, and without stable finances all other aspects of life were impacted.
If finances weren’t an issue, everything else could have been coped with, with so much more ease, it would have been a challenge and difficult, but it wouldn’t have been nearly as hard as it was.—Tina
You know, it was really having more money has totally taken away a lot of the depression issues. But when, when you are disabled, and when you are on a pension, and when you are neurodivergent and when executive function is a problem, you do get depressed, you get severely depressed.—Jane
Participants expressed how employment was beneficial to mental health but only under certain conditions. If the employment allowed the participant financial freedom to survive, or if the employment was related to a passion, then having employment became a protective factor for mental health. The work itself was not the goal but rather a means to be able to live a fulfilling life.
I’ve always loved programming, I’ve loved the challenge of, of problem solving every day. And I love the feeling of being good at what I do … That’s satisfying … I think it certainly helps given the financial responsibility of life.—Harry
For other participants employment was “detrimental to mental health.” Many struggled to work and found the environment too overwhelming from sensory and social factors. Most participants who could work reported that, without accommodations, they could only remain in any given position for a short amount of time before becoming overwhelmed by sensory and social input resulting in burnout.
it’s just maintaining that job. Not, not from doing anything wrong at the job but my own, you know, I tend to just fade about four and a half years is the longest I’ve been at one job.—Nicole
The impact of being overwhelmed by the sensory and social environment was mitigated when the workplace provided a “supportive environment” and “flexibility.” Employers being aware of their autistic identity and sensory profile enabled participants to advocate for their needs in the workplace and reduce the social demands as needed.
Subtheme 3: Disability support mechanisms
Participants all reported that having support, be it financial, emotional, or physical, was highly significant to their mental health.
So, I, you know, I really do think that the biggest factor in my life hasn’t been strategies, it’s been those sorts of supports.—Alex
Many of the participants reported accessing or attempting to access formal disability supports, such as the NDIS. For several participants, they were able to access the NDIS and have been able to engage support workers, cleaners, and/or therapists, which “has been life changing,” improving their overall well-being significantly.
However, several participants described being denied disability supports, negatively impacting their mental health.
The stress of advocacy, dealing with the NDIS has caused a lot of issues, going through that process with dealing with the Administrative Appeals Tribunal (AAT) trying to fight for the necessary and reasonable supports for having a disability, both for myself and for my kids.—Sarah
Discussion
Mental illness is a leading global concern for many autistic individuals, with suicide reported to be approximately three times more likely for autistic people than the general population. 12 This autistic-led, coproduced study explored the lived experience of autistic mental health. Exploration of the lived experience involved consideration of mental health through relevant factors including childhood through to the present, family, romantic and peer relationships, educational and employment experiences, physical health, and autism diagnosis and subsequent support.
The impact of discovering one’s autistic identity and the need to hide one’s autistic traits through adaptive morphing was a dominant theme of this research. Participants shared how receiving an autism diagnosis led them on a journey of self-discovery, which improved their self-acceptance and mental well-being. This is in line with recent literature that demonstrates how a late autism diagnosis leads to improved self-awareness, allowing for the development of coping strategies including self-acceptance and self-compassion.60,61 Participants who were diagnosed during adolescence reported that receiving their diagnosis was challenging, and although they struggled with their autistic identity at the time, as adults, their journey to self-acceptance continued as they joined the autistic community, found a sense of belonging, and embraced their autistic identity. Positive autistic social identity may then be understood as a protective mechanism for positive mental health. 62 Similarly, adaptive morphing has been linked to poor mental health outcomes including autistic burnout. 40 Participants reported on the emotional toll of adaptive morphing around family and professionals, highlighting the need for improved understanding of autistic traits by those supporting autistic individuals and the wider community in general. This finding is important as it echoes the current need for therapies and education that respects autistic identity, moving away from an adaptive morphing paradigm, which has been associated with trauma, anxiety, depression, and low self-esteem. 63
Supportive relationships, environments, and social connectedness play an important role in promoting autistic mental health. 64 Participants described the crucial role those supportive relationships played in their lives, providing a sense of safety, with many directly attributing their well-being to those relationships. This finding is consistent with research demonstrating that social acceptance and support positively impact autistic individuals’ mental health and well-being, resulting in increased self-esteem and sense of belonging to the community. 65 This is an important consideration for health professionals when planning supports. The stigma associated with an autism diagnosis continues to negatively impact autistic individuals.66,67 Participants in the present study described their need for a socially supportive culture in educational and employment settings, as well as their need for environmental accommodations and flexibility. Positive mental health outcomes for autistic individuals have been demonstrated through cultures of inclusion and connectedness in schools 68 and through flexibility and supportive flexible workplaces. 69 Negative attitudes toward autism can be improved through education about autism and increased societal acceptance.25,70 Findings highlight the importance of educating not only the autistic individual but also those in their support network. This need aligns with current paradigms around neurodiversity and a need for acceptance and respect. 71
Sensory differences have recently been shown to contribute to poor mental health in autistic adults, 72 even to the extent of producing somatic reactions. 73 Participants for this study reported sensory input directly impacted virtually every aspect of their lives, particularly when engaging in education, working, and parenting, when their ability to escape the sensory overload was restricted.
Participants also reported how the challenges of executive dysfunction contributed to the state of their mental health through the effect on multiple aspects of life, including their ability to work or care for themselves and others. Challenges with executive functioning and difficulties in emotion processing are associated with lower quality of life in autistic young adults. 74 The interrelatedness of sensory input and executive functioning and their impact on other areas of an individual’s life require consideration when planning mental health assessments and interventions for autistic individuals. Participants reported that when their challenges and support needs were accommodated in the workplace, they experienced positive well-being. When factors such as executive functioning challenges are accommodated in the workplace, productivity is found to increase, 75 and success in the workplace improves feelings of being valued and accepted while providing financial independence 76
Maintaining good physical health through healthy sleep, diet, and exercise habits contributes to positive mental well-being. 77 Participants expressed their need to engage in healthy lifestyle habits, such as strict sleep schedules, attending the gym, or healthy eating in order to maintain positive mental health. Prior research shows that autistic adults are more likely to have unhealthy diet, exercise, and sleep patterns, as well as being more likely to experience co-occurring physical conditions than non-autistic adults. 78 In this study, 17 participants reported having a co-occurring condition, 12 of whom had a physical condition, which is in line with previous studies that found autistic people have a higher prevalence of physical health conditions than the general population. 79 When considering mental health, it is important to consider the direct and indirect effects that physical health has on mental health. 80 Participants expressed how they managed co-occurring physical conditions utilizing an array of strategies unique to each individual, including exercise routine and diet management. Individuals may benefit from exploration of tailor-made lifestyle and support choices that are best suited to their situation and needs. There cannot be a one-size-fits-all approach, and supports given to individuals need to account for the variability of their personal requirements and co-occurring conditions. 81
Vulnerability of autistic adults to negative life experiences may diminish mental health and life satisfaction. 82 Participants reported experiencing various forms of mental illness and distress for many years due to negative life events and the abusive actions of others. Autistic individuals experience high rates of trauma and sexual and physical assault.83,84 Participants described how these traumatic negative life events led to long-term suffering and negative life outcomes such as mental illness and maladaptive coping mechanisms. Understanding vulnerability and trauma requires specialized skills and knowledge to be able to provide appropriate support and/or therapy. 85 A potential consideration to meet these needs is to provide specialized, trauma-informed mental health support targeting autistic individuals. 86
In Australia, the majority of funding for autism supports come from the NDIS. 87 Participants of this study reported varied accounts of their experiences of receiving support through the NDIS and the impact this had on their mental health. The findings from this study demonstrated that there is inconsistency in the support provided to autistic adults through official support providers. Reviews of the scheme have highlighted inconsistencies in the supports provided by the NDIS where some NDIS participants received adequate funding required to achieve positive outcomes and increased community participation, while other NDIS participants did not receive the required funding to meet their needs. 88 The outcome of the inconsistencies reported by participants in this project was that while some individuals experienced enhanced mental well-being by being well supported, others experienced distress consistent with previous findings that determined that some NDIS participants experience administrative burden 89 and the inability to access funding for necessary supports. 90
The autistic individuals interviewed for this project had complex and unique circumstances, as well as sensory profiles, which require customized approaches. A common theme among participants was the need for personalized therapies. Autistic people are often not believed when attempting to advocate for their needs. 91 Participants reported that when therapists applied a one-size-fits-all approach, it was counterproductive as it demonstrated a lack of understanding, and the resulting patronizing attitudes reduced the mental well-being of the participants. There is no one-size-fits-all approach to the therapy; the therapy needs to be adapted to the autistic individual and be neurodiversity affirming.8,92
The recovery model for mental health emphasizes the need for the consumer to have control over their own recovery from mental illness rather than the control being in the hands of the clinician as set out by the biomedical model. 93 This concept of control, or empowerment, is described as one of the five processes for recovery in the conceptual framework underpinning the recovery model. 94 The concept is consistent with the findings of this research, in that even though the individual, or consumer, may experience alexithymia or poor interoception, participants demonstrated proficient self-awareness to be considered the expert of their own mind and able to recognize their own needs.
This study provides an important contribution to the understanding of autistic mental health as described by autistic people themselves. The findings demonstrate the nuance that distinguishes critical factors of autistic mental health from that of the general population. The concepts of self-identity, sensory input, and individualized neuro-affirming supports are of particular importance for supporting autistic mental health. These findings support and confirm the recent findings of other qualitative studies such as those investigating quality of life,43,44 impact of parenting, 95 adaptive morphing, 96 and sensory processing 31 while providing an overarching view of mental health, particularly the interrelatedness of the themes.
Limitations and future research
Limitations of this research include the demographic aspects. Specifically, even though purposive sampling was used, the ratio of male-to-female engagement with the research is disproportionate to the ratio of diagnosis in Australia at this time. Recent research shows a gender bias in the diagnostic process, which, if accounted for, would produce a ratio of three males to every four females. 97 This study, however, had a large response for expression of interest by females, and the researchers actively recruited male participants to overcome this imbalance. Despite this, the final sample is significantly shy of the diagnosed ratio of 3.5 males per female. 3
vAnother demographic limitation of this study is the age of diagnosis. While there are no statistics available by the Australian Bureau of Statistics for Australia, globally it is estimated that the current average age of diagnosis for the Autism Spectrum is 5 years old. 98 In this study, the lowest age of diagnosis was 15 years old, meaning that this study is only representative of autistic individuals who were late diagnosed (i.e., diagnosed in adolescence or adulthood) and therefore missed the opportunity for appropriate supports during the formative years. The mental health of autistic individuals who were diagnosed at a younger age and did receive supports is therefore an area for further study. The authors also recognize that requiring a diagnosis excluded those who are self-diagnosed autistic, and this privileges the experience of those who were able to access and afford diagnostic services. Future research should explore the experiences of individuals who self-diagnose.
Screening for emotional distress limited the recruitment of participants to those who are currently experiencing better mental health than many in the autistic community. Poor mental health is well established in prior research, 99 and as such by screening those individuals at risk of adverse reactions to participating, the study will naturally be skewed toward those who are currently well supported and thriving. Also, several participants reported having experienced extreme financial distress in the past, but none were in financial distress at the time of the interview. This could skew the results away from the impact of financial security on well-being, as those with less stable finances may not be able to afford an official diagnosis and also may be less likely to be eligible for this type of research project due to finance induced emotional distress. 100
Footnotes
Acknowledgment
The authors would like to thank members of the consumer steering group and the study participants for their time and involvement.
Authorship Confirmation Statement
This work will contribute to a Master of Philosophy degree for K.B. All authors conceptualized this work. K.B. was responsible for collection and curation of the data. K.B. analyzed the data under the supervision and mentorship of B.M., W.L., S.G., S.M., and M.S. K.B. wrote the original draft, and B.M., W.L., and S.G. contributed to the review and editing of the article. The article has been submitted solely to Autism in Adulthood.
Ethical Approval
Ethical approval was obtained by the Curtin University Human Research Ethics Committee (HRE2021-0265), Perth, Western Australia.
Informed Consent
Informed consent was obtained from all participants included in the study. Participants were provided with information outlining the aims and procedures of the study prior to providing written informed consent to participate and informed of their ability to withdraw from the study at any point without the provision of justification or prejudice. All names have been changed for confidentiality.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received in relation to this research study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.