
Abstract
Background:
The self-reported experience of itch for autistic people has not been studied. Anecdote, theory, and emerging research suggest that itch experience is different in autistic people, with negative consequences.
Methods:
An online survey was completed by participants who self-categorized as diagnosed autistic (n = 158), self-identified autistic (n = 37), or not autistic (n = 85). We asked about three categories of itch, namely, spontaneous, provoked, and itch caused by a medical condition, with questions focused on severity, timing and duration, and impact on daily activities.
Results:
Across all categories of itch there was a pattern of greater severity, duration, and impact in diagnosed autistic people compared with non-autistic people. Those with self-identified autism largely fell between the diagnosed autistic and not autistic groups. Itch severity was associated with self-reported autistic traits. As expected, we found more dermatitis-related itch in autistic respondents, but this did not drive differences in spontaneous and provoked itch.
Conclusion:
Findings suggest that the self-reported itch experience of autistic people is more severe, longer lasting, and of greater daily relevance, differences that cannot be attributed to the higher prevalence of skin dermatitis found in autism. Future studies are required to understand itch experience within the broader picture of sensory differences, and to develop management strategies for what can be a highly morbid experience.
Community Brief
What was the purpose of this study?
Differences in sensory experiences in autistic people are well documented. However, the experience of itch for autistic people has been largely unresearched. Our study is the first to formally ask “Is itch experience different for autistic people?”
Why is this an important issue?
It is known that sensory differences can have a notable impact on autistic peoples’ quality of life. It is also known that long-term itch can be detrimental to physical and mental health. What isn’t known is whether autistic people suffer itch, with its negative impacts, more than non-autistic people.
What did the researchers do?
We distributed an international online survey that asked autistic and non-autistic adults about their experience of itch and the impact of itch on daily life. We asked about three types of itch: (1) spontaneous itch, (2) itch provoked by either contact with others, objects, hot and cold items, or itch experienced instead of pain, and (3) itch caused by medical conditions.
What were the results of the study?
Autistic adults reported significantly greater itch severity and itch-related impact on their daily life for all itch types. Heightened spontaneous and provoked itch experience in autistic people was not explained by higher rates of eczema-related itch.
What do these findings add to what was already known?
As the first of its kind, our study highlights that itch experience is different in autistic versus non- autistic adults.
What are potential weaknesses in the study?
Our study population was predominantly females older than 30 years, all of whom could access and complete an online survey. It will therefore be important to validate the findings in other autistic populations.
How will these findings help autistic adults now or in the future?
These new findings highlight the need to better understand the experience of itch for autistic people and are the foundation for beginning to translate this into support for autistic people who are being negatively impacted by itch.
Background
Itch, “… a sensation in the skin that provokes the desire to scratch,” can vary from a mild and transitory annoyance to a distressing and chronic experience. 1 When itch is experienced as distressing, it has been associated with poorer quality of life, including depressed mood. 2 Despite differences in sensory experience between autistic and non-autistic people being commonly described, 3 the experience of itch for autistic people is little explored. Itch can be described as an interoceptive sensation, which refers to sensations that convey information about one’s “physiological condition.” 4 Interoceptive sensations are distinct from exteroceptive sensory modalities that inform people about the external world (such as discriminative touch). Differences between autistic and non-autistic people have been reported for the interoceptive somatosensory modalities of pain, temperature, and affective touch,5–8 however, the interoceptive experience of itch for autistic people remains largely unexplored.
Somatosensory interoceptive modalities have a common neurobiology: peripheral, unmyelinated c-fibers synapsing in the superficial layers of spinal cord dorsal horn. They are also known to interact at multiple levels of the nervous system.9–18 Many theories of autistic perception predict the existence of interoceptive differences,19,20 and in light of the multimodal interoceptive differences found in autistic people, 19 it would be surprising if itch experience were unaffected. It is important to note that exteroceptive sensory systems are also affected in autism, and a global mechanism might be driving interoceptive and exteroceptive changes in sensory sensitivity processing in autism (e.g., see Monday et al. 2023 21 ). Furthermore, a recent study has suggested a genetic link between itch and autism in a knockout mouse model of CNTNAP2. 22
Aside from neurobiological and mechanistic predictions, there is also limited but compelling evidence that itch experience is different for autistic people. Anecdotal, autobiographical reports from autistic adults make mention of itch, including Temple Grandin’s accounts (Grandin, 1996, 2008).23,24 However, these allusions to a different, and often notably unpleasant, itch experience for autistic people have not been followed-up with research studies. This is perhaps due to a passive assimilation of “itch” under other terminology, such as “tactile defensiveness,” 25 “self-injurious behavior,” 26 “hypersensitivity” (archetypically to clothes labels), 27 and “repetitive behaviors.” 28 Indeed, the importance of efforts to formulate a standardized taxonomy to aid future autism sensory research have been highlighted elsewhere. 29 Kyriacou et al. (2021) presented qualitative data on the autistic experience of itch in relation to textiles, and highlighted some of the negative consequences of itch, such as self-injurious scratching. 27 However, textile-provoked itch hypersensitivity was not explored as a separate autistic phenomenon and was nested under “tactile defensiveness” and “hyper-responsiveness” terminology. 27 The only study to explicitly quantify itch in autism is by Helt et al. (2021), who explored the phenomenon of “itch contagion,” which refers to itch that is elicited when watching others scratch. 30 Their baseline data confirmed that autistic children scratch more often than age-matched controls, and that scratching increased more for autistic children when exposed to images of others scratching.
The current study
Despite theoretical, physiological, and anecdotal accounts converging to suggest that the experience of itch may be different for autistic people, there has been very little exploration of self-reported experiences of itch. The aim of the current study was to address this need by conducting an international survey of itch experience in autistic and non-autistic people.
We used a bespoke online survey that drew on items in the 5D Itch Scale 31 to explore the experiences of three types of itch: provoked, spontaneous, and medically induced. Provoked itch refers to an experience of itch that is provoked by an external stimulus. We included itch provoked by textiles, reflecting reports from autistic adults of problematic itch induced by clothing. 27 Based on existing understanding of the neurobiology of interoceptive somatosensory modalities (Craig, 2003; Marshall et al., 2019),4,32 we also asked about itch provoked by activation of other c-fiber modalities, such as contact with hot or cold objects, social touch, or pain. For completeness, we also asked about itch provoked by contact with any object.
We additionally asked about itch occurring without provocation (i.e., spontaneous itch). There are suggestions that autistic people have difficulty attenuating interoceptive information, 20 which could increase vulnerability to spontaneous itch.
Our final category focused on medical causes of itch, reflecting that itch can be caused by a wide range of medical conditions, including psoriasis, dermatitis (including eczema), liver disease, and diabetes. 33 Autistic people have higher rates of poor physical health compared with non-autistic people, 34 and autistic people have repeatedly been shown to be at greater risk of atopic dermatitis compared with non-autistic people. 35
To gain a breadth of insight, our survey asked respondents to reflect on the severity, timing and duration, and impact on daily life of each type of itch. Based on previous theoretical, physiological, and anecdotal accounts, we predicted that the experience of each type of itch would be significantly more pronounced in autistic adults compared with non-autistic adults. We additionally predicted that people with dermatitis would be more susceptible to other forms of spontaneous and provoked itch (i.e., induced hypersensitivity) compared with those without dermatitis and that dermatitis would be overrepresented in autistic adults. 36 This follows the predictions by Helt et al. (2021) who note that contagious itch is heightened in those with atopic dermatitis,30,37 and the predictions of Mishra et al. (2022) who speculate a common genetic cause for dermatitis and autism. 22 We also collected self-report of autistic traits and general sensory differences, to explore their association with itch phenomena. We predicted that itch features would positively correlate with autistic traits and sensory features. Finally, in light of known associations between itch and anxiety and between anxiety and autism, an exploratory analysis was undertaken to look at the relationship between reported itch and anxiety diagnosis (Hollocks et al 2019; Sanders & Akiyama, 2018).38,39
Methods
Participants
Our online survey was launched out of the following two autism research centers: Wales Autism Research Centre (UK) and Olga Tennison Autism Research Centre (Australia). It was disseminated via means of research databases (academic and charitable, including Autistica: https://www.autistica.org.uk/) and via social media posts (TwitterTM and FacebookTM). Participants were invited to take part if they were older than 18 years and autistic or non-autistic. People who took part were invited to take part in a prize draw to win one of several cash prizes (GBP£50 or AUS$90).
We received 280 fully completed responses. Based on participants’ self-report, we categorized them into three groups as follows: Clinically diagnosed as autistic (AUT-D; n = 158); self-identified autistic (AUT-S; n = 37); not autistic (N-AUT; n = 85). Age, sex, and educational attainment did not differ across groups; White ethnicities were overrepresented in AUT-D. There was a lower proportion of AUT-D to N-AUT in Australian participants compared with the United Kingdom. Details of demographics are shown in Table 1 and Supplementary Table S5A, S5B.
Participant Characteristics
Slightly right-skewed (Shapiro–Wilk p < 0.01).
ANOVA, p < 0.01; post hoc Tukey, all comparisons, p < 0.01.
Chi-square, p < 0.01; post hoc comparison, p < 0.01 for AUT-D versus N-AUT, including when limited to the United Kingdom and Australia.
The Short Autism Quotient; GSQ, Glasgow Sensory Questionnaire; U.K., the United Kingdom; Aus., Australia; AUT-D, diagnosed autistic; AUT-S, self-identified autism; N-AUT, not autistic.
Institutional review board approval
Our study was ethically approved by the Cardiff University School of Psychology Research Ethics Committee (EC.21.10.12.6416R), with reciprocal ethical approval from the La Trobe University.
Materials
Demographic questions
We collected data on age, gender, sex, country or residence, ethnicity, and education level. Additional questions asked whether participants had a clinical diagnosis of autism or self-identified as autistic, as well as whether they have ever been diagnosed with a range of medical, neurodevelopmental, and psychiatric conditions (see Supplementary Table S5C). Each participant was able to select multiple conditions. AUT-D had higher proportions of diagnosed anxiety (AUT-D: 74%; AUT-S: 46%; N-AUT: 33%; χ2 p < 0.01), depression (AUT-D: 66%; AUT-S: 35%; N-AUT: 24%; χ2 p < 0.01), and asthma (AUT-D: 20%; AUT-S: 16%; N-AUT: 5%; χ2 p < 0.01).
Itch survey
Questions about itch experience were adapted from a previously validated measure used to evaluate medical causes of itch, the 5D Itch Scale. 31
Domains of Itch Measured
Our itch survey adapted four domains from the 5D Itch Scale: Duration, Degree, Disability, and Distribution. Data on the distribution of itch (i.e., where on the body itch was experienced) were captured but will be reported elsewhere. We reformulated the remaining three domains as follows: severity (Degree), timing and duration (Duration), and impact (Disability), asking about a person’s lifetime experience (“…at any point now or in the past…”) rather than “during the past 2 weeks” as in the 5D Itch Scale. Most questions recorded responses on a Likert scale, with scales adjusted from the original where necessary to reflect our specific aims.
Severity of itch was measured by asking about the “greatest intensity” of itch experienced, which ranged from 1 (mild) to 4 (very severe).
Timing and duration of itch was measured using three questions: the duration of the longest period of continuous itch [longest episode; ranging from 1 = less than 6 hours a day to 5 = all day (or more)]; the longest duration of episodes (longest cluster; ranging from 1 = up to 1 week to 6 = more than 5 years); and how long ago the most recent episode was experienced (most recent episode; ranging from 1 = within the last week to 6 = longer than 5 years ago).
The impact of current or prior itch on four different activities was measured. These were as follows: sleep, leisure or sports activities, housework or errands, work or school activities. For the latter three activities, the options ranged from 0 = never affects this activity to 4 = always affects this activity, with an N/A response also available. For sleep, the choices ranged from 0 = never affected sleep to 4 = delayed falling asleep and frequently wakes me up at night.
Categories of itch measured
The survey questions were presented in a fixed order for the following three separate categories of itch: spontaneous itch; provoked itch; and medical itch. The itch categories were presented in a random order. For spontaneous itch, participants were asked: “Have you ever felt itchy (or wanted to scratch) for no obvious reason?” to which they could respond “yes” or “no.” If yes, they were then presented with the questions probing severity, timing and duration, and impact.
For provoked itch, participants were asked: “Have you ever felt itchy (or wanted to scratch) when something or someone touches (or injures) your skin?” If yes, participants were asked to select the subtypes of provoked itch that reflected their experiences (Table 2). Multiple subtypes of provoked itch could be selected. They were then asked about each subtype in turn using severity, timing and duration, and impact questions. For most analyses, provoked itch types were coalesced and analyzed as a single, parent category (provoked itch), alongside analyses of subtypes.
Medical and Provoked Itch Subtypes, Participant Counts, and Additional Information
N = Participant counts for itch subtypes.
For itch of medical cause, participants were asked: “Have you ever felt itchy (or wanted to scratch) because of a medical condition, for example, eczema?” As for provoked itch, those identifying an itch of medical cause were asked to further specify its cause (Table 2). Multiple subtypes of medical itch could be selected. Subsequently, they were then asked about each subtype in turn using the severity, timing and duration, and impact questions. For the purposes of analysis, medical itch categories were coalesced into a single, parent category (medical itch), as well as into broad subcategories (Table 2).
Throughout the survey, free-text questions were also asked about each itch (e.g., “Can you describe this itch in more detail?”). These data will be analyzed separately.
Other measures
Additional validated measures were presented after completion of the itch questions. The 10-item version of the Autism Spectrum Quotient (AQ-10) 40 was administered to measure autistic traits. Scores can range from 1 to 10, with a higher score indicating more autism traits. Clinical guidelines recommend score >5 should prompt referral for autism assessment. We opted for this over the full 50-question Autism Quotient (AQ) 41 to reduce dropout from questionnaire fatigue. The Glasgow Sensory Questionnaire (GSQ) 42 was administered to explore general sensory features related to autism. This is a 42-item questionnaire covering 12 sensory domains. Within each domain there are two questions, one probing hyposensitivity and the other hypersensitivity. Scores can range from 0 to 168, with higher scores indicating more autism-related sensory features. Floor and ceiling effects for AQ-10 were present: highest (ceiling; AQ-10 = 10) values made up 15.1% of scores, while lowest (floor; AQ-10 = 0) values made up 3% of scores. GSQ did not have floor or ceiling effects.
Analysis and statistics
Participant characteristics
Age and performance on the AQ-10 and GSQ were compared across groups using one-way ANOVA, with post hoc Tukey testing. Sex differences were evaluated with chi-square. Normal distribution of data was assessed using the Shapiro–Wilk test.
Itch counts
Alongside the measures of severity, timing and duration, and impact, we wanted to the explore the frequency with which itch was reported across groups. We calculated the number of participants reporting each itch type (total participant count), and the number of itch types per participant (itch count per participant, inclusive of subtypes).
Total participant counts were compared across groups and evaluated with chi-square. Post hoc paired chi-squares were performed where whole-group chi-squares were significant and Bonferroni corrected for multiple comparisons.
Itch counts per participant were non-normally distributed and therefore compared across groups using Kruskal–Wallis chi-square and post hoc pairwise Wilcoxon signed rank-sum test, Bonferroni corrected for multiple comparisons.
Comparisons of itch metrics across groups
Severity, timing and duration, and impact were compared across the three groups, collapsed across all categories of itch and for separate parent itch categories and itch subtypes. The normality of itch severity, timing and duration, and impact scores could not be assumed. 43 Furthermore, Likert scale-type data are traditionally assessed with nonparametric tests. Therefore, Likert scores for the itch categories were compared using the omnibus Kruskal–Wallis chi-square. Post hoc testing was performed using pairwise Wilcoxon signed rank-sum test and Bonferroni corrected for multiple comparisons.
Means were reported as we felt these better represent numerically small differences between groups for low-resolution Likert scales. Where itch types were coalesced into a parent category, within-participant maxima were used as the summary statistic. Those stating an absence of an itch type, at any point now or in the past, were given an “anytime” itch severity of zero. Where an itch type was identified but a Likert scale metric was not completed, or an available N/A option was selected, these were excluded from statistical evaluation.
Comparisons of itch metrics across itch categories
Comparisons of severity, timing and duration, and impact measures across the three itch categories were performed using chi-square comparison of proportions and Kruskal–Wallis chi-squares. Detailed results of these comparisons can be found in the Supplementary Data.
Influence of dermatitis
To ascertain the effect of dermatitis, known to be more prevalent in autistic people, a medical subcategory “dermatitis” was formed. This combined the medical itch subtypes of eczema and contact dermatitis.
We compared dermatitis participant counts across groups and evaluated with chi-squares. Then, having excluded participants reporting dermatitis from our dataset, we reran count and severity, timing/duration, and impact analyses for spontaneous and provoked forms of itch, and compared metrics with and without dermatitis sufferers with the Mann–Whitney U test.
Influence of anxiety and other diagnosed conditions
We compared participant counts of diagnosed conditions across groups, evaluated with chi-square. Severity metrics, with and without diagnosed conditions, were compared with Kruskal–Wallis.
Relationship between itch metrics and autistic and sensory traits
Correlations between the AQ-10 and GSQ with itch severity, timing/duration, and impact measures were evaluated with Spearman’s rho (ρ).
Following this, manual hierarchical linear regression models were used to explore the relationships between itch characteristics and the AQ-10 and GSQ. The process was not automated, and its end-goal was not to produce the most-predictive model but rather to facilitate understanding of the associations within this explorative and highly nested dataset. To encourage unbiased inference, every iteration of the hierarchical regression model is provided in Supplementary Tables S11 and S12. The variance inflation factor was calculated for every independent variable within each model; none exceeded our cutoff of 5, and therefore, no independent variables were excluded on the grounds of colinearity.
Two sets of manual hierarchical linear regression models were built. The first set of regression models used the AQ-10 or GSQ as the outcome variable. These were built iteratively, initially including all three itch categories as predictor variables and taking each type of itch characteristic in turn (i.e., severity, timing/duration, impact). At each iteration, predictor variables with p values that were below statistical significance (defined as p < 0.05) were removed while retaining and exploding into subtypes (where possible, e.g., provoked subtypes) other variables. At each stage, the explanatory power of the model was reassessed (adjusted R2), with the aim of optimizing this value. Our purpose in optimizing R2 was to provide a window into meaningful associations within our explorative dataset rather than to build the most-predictive model (e.g., to test on a future dataset). This is important to note as artificial inflation of R2 is an inevitable consequence of using an iterative approach. 44 Again, because of the explorative nature of these models, model p values were not corrected for multiple comparisons (all raw p values can be found in Supplementary Tables S11 and S12).
Combined models, taking the most predictive itch categories and characteristics from subordinate models, were also evaluated. The effect of coregressing group, AQ-10 (for GSQ models) and GSQ (for AQ-10 models), was also assessed and compared with models built with these regressors alone.
For all regression model independent variables, an absent value (i.e., because of omission or irrelevance) was substituted with a zero. Impact categories were summed to create a “total impact” score for the purposes of regression.
Effect sizes and significance
Effect sizes were reported using Cramer’s V for chi-square, rank eta-squared for Kruskal–Wallis, and rank biserial for Mann–Whitney’s U. Significance was defined as p < 0.05. For post hoc tests, adjustment of p values for multiple comparisons was performed using the Bonferroni method.
Community involvement
The idea and impetus for this study were based on feedback from autistic participants we had previously worked with within other sensory studies. The charity Autistic UK aided in recruiting two autistic adults who advised on question relevance, appropriateness, and wording.
Results
Itch counts
Comparison of total participant counts across groups
Looking at the total participant counts across groups, itch was reported by more AUT-D participants compared with AUT-S and N-AUT [χ2 (2,265) = 81.00, p < 0.001]. All three itch categories had higher participant counts for AUT-D compared with N-AUT, and omnibus evaluations were all significant. Post hoc pairwise significant differences were demonstrated for spontaneous and provoked itch, but not for medical itch (see Supplementary Table S1A). Results are summarized in Figure 1, with the number of counts additionally tabulated in Supplementary Table S1B. Further analysis probed the participant counts for the subtypes of both provoked and medical itch. A similar pattern of participant counts across group was found for the provoked itch subtypes of material/clothing, objects, other’s touch, and instead of pain. These provoked itch subtypes had significantly higher counts for the AUT-D group compared with the N-AUT group (Supplementary Tables S6A and S7A). For medical itch subtypes, when coalesced into broad subcategories, the dermatological subcategory participant counts were different across groups, with significantly higher counts in AUT-D versus N-AUT post hoc (Supplementary Tables S6B and S7B). The other broad medical itch subcategories (Table 2) had no significant participant count differences across groups.
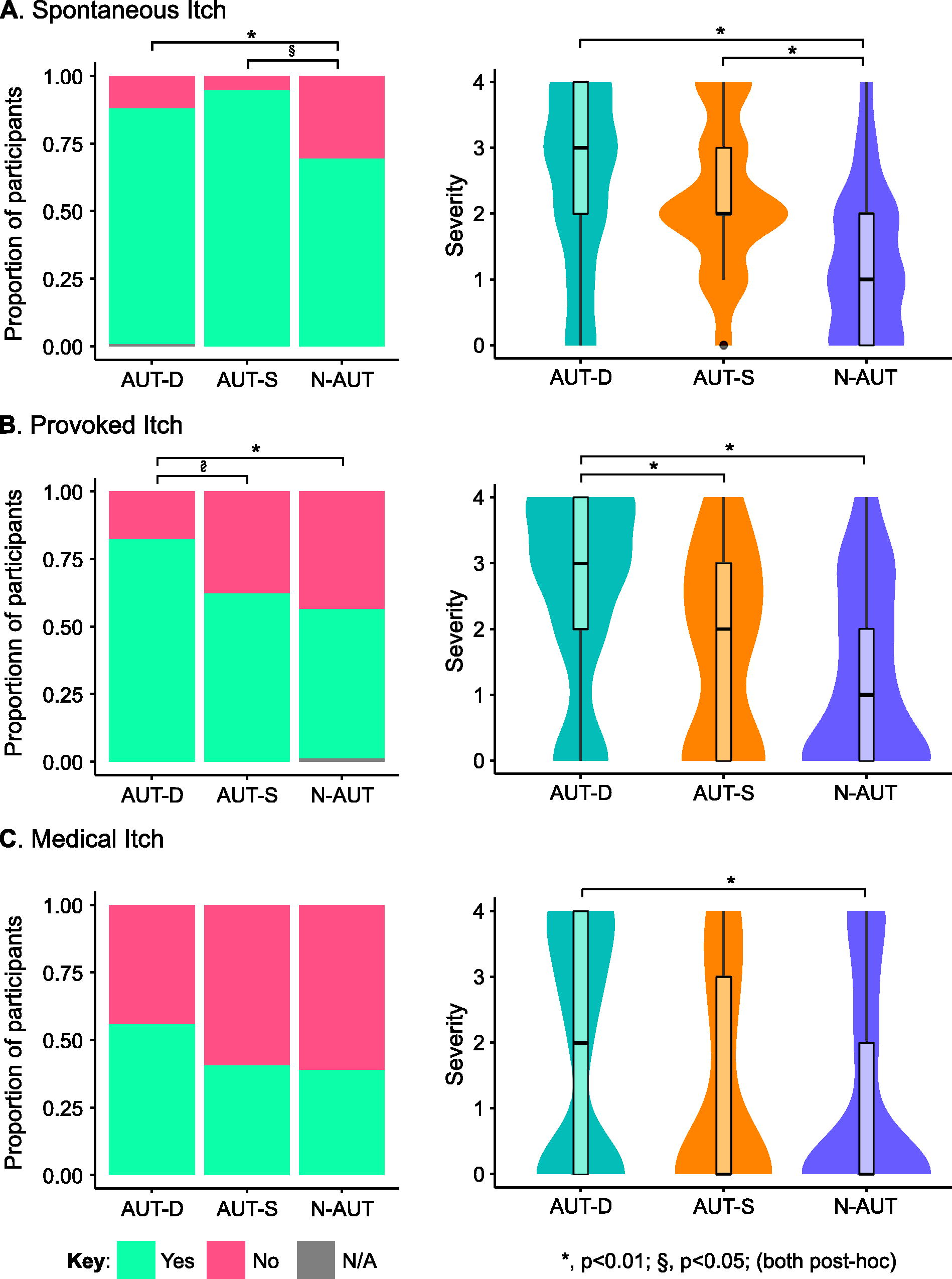
Proportion of participants reporting each itch type (participant counts) and severity of itch types by group. Severity was assessed by a 5-point scale with the following wording: 0 = no itching, 1 = mild, 2 = moderate, 3 = severe, 4 = very severe. AUT-D, diagnosed autistic; AUT-S, self-identified autism; N-AUT, not autistic.
Provoked and medical itch subtypes
The most commonly reported provoked itch subtype across all three groups was material/clothing (n = 169), followed by other’s touch (n = 103) and objects (n = 88), with fewer reporting itch instead of pain (n = 62), contact with warm or cold objects (n = 42), or other provoked causes (n = 24). Of those with itch in response to contact with warm or cold objects, the majority were in response to either hot or cold objects (n = 23), with fewer reporting itch in response to specifically warm (n = 12) or cold objects (n = 5) (Table 2).
Participants reported a total of 16 types of itch with medical cause (including other), the commonest was eczema (n = 83), followed by dry skin (n = 68), sunburn (n = 47), dandruff (n = 43), and contact dermatitis (n = 39) (Table 2).
Comparison of itch counts per participant across groups
The number of itch types reported per participant across all three categories was significantly different across the AUT-D, AUT-S, and N-AUT groups, with significantly more itch types per participant for AUT-D versus N-AUT [AUT-D, Md = 5; AUT-S, Md = 4, N-AUT, Md = 2; H(2) = 29.797, p < 0.001; post hoc: AUT-D vs. N-AUT, p < 0.001].
Itch severity
Comparison of severity across groups
Omnibus evaluation of severity revealed significant differences in severity between groups for all itch categories [spontaneous: H(2) = 44.39, η2 = 0.16, p < 0.001; provoked: H(2) = 42.56, η2 = 0.15; p < 0.001; medical: H(2) = 10.25, η2 = 0.03; p < 0.006], with significantly greater severity reported for AUT-D compared with N-AUT. Results are summarized in Figure 1 and Supplementary Table S2.
For provoked itch subtypes, similar patterns of significance were found for the material/clothing, objects, other’s touch, and instead of pain subtypes (Supplementary Table S8A). Of the medical itch subcategories, only dermatological itch showed significant differences across groups, with greater severity in AUT-D versus N-AUT (Supplementary Table S8B).
Timing and duration of itch
Comparison of timing and duration across groups
Omnibus evaluation of timings and durations showed significant differences across groups. For spontaneous itch, the longest episode of itch was significantly different between groups [H(2) = 13.07, η2 = 0.05, p < 0.001]. For provoked itch, the longest episode of itch, the longest cluster of itch, and the most recent episode of itch were all significantly different [longest episode: H(2) = 10.72, η2 = 0.04, p = 0.005; longest cluster: H(2) = 10.24, η2 = 0.04, p = 0.006; most recent: H(2) = 7.76, η2 = 0.03, p = 0.021], with significant differences in object and material subtypes for cluster length and most recent episode (Supplementary Tables S3 and Table S9A). In general, these reflected longer durations for AUT-D compared with N-AUT, although episodes were more recent for AUT-S. Results are summarized in Figure 2 and Supplementary Table S3.
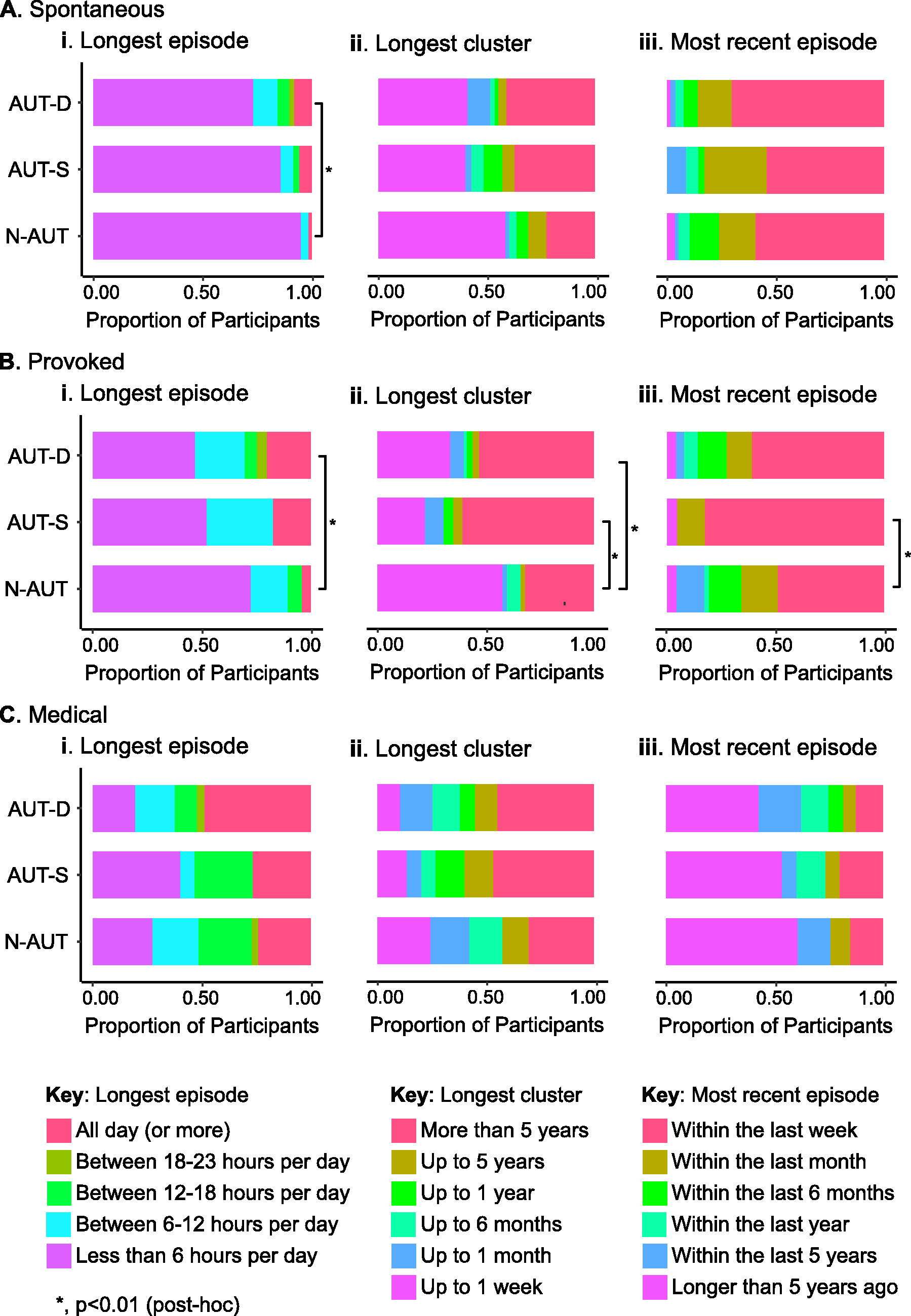
Duration and timing of itch categories by group. AUT-D, diagnosed autistic; AUT-S, self-identified autism; N-AUT, not autistic.
Although omnibus evaluation did not reveal significant differences for the medical itch, the dermatological subcategory demonstrated significantly longer episodes for AUT-D compared with AUT-S (Supplementary Table S9B).
Prevalence estimates of current itch (defined as “within the last week”) and chronic itch (defined as current itch of >4-week duration) are included in the Supplementary Data (Supplementary Table S13).
Impact of itch on everyday life
Comparison of impact of itch across groups
There were significant differences for all types of impact and within all itch categories across groups, with the exception of the impact of medical itch on sleep. The pattern of significance was driven by itch having a significantly greater impact on those in the AUT-D group compared with the N-AUT group. Here, post hoc comparisons were significant for all types of itch with the exception of the impact of medical itch on sleep and on work/school. The AUT-D group reported a significantly greater impact of itch compared with the AUT-S group on a more limited range of itch categories and impact types, most notably for housework where all itch categories had a significantly greater impact. There were only a few significant differences between the AUT-S and AUT-N groups. Results are summarized in Figure 3 and Supplementary Table S4.
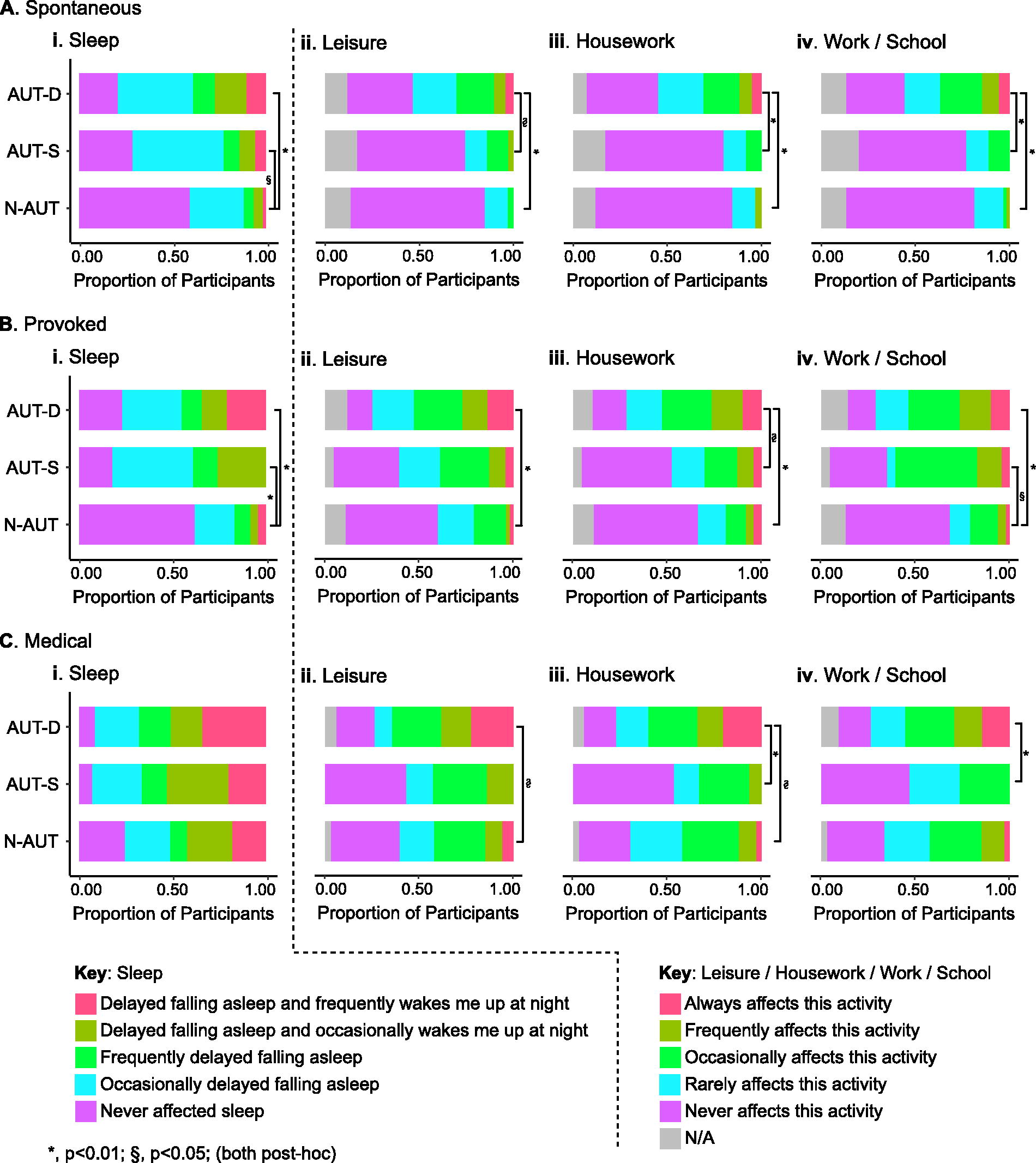
Impact of categories of itch on different aspects of everyday life by group. AUT-D, diagnosed autistic; AUT-S, self-identified autism; N-AUT, not autistic.
Provoked itch subtypes largely replicated that of the provoked itch parent category (Supplementary Table S10A). Notably, the dermatological medical itch subcategory showed significantly greater impacts for those in the AUT-D group, while no significant differences were found for other medical itch subcategories (Supplementary Table S10B).
Exploring the effect of dermatitis on nonmedical itch experience
There were 122 participants with dermatitis (formed by combining eczema with contact dermatitis). Counts were significantly different across groups [AUT-D 68/158, AUT-S 12/37, N-AUT 20/85; χ2 (2,280) = 9.36, Cramer’s V = 0.16, p = 0.009], with significantly more participants in the AUT-D group compared with the N-AUT group (post hoc; 43% vs. 23%; p = 0.012).
When excluding dermatitis sufferers from analysis of spontaneous and provoked itch counts, significant differences across groups (i.e., greater numbers in AUT-D) remained for provoked itch but not for spontaneous itch, with a reduced effect size (Cramer’s V, 0.16 with dermatitis excluded, previously 0.24).
When excluding dermatitis sufferers from analysis of spontaneous and provoked itch severity, significant differences remained for both (H(2) = 26.27, η2 = 0.14, p < 0.001 and H(2) = 28.16, η2 = 0.15, p < 0.001, respectively), with post hoc tests showing greater severity in AUT-D.
In addition, no significant differences were found between median severity scores for spontaneous or provoked itch. This was true for the whole sample, and for separate groups.
Exploring the association of anxiety and depression on itch experience
Anxiety and depression were significantly associated with the presence of spontaneous itch (χ2, both p < 0.05); anxiety, depression, and asthma were significantly associated with the presence of provoked itch (χ2, all p < 0.01); depression and asthma were significantly associated with the presence of medical itch (χ2, both p < 0.01). Severity was also significantly higher for those with an anxiety diagnosis for spontaneous and provoked itch (Kruskal–Wallis, p < 0.001), for those with depression for all itch types (Kruskal–Wallis, p < 0.001), and for asthma for provoked and medical itch types (Kruskal–Wallis, p < 0.01).
Exploring the relationship between the experience of itch and autistic traits and sensory differences
The AQ-10 and GSQ differed significantly across groups, with higher self-report of autistic traits and sensory differences in AUT-D versus AUT-S, and AUT-S versus N-AUT (Table 1). Severity, duration, and impact variables for parent itch categories positively correlated with AQ-10 and GSQ scores, with small but negative correlations for the most recent episode between spontaneous itch and AQ-10 and for both spontaneous and provoked itch and GSQ. AQ-10 scores for AUT-S were normally distributed (Shapiro test, p > 0.05), while AUT-D and N-AUT were non-normal, with skews consistent with ceiling and floor effects (respectively). See Supplementary Tables S11 and S12 for detailed iterative model outputs.
The relationship between autistic traits and itch features
Across all models, medical itch did not associate with autistic traits. Greater self-reported spontaneous and provoked itch severity were significantly associated with higher AQ-10 scores, producing a significant regression model that explained 27% of AQ-10 variance [Adj. R2 (2,270) = 0.27, p < 0.001].
Longer provoked itch episode durations were associated with higher scores on the AQ-10. The resultant significant model explained 10% of AQ-10 variance [Adj. R2 (2,276) = 0.10, p < 0.001].
Similarly, greater total impact from spontaneous itch and provoked itch caused by material/clothing was associated with greater AQ-10 scores and produced a significant model explaining 17% of AQ-10 variance [Adj. R2 (2,276) = 0.17, p < 0.001].
A combined model, including relevant severity, duration, and impact variables from earlier iterations, isolated greater severity scores (spontaneous and provoked itch) as the only variable significantly associated with higher AQ-10 scores [Adj. R2 (6,266) = 0.26, p < 0.001]. Their effects remained significant after controlling for the effect of group, and subsequent removal of spontaneous and itch severity variables led to a lower adjusted R2 (i.e., itch severity added explanatory power beyond the group effect). Adding GSQ scores to the model removed the significant effect of spontaneous itch, however, provoked itch remained significantly associated.
The relationship between sensory differences and itch features
Across all models, medical itch did not associate with sensory differences. Greater severity of spontaneous and provoked itch (material/clothing, other’s touch, objects, or instead of pain) were significantly associated with higher total GSQ score, explaining nearly 50% of GSQ variance [Adj. R2 (5,258) = 0.43, p < 0.001].
Longer duration of provoked itch episodes and longer duration of provoked and spontaneous clusters of itch episodes were all significantly associated with GSQ score, together explaining 23% of GSQ variance [Adj. R2 (3,273) = 0.23, p < 0.001].
Total impact from spontaneous itch and itch provoked by both material/clothing and other’s touch were significantly associated with GSQ, together explaining 40% of GSQ variance [Adj. R2 (3,273) = 0.40, p < 0.001].
A combined model, including relevant severity, duration, and impact variables from earlier iterations, explained greater variance. Within this model, greater severity of spontaneous itch and itch provoked by objects and instead of pain, and greater total impact of spontaneous itch associated with higher levels of sensory differences [Adj. R2 (4,261) = 0.43, p < 0.001]. The effect of these itch metrics remained significant after regressing out groups or AQ-10, and in both instances, the adjusted R-squared values were lower with itch measures excluded (i.e., itch severity and impact measures added predictive power beyond group).
Discussion
This is the first study to extensively and quantitatively explore the self-reported experience of itch in autistic people. We asked participants about their lifetime experience of itch across three categories as follows: spontaneous, provoked, and medical itch. Our questions targeted the feeling of itchiness rather than the behavioral act of scratching an itch. Compared with a non-autistic comparison group, autistic people experienced more severe and long-lasting itch, with a greater negative impact on daily life. Importantly, there was no evidence that itch caused by dermatitis, an itchy skin condition more prevalent in autistic populations, contributed to their heightened experience of non-medical itch.
Autistic participants had a heightened experience of provoked itch. The neurobiology of mechanically induced itch (i.e., itch induced by a physical skin stimulus) is not fully understood but the role of c-fibers is increasingly recognized.45,46 There is evidence for mechanical itch-specific c-fiber pathways as well as evidence for c-fiber pathways shared with other modalities, including pain and affective touch.14,47 In our study, itch caused by clothing and material was more common and severe in those with an autism diagnosis, as well as itch caused by another’s touch or typically painful stimuli. This raises the possibility that itch-specific and nonspecific pathways are sensitized in autism and may implicate a central location causing these differences.48,49 However, the limit to biological inferences an explorative questionnaire can make is quickly reached, and future efforts exploring central nervous system structures, including the spinal cord (accessible using spinal cord fMRI), will be required to draw conclusions.
Similar to provoked itch, spontaneous itch also affected significantly more AUT-D participants at significantly greater severity, duration, and impact compared with the non-autistic group. This finding is compatible with hypotheses proposing differences in attenuating interoceptive information in autism 20 but needs further work to confirm if this is the case.
As predicted, itch caused by medical conditions was experienced across all participant groups as more severe than spontaneous and provoked itch. Comparing the groups, it was more severe for those with a clinical diagnosis of autism and also had a greater impact on daily life, with the exception of sleep. No differences for timing and duration were found. Although the total number of people endorsing the different types of medical itch (participant counts) was significantly different by group, post hoc pairwise tests were not significant. Itch caused by the subcategory dermatitis did affect significantly more AUT-D participants, in line with the literature and our hypothesis. 35 However, contrary to predictions,22,30 the severity of dermatitis itch did not influence severity scores of other coexistent nonmedical itch types. Furthermore, removing participants with a history of dermatitis did not affect significant group differences in itch severity for spontaneous or provoked itch, but did reduce the effect size for spontaneous itch group differences in participant counts. Finally, within our regression models, medical itch features were not associated with the degree of autistic traits reported by participants (AQ-10), nor their overall sensory differences (GSQ). As such, our prediction that autistic propensity to dermatitis would exacerbate spontaneous and provoked itch experience was not reflected in the data. Instead, we suggest that medical itch features are largely independent of autistic traits and that provoked and spontaneous itch are distinct forms of itch that are experienced differently in autistic people. The data thus highlight that both medical itch and other forms of itch are important components of the autistic experience. Our results suggest that more autistic people will present with medical itch, with greater severity and impact compared with non-autistic people, and that this will negatively contribute to existing disadvantages faced by autistic people in health care. 50 It is therefore essential that heightened, medically caused itch is researched alongside other itch types in autism, and that relevant findings are made accessible to patients and health care professionals to guide their management.
Impacts on daily life were similarly and significantly overrepresented in our autistic participants with a clinical diagnosis. For example, over 75% of AUT-D with provoked or spontaneous itch reported affected sleep, compared with less than 50% of non-autistic respondents. Differences found in both the impact on sleep and other daily activities provide support that itch experience is not simply better attended to by autistic people but a highly relevant component of their well-being. It is known that poor sleep directly impacts physical and mental health and one’s ability to work,51–54 suggesting that unpleasant itch may have both direct and indirect effects on quality of life.
Our study allowed respondents to self-identify as autistic (AUT-S), that is, they thought they were autistic but had not received a formal diagnosis. The scores for this group lay between the AUT-D and N-AUT groups for almost all measures, including AQ-10 and GSQ. We have limited information on the AUT-S participants and the reasons why they do not have (or have not sought) an autism diagnosis. It is likely many may be on a waiting list for diagnostic assessment, and some may have had a diagnostic assessment but not been diagnosed. Despite generally presenting with an intermediate itch presentation, a couple of subtle exceptions to this pattern were found. For spontaneous itch, participant counts and severity were the same (statistically) for those who self-identified they had autism compared with those who were diagnosed, while for provoked itch they were significantly lower. The presence of severe provoked itch is therefore associated with autism diagnosis, while severe spontaneous itch is a more general marker of elevated autistic traits.
Across all participants, autistic traits and sensory features positively correlated with severity, duration, and impact of spontaneous and provoked itch. This fits with our predictions made on the basis of higher rates of baseline scratching found as part of a study of itch contagion. 30 These significant correlations also persisted within groups. Together our studies present early corroborative objective evidence that itch is heightened in autistic populations. Helt et al.’s (2021) study also serves to highlight that scratching in autism, a phenomenon commonly encompassed under self-injury and “stimming” behaviors, may sometimes be itch-related behavior. Our study is unique in its probing of itch experience from self-report, rather than via a surrogate of scratching behavior. However, we did not explore the possible overlap between itching and repetitive motor behaviors. Also, some respondents may have been drawing on their experiences of itch-related stimming behaviors as much as of the underlying experience of itch sensation. The relationship between itch sensation, scratching, stimming, and self-injurious behavior will be an important avenue for future research.
Epidemiology of itch
Itch in the general population is a widespread phenomenon, but one with a poorly defined epidemiology.55–57 Our study was not epidemiological in its design, however, some approximated prevalence estimates can be made for the purpose of comparison. Within our non-autistic participants, 55% experienced itch within the last week and 39% experienced current chronic itch. These are both higher than most literature estimates at 8.5% and between 8% and 26%, respectively,57–61 but are comparable with a study where efforts were made to focus on a general patient population. 2 However, the previous investigations of itch within the last week excluded “yes, a little” as a response option, 58 and the studies that explored chronicity used longer durations (>6 weeks vs. >4 weeks in ours). Not only might these methodological differences account for disparities, but our counts may also be greater because of the nonclinical nature of our study: itch asked about as a phenomenon not a “problem” or “complaint” might encourage people to report itch otherwise considered trivial. Indeed, a very high percentage of our participants (95%), both autistic and non-autistic, reported itch at some point during their lives. Of note, a condition termed sensitive skin syndrome (SSS) has a worldwide prevalence of at least 38%, close to our chronic itch prevalence estimate for our non-autistic sample. 62 Its high prevalence may reflect the distress that unwanted skin sensations can cause. SSS is defined as “stinging, burning, pain, pruritus [itch] and tingling sensations … in response to stimuli that normally should not provoke such sensations…” (p.5) 63 and is a “diagnosis of exclusion,” only considered once other causes of itch have been ruled-out. 64 SSS presents a syndrome worthy of exploration within autism. Beyond SSS, prevalence studies of “incidental” itch of the type that we have measured (e.g., without medical cause and captured by our categories of provoked and spontaneous itch) are not readily found. However, the possible inflation of itch rates described above is unlikely to fully account for the negative impacts of itch that were endorsed by our participants.
Itch, autism, and interoception
Many hypothetical models of autism predict that heightened interoceptive experiences contribute to sensory differences. 19 Itch can be considered an interoceptive sensation as it provides the organism with information about the state of its own structures or tissues. Models propose that attention biased toward interoceptive information, occurring as a result of any of overamplification, reduced attenuation, or underprediction, might variously lead to greater reliance on the immediate interoceptive signal. This is sometimes at the expense of integrating other sensations, including socially relevant exteroceptive cues.19,20 Thus, what for non-autistic people might be a trivial itch sensation, for autistic people might become a highly salient event that interferes with social interactions.
Itch and anxiety
The itch literature shows a clear interplay between itch experience and anxiety. 39 Given that autistic people are more at risk of anxiety, and that our autistic participants reported heightened itch experience, it is interesting to consider whether anxiety might contribute part of the explanation. Within our Demographics section, we asked about diagnosed anxiety. As expected, AUT-D had higher proportions of diagnosed anxiety, and anxiety was significantly associated with the presence of all three categories of itch. Severity was also significantly higher for those with an anxiety diagnosis for spontaneous and provoked itch. Anxiety was not formally measured, however, and this highlights an important area that warrants follow-up.
Limitations
In interpreting our findings, it is important to recognize that our participants were a self-selected cohort; personal experiences with itch or autism may have attracted them to the study and “volunteer bias” may have inflated the self-report of itch experience. Also, as recruitment was uncontrolled, there was a disproportionate response by U.K. nationals compared with Australian, which raises the potential for sociocultural confounders. Those with an autism diagnosis had relatively late diagnoses, were early middle-aged, and predominantly female. Although age and sex did not differ significantly across groups and therefore does not invalidate our group comparisons, late-diagnosed autistic people are not necessarily representative of the wider spectrum of autism.65–68 Furthermore, completion of the survey necessitated a certain intellectual capacity, which also limited our ability to capture the heterogeneity of autism. The experience of itch for autistic children is also another important area for further study, which will additionally provide insights into the development of unusual itch experiences in autistic people.
Our survey was built on a validated clinical itch scale. 31 However, our study was explorative, and our survey was adapted and developed within this frame. The scope of our survey was necessarily constrained by considerations about completion time and participant fatigue (the primary motivation for using the abbreviated AQ). For example, we did not explore the contexts within which itch occurs. It might be that autistic people are more likely to experience itch, or experience itch as distressing, in particular environments. For example, we know that chronic itch and SSS are exacerbated by stress, negative emotions,63,69 and anxiety. 39 In addition, autistic children show increased scratching when viewing others scratching, which indicates sensitivity to the social context in the form of contagious itch. 30 There is the possibility that social context was a causative factor in spontaneous itch reported in our study. Further research into context could be important for helping autistic people better manage itch in the future. Another unexplored avenue that warrants follow-up is how ethnicity affects itch experience 70 and how this might intersect with autism.
We also focused on itch as a problem. However, it is known that some autistic people find components of their intense sensory experience pleasurable,71,72 and scratching an itch is often highly pleasurable. 73 Therefore, asking about itch-related pleasure will be important moving forward.
Finally, itch features and their relationships with autistic traits (AQ-10) and sensory features (GSQ) were explored via iterative regression modeling, a technique that can artificially inflate the predictive power of the final model. 44 The robustness of inferences that can be drawn from the AQ-10 data is also hampered by ceiling effects. It is important to note, however, that these models were designed to be exploratory and the findings require replication and extension in future work. Recent concerns regarding the psychometric properties of the AQ-10 need also to be taken into account when evaluating the model outcomes. 74
Implications
Our evidence suggesting heighted itch is a relevant and impactful feature of the autistic experience has implications for supporting the health and well-being of autistic people. For example, existing psychoeducational information on sensory differences in autism could be expanded to include discussion of itch. Clinically, the experience of itch in autism is not well documented or recognized. It may be important going forward to consider ways of disseminating information about the autistic experience of itch to clinical services, including both autism services and medical services that treat itch. Related to this, existing interventions for the management of forms of chronic itch may be amenable to adaptation for the problematic itch experienced by autistic people. For example, web-based tools for managing itch in eczema and psoriasis include information about coping techniques and itch triggers that could be applicable. 75 Indeed, working with the autistic community and clinicians to make existing therapies more autism-specific may be an endeavor that autistic people consider an important future step. A challenge of any research on a subjective experience that cannot be objectively measured is that personal perceptions may vary. We did not include a definition of itch, or examples of itch, due to concern that a description that did not mirror a person’s own definition may limit or bias their responses. It is important to note, therefore, that our data are underpinned by participants drawing on personal definitions and understandings of itch, and not on a singular definition. Currently, there has been no exploration of how autistic people describe itch and whether these descriptions can be considered similar or different to non-autistic people. These types of detailed insights and understanding would be best supported by qualitative methodology, such as interpretive phenomenological analysis. 76
Conclusion
Itch is a largely overlooked aspect of the autistic sensory experience. Our online survey has revealed that autistic adults report more itch, which is of both greater severity and longer duration, compared with non-autistic adults. Importantly, itch also had a greater impact on key elements of daily life, including leisure, housework, work, and sleep. The group differences were more pronounced for provoked itch and spontaneous itch compared with medical itch. However, and importantly, differences in medical itch did not appear to drive the experiences of other types of itch. Our group of participants who self-identified as autistic generally fell between the other two groups. These novel findings are a clear indication of a need to better understand the experience of itch for autistic people and to translate this research into support for autistic people who are being negatively impacted by itch.
Footnotes
Authorship Confirmation Statement
All the authors were involved in conceptualizing the study and developing its methodology. G.T. undertook the initial formal analysis, with subsequent input and advice from all the authors. The original draft was written by G.T. and has been extensively reviewed and edited by all the authors. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.