
Abstract
Background:
Neurodivergent higher education (HE) students (those with autism, attention-deficit/hyperactivity disorder [ADHD], specific learning disorders [SpLD], motor disorders, and communication disorders) report lower course completion rates than non-neurodivergent students and may require additional support. Existing research investigating neurodivergent HE student experiences has focused primarily on autistic or ADHD students. Little is known about students with other neurodevelopmental and/or multiple neurodivergent conditions. While some institutions are becoming more neurodiversity affirming, increasing our understanding about neurodivergent and non-neurodivergent students’ differences will help institutions improve supports.
Methods:
Using the bioecological framework, this study compared 131 neurodivergent and 73 non-neurodivergent students on person-disposition characteristics (autistic and ADHD traits, executive functioning [EF], self-efficacy, and sensory sensitivities [SS]), person-resource characteristics (mental health and well-being), and HE context factors (social support, enjoyment, disclosure, support use, institution type, study load, and campus mode). We compared five student groups, Autistic, Autistic and ADHD (AuDHD), ADHD, Neurodivergent-other (SpLD, motor and/or communication disorders) and Non-neurodivergent groups on these variables.
Results:
Neurodivergent students had higher autistic and ADHD traits, SS, anxiety and depression, and lower EF, self-efficacy, well-being, and enjoyment than non-neurodivergent students. Students in the AuDHD group reported the highest levels of anxiety, depression, autistic traits and SS, and the lowest EF and enjoyment. Apart from the AuDHD group, most eligible students did not disclose their condition(s) to their institution, nor use supports, indicating that increased efforts are required to normalize disclosure and help-seeking.
Conclusion:
This study increases our understanding of differences between neurodivergent and non-neurodivergent students and highlights the particularly poor mental health and well-being of students with AuDHD. Implementing neurodiversity-affirming, sensory-friendly, and flexible learning environments would benefit all students, not just those registered for support, and could lead to improved mental health, enjoyment, and thus retention of this growing population.
Community Brief
Why is this an important issue?
Neurodivergent students complete higher education at lower rates than non-neurodivergent students. Research into why this happens tends to focus on autistic students, with less attention on students with other neurodivergent conditions such as attention-deficit/hyperactivity disorder (ADHD), specific learning disorders (dyslexia, dysgraphia, and dyscalculia), and motor and communication disorders. While some institutions are making improvements in how they support neurodivergent students, a better understanding of how students with a range of neurotypes differ from each other may help institutions support more students to complete their education.
What was the purpose of the study?
We wanted to understand how neurodivergent student groups differed from each other and from non-neurodivergent students on person characteristics and features of higher education settings. We used a bioecological framework (interactions between people and environments) to structure our study.
What did the researchers do?
We surveyed 131 neurodivergent and 73 non-neurodivergent higher education students who were currently studying or had studied in Australia and New Zealand about their person characteristics, and higher education settings and experiences. Participants responded to an online, anonymous survey that took about 30 minutes to complete. Neurodivergent students fell into one of four groups—Autistic, Autistic and ADHD (AuDHD), ADHD, and Neurodivergent-other (i.e., students with neurodivergent conditions other than autism and ADHD). Almost one-third of these students had two or more neurodivergent conditions. We compared these four groups with each other and with the non-neurodivergent students.
What were the results of the study?
Compared with non-neurodivergent students, neurodivergent students had more autistic and ADHD traits, sensory sensitivities, and anxiety and depression symptoms. Neurodivergent students also had lower executive functioning, self-efficacy, and well-being and less education enjoyment than non-neurodivergent students. Students in the AuDHD group reported the highest levels of anxiety, depression, autistic traits, and sensory sensitivities, and the lowest executive functioning and enjoyment. Except for the AuDHD group, most students did not disclose their condition(s) to their institution, nor use any supports.
What do these findings add to what was already known?
This is the first study to compare higher education students across neurodevelopmental conditions with non-neurodivergent students. Our results show how neurodivergent students differ from each other and from non-neurodivergent students, and highlight the particularly poor mental health and well-being of students with AuDHD.
What are the potential weaknesses in the study?
We did not have many students with neurodivergent conditions other than autism or ADHD. This meant we could not conduct robust statistical comparisons across the neurodevelopmental conditions (as listed in the DSM-5) or on the number of co-occurring conditions students had. There were also more female than male students, and most of our sample attended university. Together these sample differences affect how well our findings may apply to other samples of neurodivergent students.
How will these findings help neurodivergent adults now or in the future?
Our results tell us that higher education institutions need to do more to support neurodivergent students. We need to increase efforts to normalize disclosure and help-seeking. We need to involve neurodivergent students in improving procedures and designing new supports to make sure higher education institutions meet their needs. Our findings can promote further research into improving higher education experiences and completion rates for neurodivergent students.
Introduction
Increasing numbers of students with disabilities are enrolling in higher education (HE), 1 but their success is less certain, particularly for those students with neurodevelopmental conditions. 1
Attending HE enables personal growth, social connections, skills acquisition, and increased employment opportunities, 2 yet completion rates are lower for HE students with autism spectrum disorder (autism),3,4 attention-deficit/hyperactivity disorder (ADHD), 5 specific learning disorder (SpLD), 6 and Tourette’s disorder, 7 compared with non-neurodivergent students. Higher education is an important life stage and usually coincides with the sensitive developmental period of early adulthood. 8 As identity formation matures and individuals experience changes in work, housing, and relationships, interactions between individual and environmental factors have increased potential to affect one’s trajectory.9,10 Applying a bioecological framework 11 to consider differences between HE students with and without neurodevelopmental conditions may enable institutions to better support neurodivergent students to course completion.
The bioecological framework of human development posits an individual develops through interactions with others (e.g., family, peers, educators) in their immediate environments (microsystems), which are in turn influenced by interactions outside their immediate contacts (mesosystems); broader systems including others’ experiences and institutional policies (exosystem); and finally, the legal, political, and cultural structures (macrosystem) in which they live. 11 Crucially, an individual’s personal characteristics can shape their interactions with others, known as proximal processes under the Process-Person-Context-Time (PPCT) model. 11 These person-characteristics are (1) demand (e.g., age, sex, gender identity, ethnicity), (2) disposition (e.g., attributes such as curiosity, distractibility, sensory sensitivities, neurodivergent conditions), and (3) resource characteristics (e.g., skills and abilities, mental health conditions). 12 Together, these person-characteristics can help or hinder social interactions and affect how others respond, thus influencing proximal processes. In turn, these processes may then impact the decisions made and the contexts in which one operates/exists so that the person is both a component of the model and an outcome of the processes they have experienced within the systems or contexts they inhabit. From a macrosystem perspective, while HE systems in Western countries such as the United Kingdom, the United States, Australia, and New Zealand differ in funding structures and legislative oversight, 13 HE globalization and massification trends mean equity, access, and persistence concerns are remarkably consistent across countries. 14 This article examines the person-characteristics and HE choices neurodivergent and non-neurodivergent students made as a result of proximal processes within the micro-, meso-, exo-, and macrosystems of HE in Australia and New Zealand.
While neurodivergence has several debated definitions, for the purposes of this study, we conceptualized neurodivergence as encompassing the neurodevelopmental disorders defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR), 15 including autism, ADHD, SpLD (dyslexia, dysgraphia, and dyscalculia), motor disorders (developmental coordination disorder [DCD]), stereotypic movement disorder and tic disorders (e.g., Tourette’s syndrome), and communication disorders (CD; language disorder, speech-sound disorder, childhood-onset fluency disorder, and social pragmatic communication disorder). While intellectual developmental disorders (IDD) are also neurodevelopmental conditions under DSM-5-TR, due to lower HE participation rates and specialized support services, 16 we considered students with IDD outside the scope of this study. Conservatively, 10%–15% of the general population may be neurodivergent, 17 and while research into autistic students’ experiences has grown, 18 students with other neurodivergent conditions have received less attention.
Person characteristics
Although neurodivergent conditions are defined by specific behavioral features, person-disposition characteristics such as sensory sensitivities (SS), executive functioning (EF), and self-efficacy occur across several conditions and may contribute to students’ HE experiences. SS are a core feature of autism and involve hyper- and/or hyporesponsiveness to sensory stimuli, which impacts daily life through sensory avoidance or sensory-seeking behaviors. 19 SS also occur in individuals with ADHD, 20 DCD, 21 SpLD, 22 anxiety, and depression 23 and can negatively affect academic progress in autistic HE students. 24 Similarly, EF skills such as planning, attention, and self-regulation are important for academic progress, with better EF predicting academic progress in first-year non-autistic 25 and autistic students, 26 and poorer EF associates with academic underachievement in adults with ADHD. 27 Finally, self-efficacy, which refers to one’s perceived ability to do things and be successful, 28 positively influenced academic performance in non-neurodivergent students 29 and predicted success for students with ADHD, dyslexia, and hearing and visual impairments. 30 Understanding how person-disposition characteristics may influence students’ HE experiences may provide insight into better supporting neurodivergent students.
Differences in mental health and well-being person-resource characteristics may also impact students’ HE experiences. Elevated anxiety, depression, and psychological distress occur among HE students,31,32 with increasing evidence that mental ill-health contributes to early course/degree termination. 33 Concerningly, neurodivergent students report higher rates of anxiety and depression than non-neurodivergent students,34–36 and 67% of students with disabilities versus 45% of students without disabilities reported mental health problems in a large survey of American college students. 37 Given the relationship between mental health and academic success in non-neurodivergent students, high rates of mental health difficulties may be contributing to reduced academic success for neurodivergent HE students.
Related to mental health is the person-resource characteristic of psychological well-being, which buffers against mental health difficulties and assists in coping with stress and engaging in productive work. 38 In HE students, well-being bolsters capacities for meeting the unique financial, independence and academic challenges of this life stage, 39 yet students report lower well-being than same-aged nonstudents.40,41 Notably, autistic 42 and ADHD 43 students and adults with DCD, 44 dyslexia, 45 and tic disorders 46 have reported poorer well-being than their non-neurodivergent peers. However, the relationship between well-being and HE experiences for neurodivergent students remains unknown, and increased understanding may lead to improved supports for these students.
Context
According to the Process-Person-Context-Time (PPCT) model, individuals’ interactions with others vary as a joint function of person-characteristics and environment, both immediate and remote. 11 In the HE context, reciprocal interactions with others (e.g., peers and educators) influence several relevant processes, which, in turn, affect students’ perceptions of social support and their choices regarding how, when, and where they study.
Social support from family, friends, and significant others provides emotional, informational, appraisal, and tangible aid to an individual 47 and eases the transition to HE. 48 However, lower levels of social support and difficulties making friends occur in autistic, 49 dyslexic, 50 and ADHD 51 students compared with non-neurodivergent peers. Given low levels of social support can exacerbate anxiety and depression52,53 and increase students’ likelihood of discontinuing their studies, 54 furthering understanding of social support differences between neurodivergent and non-neurodivergent students may inform future HE support provision.
The specific HE-context choices students make regarding study load, campus mode, and institution type can affect academic success and enjoyment of their overall HE experiences. For example, full-time students tend to perform better than part-time students, 55 which may be explained by the academic momentum theory, which posits students’ initial course load and progress create a strong trajectory toward degree completion. 56 While autistic students are more likely to study part-time,57,58 it is unclear if students with other neurodivergent conditions do so, or the impact part-time study may have on their experiences. Study mode may also influence HE success, with more online study associated with reduced degree completion.59,60 Given students with disability are more likely to study online61,62 and autistic students prefer it, 63 understanding neurodivergent students’ study mode preferences could help institutions tailor more targeted supports.
Institution type may be another contextual area of difference; American students with disability are more likely to attend 2-year than 4-year colleges, 64 and more Australian autistic students attend TAFE (Technical and Further Education) institutions than university. 57 This may be due to Australian TAFEs and New Zealand Institutes of Technology and Polytechnics (ITPs) focusing on vocational education and smaller class sizes, or their use as a pathway into university courses,65,66 similarly to American 2-year colleges. Less is known about institution choices for other neurodivergent students; this warrants further investigation given possible implications for support provision, as teaching and learning across university, college, and TAFE environments differ.
Perhaps the most important contextual factor for neurodivergent students is the provision of supports and reasonable accommodations, as support use predicts success, that is, grades and graduation, 30 and improves persistence 67 for students with disability. However, to access supports, students must first disclose their condition(s) to their institution, yet reluctance to do so is frequently reported in both non-neurodivergent students and students with disability. For example, a national survey of American college students found half were unwilling to disclose mental health conditions to their institution, 68 and a longitudinal study of 3000 American students with disability found that while 95% used supports in secondary school, only 35% disclosed to their HE institution, and then only 23% used the available supports. 64 On follow-up, students who had accessed supports were more likely to persist in their studies. 69 Among neurodivergent students, only 21%–30% of autistic students disclose to their institution,49,70 and students with ADHD were less likely to register for support (16%) than autistic students (23%). 71 Reasons for nondisclosure included fear of stigma, wanting to try on one’s own, or being unaware of available services.24,72,73 Understanding potential differences in disclosure reluctance is crucial for improving disclosure and subsequent support usage by neurodivergent students.
Finally, when the environment is right, students are more likely to enjoy their time in HE, engage in deeper learning, 74 and persist with their studies. 75 Enjoyment, that is, positive feelings toward an activity, is an important psychological construct across many areas of life, and involves individuals appraising their situation. 76 Distinct from passive experiences of momentary pleasure, enjoyment is experienced through active participation in activities that lead to personal growth and development. 77 Despite this, few studies have examined HE enjoyment in neurodivergent students. In studies with autistic HE students, enjoyment has been primarily addressed in qualitative analyses78–80 with only one quantitative/mixed-methods study found. 81 Overall, these studies found autistic students enjoy the act of learning, however, sensory overload and social anxiety can affect enjoyment. We found no studies comparing neurodivergent and non-neurodivergent students on HE enjoyment. Given that enjoyment may be more important for HE persistence than academic competence, 82 and the intrinsic connection to one’s context, further investigation into potential differences between neurodivergent and non-neurodivergent students is needed. While some institutions are becoming more neurodiversity affirming in their policies and practices, 83 there remains wide variability in implementation, potentially exacerbated by a lack of research to guide reform efforts.
In summary, the literature on neurodivergent HE students primarily focuses on students with autism or ADHD; little is known about other neurodivergent students (SpLD, communication and motor disorders) or those with multiple conditions. We aimed to compare Australian and New Zealand (Australasian) neurodivergent and non-neurodivergent HE students on person-characteristics and context factors within Bronfenbrenner’s bioecological framework (see Fig. 1), so that any differences may inform more tailored supports to increase neurodivergent students’ retention and HE completion. We hypothesized that compared with non-neurodivergent students, neurodivergent students would differ significantly on the following: (1) person-disposition characteristics with increased autistic traits, ADHD traits and SS, and lower EF and self-efficacy; (2) person-resource characteristics with increased anxiety and depression symptomatology and reduced mental well-being; and (3) HE context factors with lower enjoyment and social support, more part-time study, and more attending off-campus. We also expected that a minority of neurodivergent students would have disclosed to their institution or used HE supports.
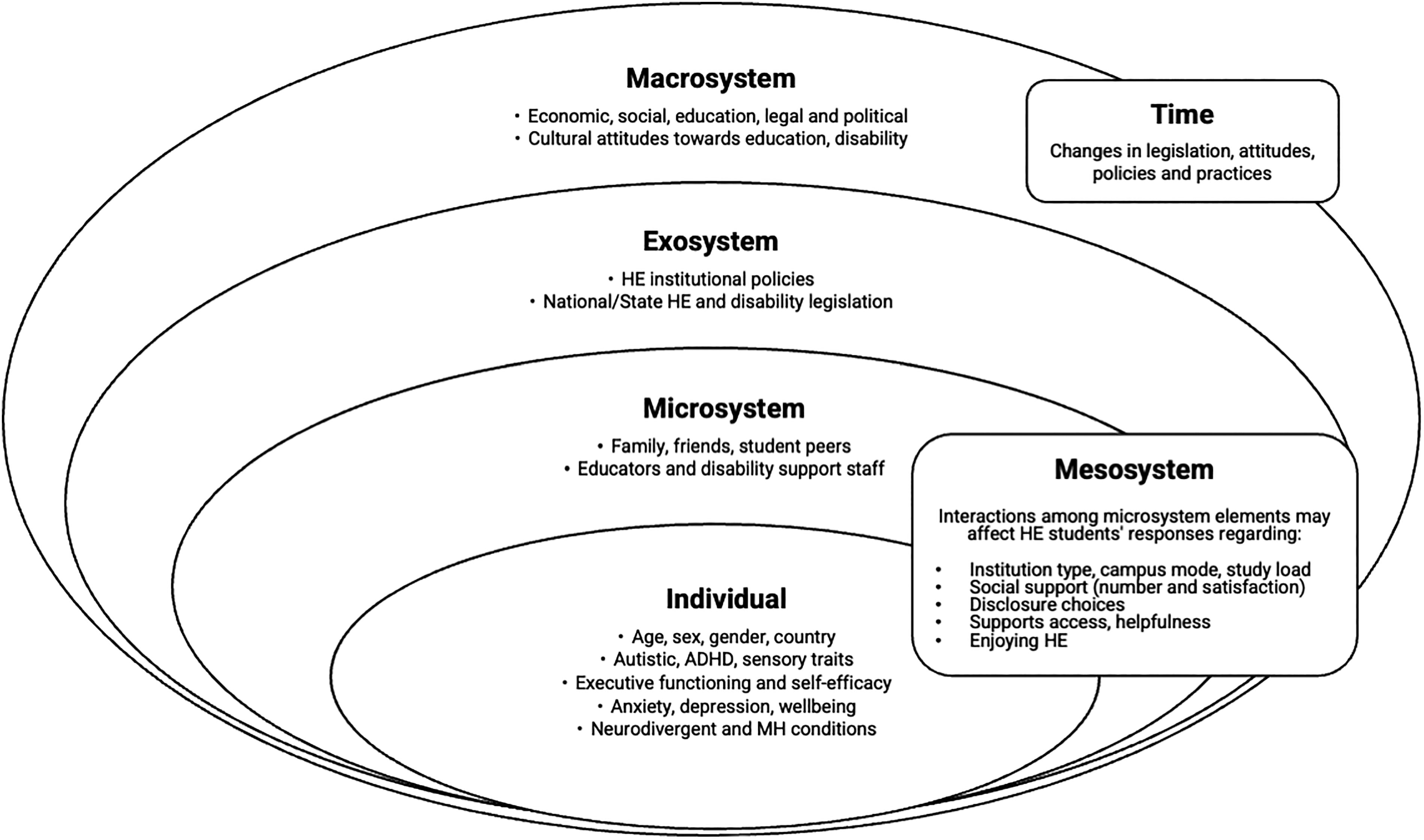
Individual (person) characteristics and higher education context variables within Bronfenbrenner’s bioecological framework.
Methods
Participants
Participants were those neurodivergent or non-neurodivergent individuals aged 18 years or older who attended HE (university, TAFE, ITP, or postsecondary college) in Australia or New Zealand between 2015 and 2021, and who completed an online survey. Participants self-reported their neurodivergent and mental health diagnoses. We excluded respondents if they were younger than 18 years, had not attended an Australian or New Zealand HE institution, or had ceased studying before 2015. Survey development followed a literature review, consultation with five neurodivergent student advisors, and review for ease of use, appropriateness, and comprehension. We shared social media posts and advertisements via Facebook, X (Twitter), LinkedIn, and asked our colleagues and affiliated institutions to do the same. We also asked Australian and New Zealand HE institutions and neurodiversity-related organizations to share our posts and advertisements with their students/members.
Where participants responded that they had a diagnosis of one or more neurodivergent conditions, they indicated which condition(s), when they were diagnosed (before primary school, during primary school, during secondary school, as an adult, or other), and by whom (psychologist, pediatrician, psychiatrist, occupational therapist, speech pathologist, GP, don’t know, or other). Participants could enter non-DSM-5 neurodevelopmental conditions by selecting “neurodivergent condition—other.” Participants could also proceed with the survey without entering “diagnosed by” information.
Participants completed the survey between April and September 2021, with a total of 204 participants classified as genuine respondents. Of these, 131 were neurodivergent (Mage = 31.34 years, SD = 9.86, 76% female) and 73 were non-neurodivergent (Mage = 33.16 years, SD = 11.24, 74% female). The majority of neurodivergent (62.6%) and non-neurodivergent (78.1%) participants were current students.
Measures
Demographics
Participants reported their age, sex at birth, current gender identity, country of birth, ancestry, home language, mental health conditions (current and ever), and neurodivergent diagnoses, including when diagnosed and by whom.
Person-disposition measures
Autism traits
The Social Responsiveness Scale for Adults 2nd edition (SRS-2) 84 comprises 65 items rated on a 4-point Likert-scale from 0 (not true) to 3 (almost always true). To improve sensitivity and specificity in general populations, we used total raw scores; scores >85 indicate an increased likelihood of autism. 84 Psychometric information for this and all other included measures can be found in Supplementary Data.
ADHD traits
The Adult ADHD Self-Report Scale Symptom Checklist (ASRS) 85 comprises 18 questions rated on a 5-point Likert-scale from 0 (never) to 4 (very often) and provides a total score used here. Total scores >30 indicate an increased likelihood of ADHD. 86
Executive functioning
The Executive Functioning Index (EFI) 87 comprises 27 items rated on a 5-point Likert-scale from 1 (not at all) to 5 (very much) and provides a total score, with higher scores indicating better EF.
Sensory sensitivities
The Glasgow Sensory Questionnaire (GSQ) 88 comprises 42 items rated on a 5-point Likert-scale from 0 (never) to 4 (always) and provides a total score, with higher scores indicating more SS.
Self-efficacy
The New Self-Efficacy Scale (NSES) 89 comprises eight items rated on a 5-point Likert-scale from 1 (strongly disagree) to 5 (strongly agree). The total score is averaged (range 1–5), with higher scores indicating higher levels of self-efficacy.
Person-resource measures
Anxiety symptoms
The Generalized Anxiety Disorder Scale (GAD-7) 90 comprises seven items rated on a 4-point Likert-scale from 0 (not at all) to 3 (nearly every day) and provides a total score, with scores >10 indicating clinical levels of anxiety symptoms.
Depressive symptoms
The Patient Health Questionnaire (PHQ-9) 91 comprises nine items rated on a 4-point Likert-scale from 0 (not at all) to 3 (nearly every day), which provides a total score, with scores >10 indicating clinical levels of depressive symptoms.
Mental well-being
The Warwick–Edinburgh Mental Well-Being Scale (WEMWBS) 92 comprises 14 items rated on a 5-point Likert-scale from 1 (none of the time) to 5 (all of the time). Higher total scores indicate higher well-being.
HE context factors
Descriptive details about participants’ HE experiences we collected included country of study (Australia or New Zealand), institution type, load, study mode, and current course status.
Social support
The Social Support Questionnaire Short Form (SSQ-6) 93 requires participants to list the number of people (0–9) they can rely on for help in six situations, then rate how satisfied they are with that support on a 6-point Likert scale from 1 (very dissatisfied) to 6 (very satisfied). We calculated average scores for the number (SSQ-6N; range 0–9) and satisfaction (SSQ-6S; range 1–6), with higher scores indicating greater support or satisfaction with that social support.
Enjoying HE
Students responded to the question “Are you enjoying your higher education experience overall?” with either strongly agree, agree, disagree, or strongly disagree. We asked participants currently in HE to reflect on their current experience and deferred and former students to reflect on their past experience.
Disclosure and support
Participants with a neurodivergent or mental health condition reported if they had disclosed their condition to their institution and accessed any HE supports. Those answering “yes” then indicated which supports they had used from the following lists: academic (recorded or transcribed lectures, note-taker, supplied lecture notes, time management or organizational skills training, other), assessment (alternatives to group projects, alternate examination room, reader for examinations, extended time for examinations or assignments, use of computer during written examinations, other), and nonacademic supports (counseling, disability support consultations, peer mentoring, peer support groups, transition programs, modified orientation, other). Students could provide free-text responses by selecting “other.”
Procedure
The La Trobe University Human Research Ethics Committee granted ethics approval (Approval number HEC21027). Advertisements linked to a REDCap 94 survey which included the participant information statement and informed consent. Participants volunteered and remained anonymous, with a median response time of 35 minutes (range 0:15–15:15 hours, as participants could pause and return to the survey browser at will). Mandatory questions and questionnaires included survey eligibility, HE enrollment, age, sex, current gender identity, neurodivergent conditions, the ASRS, GAD-7, PHQ-9, WEMWBS, and NSES. In case existing options did not capture participants’ experiences, free-text options were available for sex, gender identity, and neurodivergent and mental health conditions. On completion participants could elect to (1) enter a one-in-five chance to win an AUD $25 (Australian) or US$20 (New Zealand residents) Amazon gift card, (2) participate in a follow-up interview, and/or (3) receive a summary of results. If provided, contact details were stored separately and could not be linked to survey responses. The removal of spurious submissions (determined by survey completion <15 minutes, and nonsense or patterned responses) left 204 genuine responses for analysis.
Data analyses
An a priori power analysis for comparing two independent groups (i.e., neurodivergent vs. non-neurodivergent students) using t-tests indicated a minimum sample size of N = 128, with effect size d = 0.5, α = 0.05, and power = 0.8. For data analysis we used SPSS version 29. We imputed missing values for the SRS-2 according to scale scoring rules, that is, we used the item median response if fewer than seven items were missing for a participant (n = 25). We imputed case means for other questionnaires if 10% or fewer items were missing (ASRS n = 6; EFI n = 4; GSQ n = 13). We only included participants with valid (non-missing) data for each comparison and present sample sizes with each analysis.
Initial analyses comparing neurodivergent with non-neurodivergent students showed significant differences in most variables of interest (see Supplementary Table S1). To assess the validity of combining all neurodivergent students into one group, we conducted subgroup analyses to examine whether neurodivergent students differed from each other on person-disposition characteristics. Due to the small number of participants with some neurodivergent conditions, and the 30.5% of students with two or more conditions, we could not form single-condition groups. Thus, we placed participants into subgroups (hereafter called neurogroups) based on the most frequent neurodivergent diagnoses (autism, ADHD) and combinations (autism and ADHD—AuDHD) reported, with remaining neurodivergent students (i.e., those without an autism or ADHD diagnosis) placed in a Neurodivergent-other group (see Table 1). Due to the change from two- to five-group comparisons, we conducted post hoc power analyses, which were adequate (0.82–0.90, see Supplementary Data).
Neurodivergent Condition Subgroups (N = 131)
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; AuDHD, Autism and ADHD; CD, communication disorders; DCD, developmental coordination disorder; ND-other, neurodivergent conditions—other; SpLD, specific learning disorder; TD, tic disorders.
We collapsed categories for institution type (college and TAFE/ITP combined 2 ) and HE experiences (strongly agree and agree combined, strongly disagree and disagree combined) due to limited option endorsement. 95 To examine group differences across categorical variables, we used chi-square tests. For expected cell frequencies <5, we used Fisher–Freeman–Halton exact (for r × c) or Pearson’s exact (for 2 × 2) tests. We determined strengths of association using Cramer’s V values of 0.05 small, 0.15 medium, and 0.25 large for df = 4. 96
To examine group differences across continuous variables, we used the nonparametric (distribution-free) Kruskal–Wallis H test, due to normality violations and uneven group sizes. We analyzed significant group differences with the Dunn–Bonferroni post hoc test for multiple pairwise comparisons, with r value effect sizes classified as 0.1 small, 0.3 medium, and 0.5 large. 95
Results
Table 2 reports participants’ neurodivergent conditions, subtypes, and diagnostic information; the most common conditions were ADHD, and then autism. Three participants in the Neurodivergent-other group reported only having conditions not classified as DSM-5 neurodevelopmental disorders (neurological impairment, Irlen syndrome and Mal de Debarquement syndrome, and nonverbal learning disorder). As excluding these students from analyses did not alter the results, and they self-identified as neurodivergent, they remained in the analyses. Diagnosis occurred in adulthood for most participants with ADHD or Neurodivergent-other and about half of the autistic participants; diagnosis occurred in childhood for most participants with SpLD, communication or tic disorders. Nearly a third (30.5%) of participants reported two or more neurodivergent conditions (Supplementary Table S2). The majority of neurodivergent students reported that a psychiatrist (49.6%) or psychologist (42.7%) gave their diagnosis (Supplementary Table S3).
Neurodivergent Conditions, Subtype Specifiers, and When Diagnosed (N = 131)
Subtype totals may differ from the neurodivergent condition totals as some participants endorsed having more than one subtype. The total number of conditions exceeds the number of participants as 40 participants had more than one condition.
Three participants in the ND-other group reported only having conditions not classified as DSM-5 neurodevelopmental disorders (“neurological impairment,” “Irlen syndrome and Mal de Debarquement syndrome,” and “nonverbal learning disorder”). Excluding them from analyses did not alter results, thus, due to their self-identification as neurodivergent, they were retained in the analyses.
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Person characteristics
Table 3 reports participants’ person characteristics. For person-demand characteristics, most participants were female, born in Australia, and reported an Australian and/or a U.K. ancestry, with median age varying from 26 to 32 years across groups. There were significant differences between groups on all person-disposition characteristics. The Non-neurodivergent group (1) differed from the Autistic group on all five disposition characteristics: SRS-2 with a medium effect (r = 0.43), ASRS with a small effect (r = 0.22), EFI with a small effect (r = −0.29), GSQ with a medium effect (r = 0.42), and NSES with a small effect (r = −0.24), (2) had lower ASRS with a medium effect (r = 0.49) and higher EFI scores compared with the ADHD group with a small effect (r = −0.23), and (3) had lower SRS-2 with a large effect (r = 0.55), ASRS with a medium effect (r = 0.41), and GSQ with a medium effect (r = 0.43), and higher EFI scores compared with the AuDHD group with a small effect (r = −0.26). There were no differences between the Non-neurodivergent and Neurodivergent-other groups.
Person Characteristic Comparisons by NeuroGroup (N = 204)
Ancestry percentages can exceed 100% as participants could select multiple ancestries.
Significance values for post hoc comparisons used the Bonferroni correction for multiple tests. NA gender identity and ancestry comparisons were not conducted as they were not part of the research questions.
Fisher–Freeman–Halton exact test was used when >20% of cells had an expected count less than 5.
MH-other includes OCD, schizophrenia, bipolar disorder, PTSD, sensory processing disorder, eating disorders, epilepsy, conversion disorder, complex PTSD, borderline personality disorder, and addiction.
Post hoc standardized residuals lie outside ±1.9.
ASRS, Adult ADHD Self-Report Scale Symptom Checklist; EFI, Executive Functioning Index; GAD-7, Generalized Anxiety Disorder Scale; GSQ, Glasgow Sensory Questionnaire; NND, non-neurodivergent; NSES, New Self-Efficacy Scale; PHQ-9, Patient Health Questionnaire; SRS-2, Social Responsiveness Scale; WEMWBS, Warwick–Edinburgh Mental Well-being Scale.
There were also differences between neurodivergent subgroups. The ADHD group had lower SRS-2 scores than the AuDHD and Autistic groups with medium effects (r = 0.31 and 0.41, respectively), lower GSQ scores than the AuDHD and Autistic groups with small effects (r = 0.28 and 0.24 respectively), and higher ASRS scores than the Autistic group with a small effect (r = 0.21). The Neurodivergent-other group had lower SRS-2 scores than the Autistic and AuDHD groups with small effects (r = 0.20 and 0.27, respectively), and lower ASRS scores than the AuDHD and ADHD groups with small effects (r = 0.25 and 0.27, respectively).
For person-resource characteristics, there were significant group differences across the GAD-7, PHQ-9, and WEMWBS scores. The Non-neurodivergent group had lower GAD-7 scores than the AuDHD group with a small effect (r = 0.27), lower PHQ-9 scores than the ADHD and AuDHD groups with small effects (r = 0.22 and 0.29, respectively), and higher WEMWBS compared with AuDHD and Autistic groups with small effects (r = −0.23 for both).
All four neurodivergent groups endorsed ever experiencing a mental health condition significantly more frequently (91%–100%) than non-neurodivergent students (75%) with a large effect (V = 0.27). There were group differences for ever experiencing an anxiety, depressive, or no mental health condition, and currently experiencing anxiety or depressive conditions. The AuDHD group was more likely to have ever had anxiety than the other groups, with a medium effect (V = 0.22). The AuDHD group was more likely and the Neurodivergent-other group less likely to have ever had depression than the other groups with a large effect (V = 0.38). For mental health conditions experienced currently, anxiety was highest in the AuDHD group with a large effect (V = 0.25), and depression was higher in the AuDHD and ADHD groups with a large effect (V = 0.29). No other mental health condition group comparisons were significant.
HE context factors
There were significant group differences on the country studied in, institution type, HE enjoyment, and HE disclosure (Table 4). There were no group differences for current student status (p = 0.116) or social support satisfaction (Mdrange = 5.17—5.58, p = 0.480). While social support numbers were not significantly different across groups (p = 0.051), the Autistic group reported fewer supportive people than the ADHD group with a small effect (Mdrange = 1.67—3.50, r = −0.20). A higher proportion of Neurodivergent-other students (59%) studied in New Zealand compared with other groups (13–27%), with a large effect (V = 0.34), and a higher proportion of AuDHD students (26%) studied at TAFE/ITP/college compared with other groups (4–14%), with a medium effect (V = 0.23). Although enjoyment was high in all groups (78.3–95.9%), the proportion of non-neurodivergent students enjoying HE was significantly higher than neurodivergent students, with a medium effect (V = 0.21). For disclosure and use of HE supports, we compared neurodivergent students with non-neurodivergent students who also reported a mental health condition (n = 42); more AuDHD students and fewer non-neurodivergent students disclosed their condition to their institution, with a large effect (V = 0.41).
Higher Education Context Comparisons by NeuroGroup (N = 204)
Significance values for post hoc comparisons used the Bonferroni correction for multiple tests.
Fisher–Freeman–Halton exact test reported when >20% of cells have expected counts less than 5.
Disclosure or supports use could be due to a neurodivergent or mental health condition.
Blended mode is a mix of on-campus and online delivery.
Post hoc standardized residuals lie outside ±1.9. ND-other, neurodivergent-other.
HE, higher education; ITP, Institute of Technology and Polytechnics; SSQ-6N, Social Support Questionnaire Number; SSQ-6S, Social Support Questionnaire Satisfaction; TAFE, Technical and Further Education.
Discussion
This exploratory study aimed to better understand differences between Australasian neurodivergent and non-neurodivergent HE students on person (disposition and resource) characteristics and HE context factors within the bioecological framework. Students comprised one of four neurodivergent (Autistic, ADHD, AuDHD, Neurodivergent-other) groups and a Non-neurodivergent group based on self-reported diagnoses. As predicted, neurodivergent students’ person-disposition characteristics differed from non-neurodivergent students, with generally higher autistic traits, ADHD traits, and SS, and lower EF and self-efficacy than non-neurodivergent students. Person-resource characteristics (i.e., mental health and well-being outcomes) were also poorer for neurodivergent students, especially those with autism, ADHD, or AuDHD. HE context factors differed by group, with a higher proportion of non-neurodivergent students enjoying HE compared with neurodivergent students, and a higher proportion of AuDHD than non-neurodivergent students attending TAFE, disclosing their conditions to their institution, and using supports.
Person-disposition characteristics
In general, findings for the five person-disposition characteristics (autistic traits, ADHD traits, EF, SS, and self-efficacy) were similar to co-occurring traits reported across neurodevelopmental conditions in children and youth.97–99 Scores for autistic and ADHD traits were consistent with participants’ self-reported autism and/or ADHD diagnoses. Many group comparisons were statistically significant, particularly for the Autistic, ADHD, or AuDHD groups compared with non-neurodivergent students. We observed significant differences across EF, SS, and self-efficacy as well as the expected group differences for autistic and ADHD traits.
We found significantly lower EF in our neurodivergent (Autistic, AuDHD, and ADHD) compared with non-neurodivergent groups, consistent with previous research showing that autistic HE students, 100 high-autistic-trait individuals, 101 and adults and HE students with ADHD,27,102 have lower EF than their non-neurodivergent peers. While our group comparison effect sizes were small, the EFI score means for our Autistic, AuDHD, and ADHD groups were also 10–14 points lower than those reported in Dutch HE students (M = 99) 103 and high-autistic-trait American HE students (M = 101). 101 Unlike previous reports that adults with DCD, 104 adolescents with SpLD, 105 and children with CD 106 had lower EF, our Neurodivergent-other group had similar EF skills to the non-neurodivergent students. This may be due to the small sample size and mixed nature of our “Neurodivergent-other” group. Children with dual diagnoses of autism and ADHD have previously reported lower EF than those with a single diagnosis, 107 but our findings for adult students did not support this, with similar scores across the Autistic, ADHD, and combined AuDHD groups. Given the association between EF and academic procrastination in undergraduate students, institutions could implement strategies to improve EF and build students’ ability to achieve academic success. 108 For example, a mentoring program RCT for ADHD students found participants sustained increases in mental health, EF, and use of disability supports, 109 while EF interventions for children with ADHD 110 and HE students with disability 111 have led to improved grades. Our findings together with existing literature highlight the critical importance of supporting EF skills for neurodivergent HE students to improve mental health and academic outcomes.
SS were significantly higher for Autistic and AuDHD students compared with non-neurodivergent students (with medium effect), and for Autistic and AuDHD students compared with ADHD students (small effect), which supports the known association of SS with autism. 88 SS for neurodivergent-other students were also higher, but not significantly so, than non-neurodivergent students, which could suggest sensory differences across a range of neurodivergent conditions. However, given our small sample size, we need further investigation. Given most sensory literature compares autistic individuals with non-autistic groups, 112 ADHD, 113 or those with other developmental conditions, 114 our findings across neurodivergent groups appear to be novel. SS are known to increase autistic students’ college adjustment difficulties 115 and negatively impact social and academic participation.116,117 Sensory-friendly space provision is highly desired by autistic students 118 and students with disability, 119 and sensory-architectural principles have been incorporated into autism-friendly university design. 120 Neurodiversity-focused resources can also assist staff to deliver more sensory-friendly lectures, classes, and events within existing physical spaces. 121 Our data expand existing knowledge, emphasizing the importance of considering SS for all neurodivergent students. Adjustments that help HE students manage sensory overload or avoid it (e.g., reducing noise, overcrowding, and harsh overhead lighting) are likely to benefit many students, autistic or otherwise.
Other than Autistic compared with non-neurodivergent students, the groups did not differ on self-efficacy. This contrasts with previous research showing HE students with ADHD and/or SpLD have lower self-efficacy compared with students without disabilities, 122 but supports research finding lower self-efficacy in autistic compared with non-autistic students. 123 Given self-efficacy in HE students can be improved 124 and is often lower in HE students than employed adults, 125 self-efficacy may be a worthwhile target for future supports for neurodivergent (particularly autistic) students.
In conclusion, examining person-disposition factors across several neurodivergent groups makes it clear that adjustments to HE supports are required for a wide array of students, not just those with autism or ADHD.
Person-resource characteristics
Our findings of poorer mental health and well-being among neurodivergent students, with the AuDHD, Autistic, and ADHD groups meeting clinical cutoffs for anxiety and/or depression, align with evidence of higher rates of anxiety and depression and poorer well-being among adults with autism,126,127 ADHD, 34 and HE students with disability, 37 compared with the general population. The elevated rates of anxiety and depression in students with AuDHD in particular, with median scores at clinically severe levels, and only one student not reporting an anxiety diagnosis, support the additive nature of autism and ADHD in conferring additional risk for mental ill-health. 128 Our results add to the scant literature examining HE students with both conditions. Given that mental ill-health is a key reason autistic students discontinue courses, 35 efforts to further understand mental health and well-being for all neurodivergent students, particularly those with less frequently studied and multiple neurodivergent conditions, and regardless of student disclosure status, may assist institutions to better support these students to course completion.
Person-demand characteristics
There were no significant group differences in person-demand characteristics of age or sex at birth; however, the sample was older than might be expected for HE students. This may be related to our sample including a mix of undergraduate, postgraduate, and higher degree by research students, as well as former students. Our sample also included a high proportion of female participants, which is consistent with previous research showing females are more likely to respond to survey requests than males. 129
HE context factors
Finally, we examined the Context from the PPCT model, being the environment in which students make HE choices, including social support, enjoyment, disclosure, support use, and structural factors. While we found social support was essentially similar across neurodivergent and non-neurodivergent students in the number of people providing supports, and satisfaction with those supports, Autistic students had statistically significantly fewer social supports than those with ADHD with a small effect. These low social support numbers are consistent with the literature for autistic adults 130 and lower than those reported for college students with disabilities. 131 However, only 54% of participants in our study provided complete data for the social support measure, possibly due to its onerous nature. The lack of difference in social support between neurodivergent and non-neurodivergent students contrasts with Alvarez-Fernandez et al. 132 who found adults with ADHD or autism had fewer social supports than non-neurodivergent peers. However, they used the Multidimensional Scale of Perceived Social Support, 133 which is shorter than the SSQ-6 and also captures support availability from family, friends, and significant others. Nevertheless, our findings indicate very few differences between neurodivergent and non-neurodivergent students on their social support network.
While HE enjoyment was generally high across all groups, more neurodivergent students reported not enjoying HE compared with non-neurodivergent students with a medium effect. Enjoyment has been identified as an emerging factor for persistence in the general student population.75,82 Historically, enjoyment in neurodivergent students has been considered a function of the neurodivergent condition,78,80 rather than as a psychosocial factor independent of one’s neurodivergence. Importantly, we identified that enjoyment was disproportionately lower for the AuDHD group. Although additional work is required to understand how adjustments to physical and social environments may improve enjoyment, it is clear that efforts to increase enjoyment for all HE students, while being mindful of neurotype, may lead to long-term benefits in mental health, well-being, and academic persistence.
To investigate disclosure differences, we compared neurodivergent students with non-neurodivergent students with a mental health condition. Over 82% of AuDHD students reported disclosing their condition to their institution compared with 19% of non-neurodivergent students, which was a large effect. Across the three other neurodivergent groups, less than half of students disclosed their condition, which is consistent with previous research showing that the majority of students with neurodivergent or mental health conditions do not disclose to their institution.71,134 Disclosure reluctance impedes students’ access to and use of supports, which impacts persistence in students with disability. 69 Most AuDHD students, about half of the other neurodivergent students, and about 40% of non-neurodivergent students with a mental health condition used supports, with no statistically significant group differences despite a medium effect. This is similar to reports for students with autism, 117 ADHD, 135 or ADHD with additional conditions. 136 Neurodivergent students have cited concerns about discrimination or being unaware of available supports as reasons for nondisclosure, 73 however, further work is required to understand why neurodivergent students, other than those with AuDHD, are not disclosing, thus missing access to supports they need to flourish in HE.
Across course structure or institution type, there were few statistically significant group differences. In contrast to previous research,61,62,137 our groups reported similar study-load and campus-mode choices, although a higher proportion of AuDHD students attended a TAFE, ITP, or college than the other groups with a medium effect, which was consistent with evidence that autistic students are more likely to attend TAFE than university; 57 AuDHD students may prefer the more hands-on, personalized, and flexible teaching environments in TAFE, ITP, and college settings. 138 It is important to note we collected these data during 2021, and thus, it is possible that COVID-19 restrictions and lockdowns influenced some HE students’ choices regarding study type. Nevertheless, our results indicate limited differences between the structure of HE studies for neurodivergent and non-neurodivergent students.
Implications
Collectively our findings describe a pattern of higher autistic traits, ADHD traits, SS, anxiety, and depression, and lower EF, self-efficacy, well-being, and enjoyment in neurodivergent students compared with non-neurodivergent students. Many of these differences were greatest in students with a dual diagnosis of autism and ADHD. AuDHD students reported a higher frequency of disclosure and support use, suggesting they have greater support requirements than other students.
Our results highlight the challenges experienced by neurodivergent HE students, particularly AuDHD students, making it timely to reconsider overall approaches to their support. A greater focus on compassionate, neurodiversity-affirming, and universal design for learning principles could lead to improved outcomes for all students. 139 Indeed, neurodivergent students and researchers have identified neurodiversity-awareness training, sensory spaces, peer groups, mentoring, and more flexible study loads as key supports for improving outcomes.83,118 While mentoring and skills development programs have been evaluated for autistic140,141 and ADHD students,142,143 additional work is required to determine if similar programs would be welcomed by all neurodivergent students. Moving away from deficit-focused, single-condition approaches and toward neurodiversity-paradigm-aligned supports could improve the uptake of supports, regardless of individual students’ diagnostic labels.
Limitations
While this exploratory study represents the first demonstration of differences between students with a range of neurodivergent diagnoses and non-neurodivergent HE students, there were some limitations. While we asked questions about formal diagnoses, the online anonymous nature of the survey precluded direct confirmation of diagnosis. While post hoc power analysis indicated adequate power, group sizes for conditions other than autism and ADHD, and for those with three or more conditions, were too small for robust comparisons based on individual neurodivergent conditions or number of conditions; larger samples may bring more nuanced group distinctions to light. In addition, we included both current and former students—it is possible that former students’ responses to the well-being and mental health measures (which captured participants’ current state) were influenced by circumstances unrelated to their HE experiences. Also, many in the ADHD or Autistic groups reported being diagnosed in adulthood, while those with other neurodivergent conditions were more frequently diagnosed in childhood. Our large proportion of female participants, reflective of much online research, 144 may explain the higher proportion of adult diagnoses. Those diagnosed in childhood may have received early supports that helped equip them for adulthood and HE. Data collection occurred during extended COVID lockdowns, which may impact the generalizability of study-load and campus-mode findings to nonpandemic times. Only 54% of participants completed the social support measure (SSQ-6) suggesting it was onerous, and the EF measure (EFI) had low reliability for the neurodivergent sample. Some of the measures we used are not validated in all the neurodevelopmental condition populations, and most of our sample reported attending university, which may reflect a recruitment bias. Future studies with larger samples may enable comparisons across individual neurodivergent conditions, and determine if results differ due to age of diagnosis, gender, and institution type. In this exploratory, descriptive, cross-sectional study, we sought to understand differences between neurodivergent and non-neurodivergent students across person-disposition characteristics, person-resource characteristics, and HE context factors. Future studies could use prospective longitudinal designs to further explore the interconnected nature of these concepts within Bronfenbrenner’s bioecological framework to deepen our understanding of student experiences and enhance outcomes.
Conclusion
Using the bioecological framework, this study increases our understanding of differences between neurodivergent and non-neurodivergent HE students that may affect their success. Person (disposition and resource) characteristics generally differed significantly across groups, with higher autistic traits, ADHD traits, SS, anxiety, and depression, and lower EF, self-efficacy, and well-being in neurodivergent compared with non-neurodivergent students. More non-neurodivergent students reported enjoying HE than neurodivergent students. Combinations of these person characteristics and context factors may be negatively impacting neurodivergent students’ success. More students co-diagnosed with autism and ADHD disclosed to their institution, and only around half of eligible students used existing HE supports. Given these findings, rather than prioritizing individualized processes after students verify support eligibility, institutions should consider systemic changes across micro-, meso-, and exosystem contexts to create more neurodiversity-affirming, sensory-friendly, and flexible learning environments that benefit all students, not just those who meet disclosure hurdles. We hope this study stimulates more reflexive investigation into the challenges experienced by neurodivergent students, regardless of diagnosis, and the transdiagnostic nature of person characteristics, processes, and contexts so that more nuanced, codesigned supports are provided to this growing population.
Footnotes
Acknowledgments
The authors gratefully acknowledge the cooperation and participation of all participants involved in this study. They thank their neurodivergent advisors and family members for their insight and valuable feedback.
Authorship Confirmation Statement
A neurodiverse team conceptualized and wrote this article. L.J.K. (neurodivergent), A.L.R., and L.P.L. contributed to the study design. L.J.K. developed the survey with five neurodivergent advisors. L.J.K. conducted the data analysis and wrote the article. A.L.R. and L.P.L. contributed to data analysis and provided critical feedback. All coauthors have reviewed and approved this article before submission. This article has been given solely to this journal and is not published, in press, or submitted elsewhere.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical considerations. The La Trobe University Human Ethics Committee (HEC21027) gave ethics approval.
Author Disclosure Statement
No competing financial interests exist. The authors declare no conflicts of interest.
Funding Information
The authors did not receive any funding for this study.
1
We prefer neurodiversity-affirming language and thus use “disorder” only when referencing diagnostic terms or existing publications.
2
In Australia, the term “college” usually refers to a high/secondary school (for students aged 13–18), a university-pathway institution, a TAFE institution, or a section of a university, for example, the ANU College at Australian National University. In New Zealand, the term “college” usually refers to high/secondary schools.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.