
Abstract
Background:
Due to a combination of thin-slice judgments, ableism, bias, and a focus on allistic (non-autistic) dispositional standards, autistic people may experience admission issues and retention problems in mental health professional fields at higher rates than allistic people.
Method:
To better understand their training and gatekeeping experiences, we interviewed 10 autistic mental health professionals and trainees from a variety of mental health professional programs (e.g., counseling psychology, clinical psychology, counseling, and social work). Utilizing reflexive thematic analysis, we generated three themes across our 11 semi-structured interview questions.
Results:
Our generated themes included ableism (systemic and interpersonal), personal toll (cognitive load and emotional toll), and protective factors (internal and external). Our understanding of our interrelated themes is informed by both double empathy theory and the minority stress model. Participants in our study also regularly discussed a need for better autistic mentorship.
Discussion:
We discuss recommendations for training program advocacy and neurodiversity-affirming practices. Based on our participant answers to strength-based and support-oriented questions, we offer suggestions for autistic mental health graduate trainees.
Community Brief
Why is this issue important?
Research shows that autistic people are judged very harshly on their personal characteristics by non-autistic people in recorded videos and in person. Non-autistic people judge autistic people as less intelligent, less likable, less trustworthy, less attractive, and more awkward than non-autistic peers. The mental health professional fields (counseling, social work, psychology, etc.) heavily factor personal characteristics in their judgment of students’ abilities to be successful in the field. Therefore, the practice of “gatekeeping”—where people are prevented from entering the mental health fields—may impact autistic trainees more than their non-autistic classmates.
What was the purpose of the study?
The purpose of the study was to explore the mental health professional training experiences of autistic students and professionals who had recently graduated, including their experiences with specific training activities (like getting feedback on recorded counseling sessions) and gatekeeping.
What did the researchers do?
We interviewed 10 autistic trainees and professionals about their mental health professional training experiences. We asked specific questions, leaving room for general conversation around these questions. Participants were paid $50 USD for an average interview of 49 minutes. After our interviews were completed, we transcribed the audio into a text form so that we could read and analyze the interviews. We analyzed the data by grouping participant experiences into general themes.
What were the results of the study?
We generated three total themes from our participant interviews, with each theme consisting of two subthemes. These included experiences of ableism from individuals and systems, the emotional and cognitive toll of living as an autistic person in graduate study, and personal and external factors that provided protection. Our participants also discussed how their autistic characteristics positively impacted their work with clients. Factors such as (a) deep, focused interest in clients and psychological science and (b) extreme empathy and c) pattern recognition appeared multiple times, which participants said helped them connect to clients—especially autistic clients.
What do these findings add to what was already known?
Some of our results match results from research focusing on disabled psychologists. Specifically, our participants also discussed barriers to accessing accommodations, expressed similar emotional struggles to the general disabled student community, and discussed a need for improved mentorship. Unique to our study, our participants discussed a desire for their mentors to be more knowledgeable about autism, in general. Our participants also discussed ways in which their autism provided them unique strengths in their fields, which had not yet been explored in the research.
What are the potential weaknesses in the study?
Our study sample was comprised of 10 individuals, which some may consider small. However, our sample was narrow, specific, and purposeful, which allowed for an informative interview and strengthens the conclusions we can draw from our data.
How will these findings help autistic adults now or in the future?
We hope that mental health professional training programs use the results of this study to increase the autistic-affirming practices. This change will both ease the emotional burden on autistic students and act to increase neurodiversity in the mental health fields, which directly benefits autistic clients and supervisees.
Background
The lens of Social Identity Theory—the humanistic attunement to organizing and defining ourselves via social groups—understands autism as a strength-based collective identity. 1 This lens is in contradistinction to a traditional, biomedical approach that treats autism as a disease to be cured which has contributed to public and professional stigma surrounding autism.2–7 Outcome research supports a social identity perspective, indicating that autistic individuals with a strong affiliation to their social identity exhibit improved self-esteem. 8 Functionally, autistic people’s perception of their social groups mirrors that of allistic (non-autistic) individuals, suggesting more commonalities than disparities. 9 Despite efforts by some researchers, many being autistic themselves, to counteract the systematic dehumanization, damaging language and attitudes persist within professional organizations.10,11
Autistic stigma, perception, and employment concerns
Researchers have recently argued that reciprocal constructs cannot solely rest as the responsibility of an individual, “disordered” party, as has been argued with autistic individuals. 12 Double empathy theory (DET; also double empathy problem) is a valuable lens through which to perceive allistic misperceptions of autistic people. The double empathy theory states that, from a value-neutral perspective, communication styles between autistic people and allistic people are simply different. 13 Despite this, because of the social perception of autistic people as “disordered” or having “deficits”—and the majority status of allistic people—the onus of repairing ruptured communication falls onto the minoritized autistic person. In line with this paradigm, researchers have found no significant differences in communication of information between autistic individuals when compared with communication between allistic individuals but rather that difficulties in communication emerge in mixed groups. 14
Perceptual biases go beyond differences in communication. Allistic individuals have been shown to have negative implicit biases against autistic individuals despite positive explicit attitudes. 15 These biases, in turn, impact evaluations of autistic individuals, with researchers finding that autistic individuals are rated more negatively than allistic individuals in video conditions.16–18 Researchers have found, in particular, that autistic individuals were rated as less attractive, more awkward, less intelligent, less likable, and less trustworthy than allistic individuals. 17 Beyond stigma, therapists appear to have limited training in autism compared with other diagnoses, which was the most common reported reason for not being open to treating autistic adults. 19 In turn, autistic individuals are negatively impacted by implicit and explicit bias by therapists and experience a lack of knowledge among clinicians as a barrier toward care.20,21
The stigma and misperceptions born from the double empathy problem have significant repercussions in the adult autistic community, particularly in the realm of employment. In a national U.S. workplace report of autistic individuals, researchers found that autistic unemployment post high school was 42%, a sixfold increase over the general disabled unemployment rate in the United States.22,23 Some of the largest contributors to these disparities are negative workplace attitudes and a lack of understanding regarding autistic people. 24 Current national U.S. statistics show that ∼69% of employed autistic adults work in jobs that are not public facing. 22 Due to anti-autistic stigma and stereotypes, autistic individuals desiring interpersonal, public-facing occupations, like those in the mental health fields, may face barriers toward admission and retention.
Admission and retention of autistic mental health professionals
A recent review of autistic employment identified concerns with job acquisition pre-employment and job retention post-employment. 25 In the mental health professions, the notion of preventing a trainee from entering the field is referred to as “gatekeeping.” 26 Gatekeeping, as a process, expands from admissions to an ongoing assessment of competencies throughout a program. 27 This process is an inherently hierarchical system by which clinicians are judged on, not only their skills but also their dispositions.26,27
While no previous research has explored the experiences of autistic students in mental health training programs, researchers have qualitatively explored the experiences of autistic medical students utilizing phenomenological methods. 28 These students described systemic concerns, including difficulty accessing adequate accommodations and a “fear of retribution,” including fear of dismissal from their programs (p. 5). Similarly, a recent high-profile example of alleged reactive gatekeeping in the counseling profession comes out of the Clinical Mental Health Counseling program of the Johns Hopkins University School of Education. 29 Four students in this program were dismissed in quick succession between 2020 and 2021, during the height of the COVID-19 pandemic. Three of these students were people of the global majority, and at least two of them have alleged disability discrimination as their reason for dismissal. In particular, gatekeeping concerns for one student included lack of “skills in communication and awareness” and lack of participation in small group settings—both criticisms that allegedly did not take into consideration the student’s formal university disability accommodations. 30 Today, there have been no repercussions for the dismissal of these students.
Research on the collegiate admission process has shown that nonacademic admission criteria (e.g., autobiographies and interviews) are more important to the screening process for students entering a college program than objective measures (e.g., GRE and GPA scores), which could systematically disadvantage individuals who could be seen as socially different (e.g., autistic people). 31 Traditional viewpoints in graduate programs recommend against disclosures of mental health diagnoses in graduate application materials, with more recent research indicating that perspectives on disclosure can differ by discipline.32,33 The decision to self-disclose one’s autistic identity appears to be complex for both autistic workers broadly and disabled psychologists.25,34,35 Alongside this complexity, researchers have found that participants with higher levels of stigma had stronger negative impressions of autistic individuals when an autism diagnosis was disclosed, while those with higher levels of autism knowledge rated first impressions more positively when the diagnosis was disclosed but not when the diagnosis was absent. 36 Therefore, despite some evidence pointing toward benefits in autistic identity disclosure to those with higher levels of autism knowledge (which one may presume could encompass those reviewing graduate applications to mental health professional training programs), it is unclear within the research how such disclosures may be viewed within graduate application committees. 36
As has been demonstrated in the literature, autistic people are much more likely to be negatively evaluated on their in vivo and recorded performances when compared with their allistic peers.15–18,36 Autistic college students face specific negative evaluations from their allistic classmates toward their academic ability. 37 Compounding this reality, misconceptions about autistic people and presentations remain common in college student populations. 38 Given that a core component of mental health professional training is peer review of video and audio data of recorded counseling sessions, it is not unlikely that some of this feedback may come from peers uneducated about the presentations of autistic people.39,40 As a result, autistic mental health professional trainees may feel increased pressure to camouflage their autistic traits overtly or covertly in order to avoid negative evaluation.
Camouflaging, or “masking,” is a conscious and unconscious process by which autistic individuals are forced to suppress their autistic traits to “fit in” to the larger allistic society. 41 Autistic rationales for masking include working effectively with classmates or colleagues, being taken seriously by others, demonstrating responsibility, getting a promotion, and performing well at university or college. 42 These findings are similar among autistic medical students who described external pressures to mask their autistic traits within their training environment, including to facilitate interactions with patients. 28 In a similar way, masking could be a purposeful way to demonstrate clinical responsibility and succeed in counseling coursework. However, masking has been shown to have detrimental effects on the self, including exhaustion, self-perception issues, disconnection, burnout, anxiety, and depression.42–44 These results highlight the need for increased understanding and awareness of autism in mental health professional training programs.
Current study and guiding theory
Recent scholarship has argued for the importance of the presence of disabled psychologists within the field to interrupt insider–outsider assumptions that disabled persons are only served by the field rather than the reality of such individuals existing and contributing within it. 45 This call to action includes a call to support disabled psychologists and trainees entering the field. The importance of this call is amplified by the experiences of disabled students in health service psychology programs who report a lack of utilization toward, or access of, accommodation resources within their programs, mirrored by only 21% of clinical supervisors regularly asking about supervisee accommodation needs.46,47 Qualitative literature in this area has also pointed toward the importance of, and desire for, mentorship from other disabled persons, indicating a need from disabled persons for representation within the field.34,46
The presence of autistic individuals within supervision and consultation settings is necessary to rectify communication gaps between groups as exemplified by DET, the guiding theory underpinning our reflexive process. 13 Autistic people tend to have a more realistic understanding of autism than allistics, and treating personal autistic accounts as valid and reliable sources of evidence on autistic experiences centers those individuals as experts on autistic lived experiences and thereby corrects for the narrative injustice that has befallen the autistic community. 48 Botha, an autistic researcher, underscores the impact of bias on individuals, writing, “To be involved in autism research when you are autistic, is to constantly experience the aggression of a field which has yet to come to terms with its own ableism” (p. 7). 49 In line with this sentiment, no study to date has yet explored the training experiences of autistic individuals as practitioners and trainees within the mental health fields.
In the present study, we aim to explore the training experiences of autistic trainees and professionals, including gatekeeping practices, in mental health professional education settings. Additionally, we hope to underscore the reality that autistic persons exist within the mental health professional fields, as well as highlight potential barriers for autistic individuals to remain within it—barriers largely perpetuated by neurotypical communication standards regarding what it means to be a counselor, how counselors must behave, and what the counseling profession must look like.
Methods
Participants and sample size
We recruited participants in the current study primarily via social media and snowball sampling. We recruited two of our participants via a follow-up interest survey following a separate research project from the same research team. We created advertisements (flyers, posters) for the current study and posted on Facebook, Twitter (X), and Instagram. At least one participant in the current study learned of the study through word-of-mouth recruitment. Inclusion criteria for participation included being (a) over age 18, (b) autistic (clinically diagnosed or self-identified), and (c) currently enrolled in (or recently graduated from) a mental health professional graduate training program. Operationally, we defined “recent graduate” as graduating within the last 5 years and “mental health professional graduate training program” to include the following programs: (master’s or doctoral programs in) counseling, marriage and family therapy, social work, psychology (counseling, clinical, school), psychiatry, or psychiatric nursing.
We recruited 10 autistic participants either currently enrolled in, or recent graduates of, a mental health professional training program. Braun and Clarke recommend against claims of data saturation in determining appropriate sample size. 50 Instead, they recommend a focus on concepts such as informational power—an emphasis on the richness of the data through a narrow study aim and targeted data collection. 51 While our semi-structured interview questions were diverse, their focus was narrow: understanding the interface between autistic characteristics/ways of being and mental health professional training.
The mean age of our participants was 31.2. Our sample was racially and ethnically diverse, with 50% of our participants identifying with a minoritized racial or ethnic identity (e.g., Cree, Jewish, Japanese, Taiwanese, etc.) and representing four countries: the United States, Canada, Norway, and England. Six participants were romantically partnered (e.g., married, long-term partnership). Seven of our participants self-identified as autistic, while three were clinically (professionally) diagnosed. Length of self-identification and clinical diagnosis ranged from 6 months to 20 years. Professionally, participants came from a variety of training programs, including counseling psychology (N = 1), clinical psychology (N = 3), social work master’s programs (N = 1), and counseling master’s programs (N = 4). Full participant demographics can be found in Table 1.
Demographic Breakdown
Alexis did not provide pronouns, so we have used the gender-neutral pronouns “they/them” for them throughout this article.
At the time of interview, Avery had recently withdrawn from her clinical-community psychology PhD due to a remediation plan that specified “deficits in interpersonal skills.” While not an active clinician, we found their experiences important enough to warrant inclusion.
Diagnosis type refers to either self-identification of an autistic identity (also called self-diagnosis) or clinical diagnosis provided through a formal, medical diagnostic process.
Procedure and data integrity
All participants in the current study completed two informed consent processes, approved by the institutional review board of the corresponding author’s institution. The first informed consent described to participants the purpose of the study, potential risks, and inclusion criteria. The second informed consent was for audio/video recording and informed participants about their rights to their recordings and data management procedures. Participants were informed, verbally and via consent paperwork, that they were free to withdraw from the study at any time. Participants were given the option to consent to audio and/or video recording—no participants opted into audio-only recording. Participants were interviewed and recorded remotely via Zoom or Google Meet. All participants were paid $50 USD for their participation. The average interview length was 49 minutes (range: 14–101 minutes). To protect participant privacy, we offered participants the option of using pseudonyms (both during the interview and in the article) and pseudo-pronouns. All participants chose a pseudonym to use in the article, and some chose to use pseudo-pronouns, as well.
We developed the initial semi-structured interview used in the current article via a collaborative and iterative process between the researchers, who developed, tested, and refined the nature of the material via mock and participant interviews. Internally, the initial semi-structured interview was referred to as the “beta” interview, to denote its unfinished nature. Our beta interview was additionally refined through a participant pilot program during the summer of 2023. Three co-authors of the current article (R.B., C.H.H., S.E.K.) engaged in piloting interviews with three autistic participants (who were monetarily compensated). Using the data and researcher experiences from these pilot interviews, we engaged in the iterative process of refining the beta interview. The pilot interview data allowed us to refine and reduce our lines of questioning to those that seemed to reoccur most frequently, thereby strengthening our information power. Our iterative refining process reduced our semi-structured interview from 3.5 pages to 1.5 pages while seeing a tandem increase in the number of questions from 6 to 13. There were two cultural insiders (including the corresponding author) involved at each step of the interview development process. The final semi-structured interview can be seen in Supplementary Appendix S1. Pilot data were excluded from final analyses.
We asked participants 13 questions during our interview processes, 11 of which were thematically analyzed for this article. The first 11 questions of our interview (Supplementary Appendix S1) centered training activities, mental health outcomes, strengths, and difficulties related to autistic identities—experiences oriented internally. Questions 12 and 13 were different in context, focused on external supports and advice to other autistic trainees. Specifically, the context of question 12 gave participants the freedom to imagine hypothetically helpful systems and personal supports if they didn’t have any to discuss (if they did, these data were analyzed for the current article). Question 12, coupled with question 13, provided rich discussion for how programs and systems could improve. In the editing of this article, based on reviewer feedback, we decided that the data derived from these two questions warranted its own document as neither the questions nor the data thematically fit with the direction of the current piece.
To protect the data from “scam” or “fraudulent” participants—people pretending to be autistic—we employed data integrity protection practices. 52 First, we had a level of identity verification for participation via email identification. That is, participants who were actively enrolled in a mental health professional education program were asked to confirm their identities by sending a verification email from their college or university email address (i.e., a .edu). Graduated professionals were asked to provide evidence of a professional online presence (e.g., a professional email address, a professional website). Second, we restricted data collection from specific sources, particularly Reddit, because the research team has experienced influxes of fraudulent participants from the site in the past. Third, we asked that participants turn their cameras on, at least momentarily, so that we could identify them physically (all participants consented to full-length video interviews). Fourth, we asked hyper-specific questions about autistic experiences and graduate training, to which answers would be difficult to falsify. Finally, participants were only able to accept compensation via a verified PayPal or Venmo account.
Analyses
We generated qualitative themes in the current study using the reflexive thematic analysis (RTA) process described by Braun and Clarke and Campbell et al.50,53 RTA is a widely recognized qualitative research method that offers a flexible, yet rigorous, framework for analyzing qualitative data. We specifically selected RTA as the analytical method in the current study because it assists in the interpretivist analysis of organic qualitative data. Steps in the iterative qualitative thematic analysis process included researcher familiarization with qualitative data, coding responses, generating themes from codes, reviewing themes, and reconstructing if needed, defining and naming themes, and report production.
The researchers for the current article began the RTA process by engaging in a personal, functional, and disciplinary reflexivity task. Personal reflexivity is defined as “how the researcher’s values shape their research and the knowledge produced,” functional reflexivity is “how the methods and other aspects of design shape the research and knowledge produced,” and disciplinary reflexivity is “how academic disciplines shape knowledge production” (pp. 60–61). 50 Particularly given the misinformation and bias surrounding autism and autistic people, the reflexivity step can be vital in understanding ways in which our qualitative data may be impacted by our sociopolitical assumptions. Researchers engaged in a formal reflexivity journal, the first of which was discussed across multiple seminar-style meetings. Continual reflexivity was discussed when appropriate (e.g., during coding, theming).
Following the beginning of the reflexive process, we began independently analyzing the data according to the steps described by Braun and Clarke. 50 Researchers familiarized themselves with the data, which involved deep readings of interview transcripts. Then, researchers divided the data into meaningful groups in the coding phase, driven by the semantic content of the data. Initial coding was done at the individual level, and then secondary coding was done as a group to analyze points of convergence and divergence. After secondary coding, our team was left with 44 condensed codes that we then recoded. After our tertiary code generation, our research team engaged in initial theme generation. As a group, our analyst team organized initial themes onto an Excel sheet and engaged in initial group diagramming of the relationship between themes generated across the analysts.
Results
Participant responses to 11 of our semi-structured interview questions were analyzed to generate 44 initial codes. After development, refinement, and naming, we generated three overarching themes, each comprised of two subthemes. We present our generated themes in this section with descriptions of their interrelation. Throughout this section, we refer to participants via their chosen pseudonym—complete participant demographics can be found in Table 1.
Theme 1: Ableism
In multiple questions across contextually diverse sections of our interview, participants brought up the concept of ableism, whether explicitly or implicitly. The theme of ableism was generated to capture participant experiences of microaggression, discrimination, and lack of staff support in their programs. Ableism, as a theme in our study, has two subcomponents: interpersonal ableism and systemic ableism.
Interpersonal ableism
Interpersonal ableism describes the everyday experiences of person-to-person discrimination, stigma, and microaggression that are commonly experienced by individuals with minoritized identities. This is what Emma said about her experiences with interpersonal ableism:
I feel like psychologists can be some of the worst when it comes to stigma against autistic people. Um, so I feel like I spend time correcting–either listening to, like, stupid microaggressions or very, like, uh, stupid stuff in class—that people have to say about autistic people. Or, if I have the emotional energy at that time, like correcting shit that people say.
Emma was not the only participant who voiced discomfort with interpersonal ableism, as evidenced by the following quote from Avery:
The social skills [were the most difficult aspect of the training program]. Um, the actual application part of it. I have all the theoretical knowledge of why interpersonal theory works, why Rogerian theory is supposed to work, but asking me to apply it in the moment at the time—and you’re filming me. Not only do you have that observer effect, um, but you’re asking me to apply it without teaching me and mentoring me and expect me to get it immediately. … I don’t think they knew how to help me, because everything they said just did not resonate.
In Avery’s case, the interpersonal ableism they experienced was through the expectation that they could immediately apply an interpersonal theory spontaneously, without much guidance, in a recorded environment. While a common activity in clinical training programs, this type of activity does not consider the cognitive differences experienced by some with autism including but not limited to difficulties with spontaneous communication, social comparison difficulties, impression management needs, and autistic camouflaging.
Systemic ableism
Emma and Avery’s descriptions of ableism are those that point to the weighty everyday interactions with which autistic individuals may be confronted, even in professional environments. In their cases, they describe that the ableism call is “coming from inside the house”—from psychologists themselves. Conversely, many of our participants discussed systemic ableism preventing them from success at various stages of their graduate process: from interview to training. Systemic ableism encompasses structures, barriers, policies, and regulations that negatively impacted our participants. This is what Olivia said about her experiences with the clinical psychology PhD application process:
The informal socialization of the interview process was probably the hardest for me. In part because, like, those situations—and that’s kind of what came up in my grad program—are always the hardest. The semi-, you know, like this isn’t technically formal, but you’re also still being kind of judged and, like, I’m like, I don’t know how to act and I don’t want to be too stiff, but I also don’t want to give too much away.
For Olivia, and many of our participants, there were conversations about allistic expectations and standards during the mental health professional graduate school interview process. Aside from application and interview components, which came up several times during our interviews, there was other systemic ableism noted: such as this statement from Alexis about seeking formal academic accommodations:
So the problem is, once you’ve had the initial meeting to ask for things, you then have to fill out all this paperwork, which is actually more difficult than filling out the paperwork to join the university in the first place. Um, and then you have to apply for funding. And then when you get the funding, you have to send it to the people, and then the people have to, um, set you up with somebody … So, so, so this year I’ve just not bothered … I’m just like. It’s too much hassle. Like I’m, you know, I’m not, I’m not doing it. So, um, so yeah, it’s really difficult.
Each of these quotes provides data for a cross-section of different types of ableism experienced by our autistic participants, at both the interpersonal and systemic levels. Across almost every question we asked during our interview, regardless of the context of the question, ableism emerged as a prominent and common experience for our participants within their training programs and universities.
Theme 2: Personal toll
The excessive stress that difficult experiences, such as consistent ableism, had on our participants also led to many discussions about the resulting personal toll. Personal Toll is a theme that comprises the psychological and physical impact of graduate school experiences on our participants as intersected with their autistic identities. Based on the responses from our participants, Personal toll is subdivided into cognitive load and emotional toll.
Cognitive load
Perhaps best illuminated by a quote, cognitive load is a subtheme that comprises the excessive higher-order cognitive hoops that our participants were expected to jump through to succeed in their programs. As reflected by our participants’ data, cognition can involve monitoring and regulation of behavior and effort, planning and executing social interactions, and understanding and predicting others’ thoughts and feelings. This is how Olivia described her experience of showing recorded mock therapy sessions in front of her peers:
And so for me, especially when we were doing the mock stuff, it was acting. So I’m like, it’s not me you are critiquing. It is [Olivia] the therapist who is acting…Because like for most of them, I was, especially if I knew I was being recorded, I was masking. So it wasn’t like a raw social interaction.
Sadie expressed a similar issue with the cognitive load of masking:
I was like, I literally feel like a performer the entire, like 75 minutes [of class]. Um, and so, I think that’s why also with like, the presentations, I needed the scripts. I needed to have run through it a few times and, like, really … I even had, like, pre-written jokes. So, I was like, there was no comfort of just like, being myself in a broader public space. Um, particularly since, like, what a horrible system. You depend on these folks to get your letters of rec and get certification to apply to internship. Whatever your preliminary exam assessors rate you on competencies to get you to even have access to applications.
While multiple participants discussed the cognitive realities of social camouflaging, some elaborated on other effortful cognitive experiences. For example, Nova discussed her difficult experiences with reflection assignments, a commonly used assessment tool in clinical training programs:
I wrote my first reflection paper in graduate school, and I was really proud of it. So proud of it. I worked really hard on it, and I got, like, an 80%. I was devastated … I had my partner, who was late-diagnosed with autism, read it … They read it and were like “this is very logical. There is no emotion. There is nothing in here that a neurotypical would read and be like ‘wow, they’re reflecting. You need to make kind of cliche statements.’” And when I started to do that, I got 100%. I would submit it, and I know I would get 100%, but it wasn’t a true artistic reflection … I had to sneak in certain phrases and certain wording to signal to a neurotypical audience that I had some sort of deep reflection process.
Alex, too, discussed components of graduate training that were made particularly cognitively challenging because of her autistic identity. In a conversation concerning upcoming oral comprehensive exams:
I just feel like having this group setting, where it’s going to be a new situation … I don’t even have time to adjust to it. I just have to, like, get there and figure it out and be able to, like, do things off the cuff. I won’t have that time to, like, observe and figure it out. I feel like I’ll just be really dysregulated.
Olivia and Sadie’s experiences reflect the intense cognitive effort of socially camouflaging their autistic traits to behave in a way that they believe is expected of them or more appealing to their allistic reviewers. They each speak to the experience of “performing” their role to meet requirements, even expressing discomfort or lack of safety in being themselves. Nova and Alex further emphasize this subtheme by discussing other academic situations in which they felt (or were shown) a requirement to bear a more extreme cognitive load to perform as expected.
Emotional toll
Firmly related to experiences that required increased cognitive efforts are those that demonstrated the emotional impacts of those cognitive demands. This quote from Alex about her training program experience highlights a significant emotional toll:
I guess I just felt very anxious and unsure of how people were, uh, seeing and perceiving me. And just feeling like I have no idea what to say is exhausting. Also, um, just being on, like, high alert the whole time. Exhausting, you know?
The exhaustion that Alex felt was similarly expressed by Jane, who said about her experiences with burnout during her graduate program:
[My meltdowns] tend to be characterized by bits of what I identify as, like, rage. Essentially out of nowhere. Um, and I tend to slam doors, slam cabinet doors, stomp around, and then, like, retreat to my bed and sob. Especially before I knew what a meltdown was. It was just, like, I would get just absolutely fucking furious out of nowhere, out of nowhere. And then, um, I really identified them as like, “oh, I’m having a temper tantrum” and, like, “I need to go and, like, lay down and cry.” And I would, like, cry and cry and cry and cry and cry and, like, overwhelm myself. And then just like, quite literally, curl up in a ball until, like, I physically had to get out of bed again.
While Alex and Jane shared experiences of severe emotional distress related to surviving as autistic trainees in their graduate programs, Avery shared an emotional toll taken by a specific training task: watching recorded psychotherapy videos.
[I experienced] shame. Feelings of incompetence. And then you’re trying to be strong, and you don’t want to show them that you’re overly emotional. You know, that you are actually an emotional being that can blow up at any moment. So, you have to kind of put on this mask of “oh yeah, I can handle this.” You know you can’t. You’re dying … Just like silently dying. A lot of shame, fear, anxiety.
Throughout our interviews, nearly all our participants shared at least one instance of significant emotional or cognitive turmoil, including narratives of: self-doubt, anxiety, anger, suicidal thoughts, sensory overwhelm, embarrassment, shame, and fear.
Theme 3: Protective factors
Protective factors is a theme comprising the numerous internal and external resources that our participants highlighted as helping them overcome or accommodate challenging components of their graduate training.
Internal resources
For example, Emma reported on her autistic pattern recognition as assisting her in multiple avenues of the training experience:
I think one [autistic trait or characteristic] that has been and is really helpful is pattern recognition. I think that’s both in terms of knowing what professors want in terms of papers and stuff like that, but also in terms of picking up stuff in my clients whenever I’m working with them.
For Emma, the experience of autistic pattern recognition allows her to more effectively navigate the everyday asks of her training and clinical experiences. Similarly, Stephen shared that his own emotional regulation abilities serve as protection for him:
I don’t think I relate to my emotions the same way as other people seem to based on, like, media representations and friends. It’s like, I have emotions, but they’re not as big or strong as a lot of people have and I’m also able to, like, suppress them for moments … Being able to use that to kind of, um, manage the stress that can come from grad school has been really useful.
Also indicative of an internal protective factor is topical monotropism, the ability to pointedly focus interest on a single (or a few) topics at any given time (a facet of the autistic neurotype). Monotropism was a strength professed by multiple participants and exemplified in this quote from Avery:
I like to go down the rabbit hole of, uh, of collecting as much information as I can in my brain. And then, the fact that I may be a know it all, but it’s coming from a place that is not meant to be like, “oh, I just want to show you.” I want to demonstrate that I know it. So, you know, I’m not trying to be that know it all. It’s just I’m showing you that I know it. I have the information. I am repeating to you back what I’ve learned.
And similarly, in this quote from Stephen:
Then the other thing is just like, focus. Special interests. That kind of constellation of common autistic traits or something that I have. They definitely help me out in grad school, which is a lot of research…I learn everything I can. So, like, that mindset has definitely been helpful. Some of the habits that I develop from just looking into special interests serve me well.
These internal protective factors (strengths) help to counterbalance the difficult emotional, cognitive, and expectancy effects experienced by our participants in their training programs.
External resources
Similarly, many of our participants discussed external protective factors as well. For example, Stephen shared about a supportive department chair:
The department chair has been super great so far. Again, during the admission process we talked about, um, when I withdrew from the program. I, you know, sent out emails to the professors that semester [I withdrew], to the chair, and a few other people. And, you know, general responses were, like, “we’re sorry to hear that.” “We understand if ever your situation changes, you’re always welcome back,” that sort of stuff. And then, um, the department chair, she was the one that helped [my decision] to come back. Um, I was working with her, and she was, um. You know, like, made time for me and helped me not just navigate getting enrolled for counseling classes, but like going through the like re-enrollment in the university process, that sort of stuff. So, um, like, she’s been solid throughout.
Like Stephen, many of our participants pointed to university personnel who were supportive and accommodating of them and their specific needs. Emma shared the following about a helpful supervisor:
In my first year, the supervisor I had whenever we were watching, um, those videos together, um, they were really good at offering me support and helping me think through like specific accommodations that would work for me in that moment because of my autism. Um, that was really, really helpful. It was very non-judgmental and just helped me think through things in my way.
Similarly, Nova shared the following experience with a supervisor they consider an “ally” to the autism community:
I think my supervisor just knows autism well, like she is not autistic herself. But she is very, very, very knowledgeable. She has autistic people close to her. And, there’s one thing to have autistic people close to you, but like, she works really, really, really hard to be in the know of everything that’s going on within the autism research field. She’s doing the work of a good ally, like genuinely doing the work of a good ally. Um, and I think that’s important. … She’s also very, very open to me understanding therapy and understanding the clinical space through my own autistic lens. And we’ve had very fruitful conversations about what it means to be an autistic therapist and what autism can look like in a therapy space.
Outside of protective individuals, some participants discussed environmental conditions that assisted in protection of their wellness. For example, in this quote from Sadie:
I did my practicum fully remote, and that was, like, a godsend in many ways because I was able to schedule my clients when I wanted to see them. I could be protective of my time that I was on shift, and they were really, really cool about matching me up with [clients in my preferred population].
Sadie spoke of a practicum placement that had policies in place that allowed her to flourish. Nova similarly spoke of an organization through which she has garnered much support (masked for anonymity):
I’ve been able to build connections with different partner organizations. So, I have a very beautiful connection with the [Autism Organization], and their subsidiary. I’m building a conference for them right now from the ground up. So, like, I’ve thrived outside of the [graduate program] cohort dynamics and I’ve been supported by everyone … I feel empowered and, um, supported and given a platform to start building stuff for myself.
The theme of protective factors sits in a contrast to the other themes in the current study, which are negatively valenced. However, based on the results of our data, all three themes sit within the realm of influence of one another (expressed graphically in Fig. 1). For example, the emotionally implosive meltdowns described by Jane (emotional toll), based on experiences of ableism and discrimination (systemic ableism), may be modulated by a supportive clinical supervisor (internal protective factor) and a strong sense of self-efficacy (internal protective factor). We want to be clear that these are hypothesized relationships and that the data of the current study do not give us sufficient evidence to draw causal, directional conclusions.
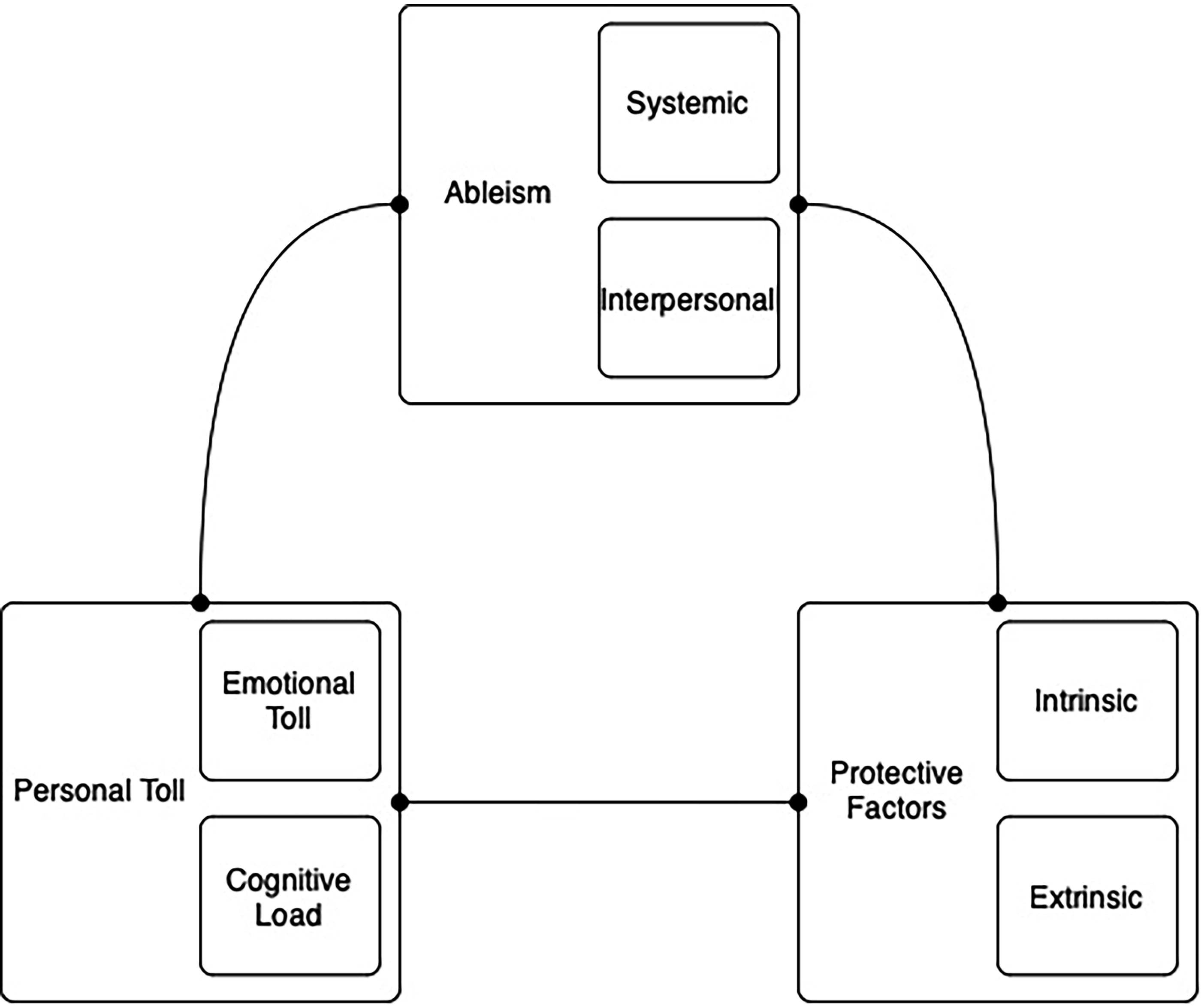
Model diagram of the hypothesized connection across generated themes.
Discussion
Using an RTA approach, we examined the nature of graduate mental health training across a diverse group of autistic mental health professional students and early career professionals to elucidate potential gatekeeping issues in various fields of mental health training. This is the first study to qualitatively explore the nature of autistic experiences in graduate mental health professional training programs. A thorough analysis of our in-depth interview data generated themes that revealed experiences of ableism on both an interpersonal and systemic level, internal cognitive load and emotional toll, and protective factors experienced by students related to their autistic identities.
Consistent with minority stress theory, a theory that centers the ways in which discrimination and prejudice impact mental wellness, our participants shared many instances in which they experienced broadly ableist microaggressions (and, in some cases, outright aggression) in reference to their autistic identity and ways of being.54,55 Some of the ableism our participants experienced was systemic—unsupportive programs, barriers to accommodations, gatekeeping—which mirrors research on disabled students in professional psychology and experiences of autistic medical students.34,56 Perhaps unique to our population are specific situations in which autistic students’ performance centers the ways in which their dispositions—not their abilities—are judged by their largely allistic professors and classmates (e.g., during face-to-face interviews, during recorded video review).
An inaptitude for programs to meet the needs of disabled students is not a new phenomenon, with a recent high-profile case of alleged disability-linked discrimination occurring in a counseling program. 29 Specifically, gatekeeping experiences of one student cited their dispositional concerns in their formal removal from the program. 30 Connected to this dispositional concern, employment research suggests that autistic people are evaluated much more negatively than allistic peers on in-person and recorded performance evaluations,15–18,36 while educational research suggests autistic college students are similarly evaluated more negatively by their classmates, 37 explicitly connected to DET issues 13 and general societal stigma that continues to permeate into college environments. 38
Camouflaging has been conceptualized to occur in response to one’s social environment, specifically in response to external bias or stigma towards autism.44,57 Likewise, camouflaging was common among our participants within their training environments. On one hand, participants discussed masking as a component of struggling to “fit into” social situations in their programs, and, on the other hand, participants discussed masking as a tool used to perform neurotypicality during a specific training exercise (counseling session video review). In both cases, the undergirding philosophy is a social pressure to suppress signature characteristics of their autistic ways of being in order to facilitate social interactions with allistic individuals, consistent with the DET. 13
Camouflaging can have detrimental effects on the physiological and psychological wellness of autistic people, leading to decreased mood, increased burnout, and increased prevalence of suicidality.16,43,44 We see some of these components of autistic wellness deterioration in our study, with our thematic subtheme of emotional toll, predominantly connected to negatively valenced intrapsychic experiences, including anxiety, overwhelm, shame, and burnout. While no previous study has quantitatively examined the mental health of autistic mental health professionals, researchers have identified that 77% of autistic physicians had considered suicide. 56 Future research is needed to uncover potential mental health concerns that may exist among this population.
Implications
The present study has implications for programmatic ability to provide adequate clinical training to autistic students. The therapeutic alliance has long been recognized as a central mechanism of change within therapy. 57 Among clients, the quality of the therapeutic alliance is positively and longitudinally associated with authenticity.58,59 Psychologists described authenticity within a qualitative phenomenological study as an alignment between internal thoughts, feelings, and beliefs with their external presentation and behaviors. 60 Authenticity was viewed as a reciprocal process between therapist and client, where authenticity evoked by either party encouraged synchronicity by the other. However, camouflaging is negatively associated with authenticity among autistic individuals, whereas authentic identity development among late diagnosed autistic women is associated with unmasking.61,62 In light of this, the pressure that participants within our study felt to mask their autistic traits, perhaps related in part to external pressures within their programs, deeply contrasts the goals of mental health professional education programs towards preparing their students to best meet the needs of their clients.44,63 This finding has implications for programs toward facilitating professional development for autistic students, as well as toward meeting the therapeutic needs of the clients they serve.
Perhaps in part despite these pressures, participants within this study expressed an ability to deeply connect with their clients, at times related to a heightened sense of empathic attunement. While experiences with empathy are varied among autistic individuals, some autistic individuals experience a heightened sense of empathy (or hyper-empathy), as was the case among some of our participants. 64 Alongside this, some autistic individuals experience a greater capacity for empathizing with the experiences of neurodivergent individuals as compared with neurotypical individuals, in alignment with the principles of DET toward similar communication styles among shared neurotypes.13,64 One of our participants noted, “I’m a great therapist for [autistic clients] when they’ve had really terrible therapists before,” indicating a potential toward autistic therapists facilitating corrective emotional experiences for past experiences of therapeutic trauma for autistic clients. 21 In this way, the present study adds to the small but growing body of literature recognizing the importance of inclusion of autistic professionals within health care settings in order to meet the needs of autistic clients and patients. 65
Beyond clinical training, the present study holds implications for the inclusion and treatment of autistic students within mental health training programs. Participants within the present study faced interpersonal and systemic barriers within their programs, alongside personal tolls navigating such concerns. These findings mirror the experiences of autistic medical students, who experience challenges within their programs such as difficulty with sensory processing concerns, lack of programmatic structure or support, and difficulty with unwritten social rules. 56
While the present study provides preliminary evidence toward the potential strengths autistic therapists may bring to the discipline, it also demonstrates a need for greater supports to be implemented. Through this interpretive lens, value for neurodiversity within mental health professional fields is not presupposed based upon the perceived service that individuals may bring to said settings. Instead, a true value of neurodiversity draws upon including people as they are and supporting their entry into areas in which there may be barriers on the basis of their shared humanity.
Strengths
The present study has many strengths. First and foremost, this is the first study to center the experiences of autistic individuals within the mental health professional fields, as well as the first study to explore autistic individuals as students within these settings. Through the RTA qualitative approach utilized, we uncovered nuanced depth toward the experiences of said students including strengths that autistic individuals may bring into therapeutic settings. This study is also novel from previous research on gatekeeping within these settings in that it centers the experiences of the gatekept rather than the experiences of gatekeepers.66,67 Finally, the participants in this study were from diverse racial and ethnic backgrounds, multiple countries, and a variety of mental health professional program settings, meaning that the themes identified may be more generalizable to the experiences of autistic students broadly.
Our strong internal validity is coupled with strong generalizability. Specifically, our research is transferably and naturalistically generalizable. 68 The transferable generalizability in the current study comes from its utility for graduate programs outside of mental health professional training programs. That is, we hope a variety of programs (and autistic students in these programs) can make use of the suggestions, recommendations, and implications herein. The naturalistic generalizability in this study stems from the resonance of the work with the primary investors—in this case, autistic graduate students. Autistic graduate students may resonate with the experiences of our participants and may directly utilize their (and our) suggestions.
Limitations
The primary limitation in the current piece may perhaps be one of population sample. However, following the qualitative methodological guidelines provided in the literature, 51 our sample data were narrow (in that our 11 questions were about a singular experience: mental health graduate study), our sample specificity was dense and purposeful, we understood our data through applied theories (double empathy theory; minority stress theory), our interview dialogue was strong (through an iterative semi-structured process), and our analysis strategy (RTA) was utilized cross-case to best understand our experiences of interest. In the context of a population that is so small, there are no adequate population estimates, and our developmental and methodological components lead to data that are of strong information power, an aspect of internal validity.
Connected to our sample demographics, 9/10 of our participants were identified as autistic as adults and 7/10 of our participants were self-identified (3/10 were clinically diagnosed). We center these demographics, not as though the autistic experiences of these individuals are limited in any way but to recognize that our sample is a thin slice of the greater autistic community. Our sample predominantly consisted of verbally fluent, college-educated, self-identified autistic adults who had experience with mental health training. This subsection of the autistic population is understudied, but we do want to be clear that their experiences may not generalize beyond autistics who share those demographics listed above.
Areas for future research
Based on the results of the current research, there are tangible, pragmatic changes to training, supervision, and organizational realities that could benefit trainees who share identities with our participants. First, as seen in our theme of ableism, autism education could assist in rectifying some of the interpersonal distress discussed by our participants. For example, our quote from Avery highlights assumptions of neurotypical performance stemming from educational experiences—an impact in the pedagogical process. Related, Emma shared experiences of microaggression in the classroom stemming from undereducated peers. Each of these instances of interpersonal ableism could be assuaged through autism acceptance or knowledge-based training, which has shown to reduce explicit autism bias. 69
Second, our participants discussed structural components of graduate training that did not align with their neurotype and autistic ways of being. These included interview formats (e.g., group interviews, informal social gatherings during interviews), specific clinical training tasks (e.g., reviewing psychotherapy recordings, reflection assignments, and in vivo supervision requests), and much more. Generally, participants pointed to structural barriers to their performance, often with concomitant cognitive and emotional impacts. To address this, clinical training programs—especially those that require internal reviews for accreditation (e.g., APA, CACREP, MPCAC, CSWE, COAMFTE)—could include an interrogation of neurodiversity-specific supports as a larger component of diversity, equity, inclusion, and justice policies. This call reflects both our participants’ experiences and current research from other health care fields. 28
Future researchers may also want to further evaluate autistic differences as potential strengths and protections against external demands in clinical training. For example, one of our participants, Stephen, shared, “I don’t think I relate to my emotions the same way as other people … I have emotions, but they’re not as big or strong as a lot of people.” In context, Stephen shares this as a protective factor of his autistic identity. Differences in emotional connection and expression are not uncommon in autistic people, with alexithymia occurring in around 50% of autistic people. 70 Alexithymia includes differences in the identification and labeling of intrapsychic emotions and can include difficulty with describing emotions to others, distinguishing between the mind–body connection of emotional arousal and an externalizing thinking style. 71 While often framed as symptomologic and dysfunctional, there could be occupational instances in which lower emotional arousal and connection could be a protective factor against unpleasant, highly emotionally arousing situations (e.g., in mental health crises). Given that autistic individuals view strengths related to their autism as context-dependent—helpful in some circumstances and difficult to navigate in others—future research in this area may be warranted. 72
Conclusion
Among a sample of 10 autistic mental health professional trainees and early career clinicians, we explored their graduate training experiences as impacted by their autistic identities. Our RTA process generated three themes across 11 questions, most of which centered a specific component of the training and graduate school experience. Each of our themes consisted of two clarifying subthemes. Consistent with double empathy theory and minority stress theory, our results indicated that autistic mental health trainees may have unique needs that are not being met by their training programs and academic systems of support. In not meeting autistic mental health trainee needs, these students could be gatekept from the fields of mental health services at much higher rates than their allistic peers. We observed this reality in our own sample—one of our participants was recently excused from their clinical program due to “deficits in interpersonal skills.”
Findings from the current study show that these worrying trends remain strong in mental health professional training programs. Our participants reported being academically strong but struggled with being judged from allistic expectations, standards, and ways of being. The constant juxtaposition of our participants’ abilities to those of their allistic peers—which reduces unique autistic strengths—led each of our participants to discuss instances of emotional and psychological turmoil. For autistic students to thrive in mental health professional environments, we need to radically de-center allistic standards in continued interrogation of what it means to be a mental health professional, how mental health professionals must behave, and what the mental health professions must look like.
Footnotes
Acknowledgments
We would like to thank members of the CRIB Lab at Valparaiso University for their dedication to centering this important work, including: Alexis Peterson, Gabrielle Eicher, and Ellen Linder. We would also like to extend our gratitude to the participants who shared their lived experiences with us; nothing about us without us. Thank you for allowing us the privilege of hearing you.
Authorship Confirmation Statement
C.R.D.: Conceptualization, data curation, analysis—primary and secondary, investigation, methodology, project administration, resources, supervision, writing—original draft, review, and editing. A.J.S.: Conceptualization, writing—original draft, review, secondary analysis, and editing; C.H.H.: Conceptualization, methodology, validation, primary analysis, investigation, writing—original draft, and visualization; R.B.: Conceptualization, methodology, validation, primary analysis, investigation, and writing—original draft; S.E.K.: Conceptualization, methodology, validation, and investigation; B.S.-N.: Validation, primary analysis, and investigation. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This research received no specific grant from any funding agency. However, the corresponding author would like to thank Knox College and Valparaiso University, the institutions from where internal research funds for this project were obtained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.