
Abstract
Background:
Difficult birth experiences are known to have long-lasting implications for physical and mental health. Autistic people are more likely to experience obstetric complications. To date, Autistic people’s experiences of maternity care have been underexplored. We aimed to explore experiences of antenatal and birth care to identify needs and factors associated with birth trauma.
Methods:
We used social media and snowball sampling to recruit for our online survey. Participants were required to be: Autistic, aged >18 years, living in the United Kingdom, and to have experienced pregnancy. Analysis included descriptive statistics and reflexive thematic analysis.
Results:
We received 193 usable responses. Quantitative results showed that the majority (86.4%) of participants reported masking when receiving care. Participants reported that they were not listened to (51.7%), misunderstood (47.8%), and unsupported (43.8%) during their maternity care. Over a third (35.4%) did not understand the way things were explained to them, and nearly half (48.9%) reported not being given the option to decline physical examinations. Our qualitative analysis resulted in three overarching themes that are interrelated. First, “health professionals’ knowledge of Autism” highlighted that maternity staff did not understand Autistic communication and pain presentations. Second, “systemic issues impacting on providing Autism-friendly care” focused on time and the ward environment as barriers to accessible maternity care. Third, “impacts of inaccessible care on Autistic people” described the way in which these two themes came together, resulting in lack of consent, safety issues, breached trust, and unmet needs for Autistic people.
Conclusions:
There is an urgent need for improvements in the health care given to Autistic birthing people. Increased knowledge of Autism, particularly focused on communication and pain expressions, is essential. Continuity of care, longer appointment times, and improvements to the sensory environment would also benefit Autistic maternity service users.
Community Brief
Why is this an important issue?
Pregnancy is a big change for anybody. There have not been many studies of Autistic people’s pregnancy experiences. Completed research has mostly interviewed small numbers of people.
“Informed consent” means that you understand what will happen and you can say no. Some research says that Autistic people have not been asked to give “informed consent” to tests or treatment in maternity care. This is linked to birth trauma in research on all people who have given birth.
What was the purpose of the study?
We wanted to ask Autistic people about maternity care, including things from previous studies on birth trauma and research with Autistic people.
What did the researchers do?
We asked Autistic people who had been pregnant and lived in the United Kingdom to do our online survey.
What were the results of the study?
In total, 193 Autistic people answered our questions. When they used tick boxes to tell us about their maternity care, most said they:
“Masked” (acted like they were not Autistic to get better treatment) during appointments; Were not listened to by maternity staff; Were misunderstood by maternity staff; Felt unsupported during their maternity care.
Also, it was common for Autistic people to not give “informed consent.” One in three said they did not understand the way their midwife or doctor explained things to them. Also, nearly half were not told that they could say “no” to treatment.
When we asked Autistic people to write down what happened to them during their maternity treatment, most people told us they had bad care.
First, in “health professionals’ knowledge of Autism,” they told us that maternity staff were not good at communicating with, or understanding them, and did not understand how they showed pain.
Second, in “systemic issues impacting on providing Autism-friendly care,” Autistic people focused on things in the maternity care system that made it hard for them, including short appointment times and the ward environment.
Third, in “impacts of inaccessible care on Autistic people,” Autistic people described issues such as having treatment without consenting and having unmet needs.
What do these findings add to what was already known?
We found similar things to previous research. The new things we found were almost half of the Autistic people said that they did not give “informed consent” most of the time. Also, many felt that maternity staff did not listen to them, understand them, or support them.
What are the potential weaknesses in the study?
The Autistic people in this study were mostly highly educated, white, cisgendered, and speaking. We also did not ask if they had learning disabilities, so our results may not apply to all Autistic people. Some of the Autistic people had their babies a long time ago.
How will these findings help Autistic adults now or in the future?
These findings show barriers in maternity services to meeting the needs of Autistic people, which may increase their risk of birth trauma. This information could be used to help maternity services better meet the needs of Autistic people.
Background
Pregnancy is a major life event and a time of significant change, regardless of neurotype. 1 Disabled 2 and Autistica, 3 parents may face stigma and discrimination, although Autistic parents report significant love and joy from parenting, 4 and becoming a parent can positively result in parents’ own adoption of Autistic identities. 5 The importance of person-centered care in maternity is well established, 6 and difficult birth experiences are known to have long-lasting implications for physical and mental health. 7 However, health care systems may make it challenging to provide person-centered maternity care, 8 and midwives’ abuse of power during birth has been reported by student midwives. 9 In a general population, birth satisfaction is associated with high levels of control. 10 Conversely, birth trauma has been associated with difficult interactions with maternity staff11,12 and has been reported alongside feeling disrespected and objectified, uninformed or misinformed, and unsupported. 13 There is some evidence that Autistic people may be at a greater risk of posttraumatic stress disorder from traumatic events—in this case motor vehicle accidents—compared with non-Autistic peers. 14
In the past decade, a small body of mostly qualitative research has sought to understand Autistic maternity experiences. This research shows that Autistic people experience sensory challenges during pregnancy and when receiving antenatal care, negatively impacting on mental health, 15 which continue during birth. 16 These challenges include lighting, smells, being touched during care, and breastfeeding. 17 Furthermore, Autistic people report a lack of effective communication with maternity staff. This includes feeling like they have to “mask,” finding it hard to share concerns, 18 not feeling comfortable to share their diagnosis, 19 and staff who would not listen, 20 including to reports of pain. 17 The consequences of this ineffective communication include receiving treatment or giving birth without adequate analgesia, 19 appropriate explanation, 21 or informed consent.22,23 Moreover, Autistic birthing people are less likely to have received support from partners, family, and friends compared with non-Autistic people. 24 Simultaneously, Autistic people have noted that during birth, they felt a need for a high degree of control. 18 In this context, Autistic people may increase “stimming” b when they feel dysregulated, such as due to a lack of control, 18 and may find home births more desirable. 23 Furthermore, the sensory environment of the postnatal ward was more likely to be found overwhelming by Autistic parents compared with non-Autistic parents. 16 Unsurprisingly, a recent systematic review identified that Autistic people were dissatisfied with their maternity care. 25 As well as parent dissatisfaction, quantitative research shows that Autistic people have a higher likelihood of major obstetric complications, 26 induction and elective cesarean sections, 25 and prenatal 24 and postnatal depression. 21
To date, the majority of the research on Autistic parents’ maternity experiences comprises small qualitative studies. In light of the potential for significant and long-lasting negative impacts arising from traumatic maternity care, 7 we sought to undertake research with a larger sample of participants with our closed questions based around the knowledge gained from these smaller studies, as well as the literature on birth trauma.
Methods
Aim
To explore Autistic adults’ experiences of antenatal and birth care in the United Kingdom to identify needs and factors associated with birth trauma and influencing the provision of optimal care.
Community involvement
To inform our survey design, we undertook an online community consultation, using Facebook and Twitter with 27 Autistic people who had been pregnant. They emphasized the need for gender-neutral language, a neurodiversity-affirming perspective, and ensuring that participants were able to report on all aspects of the maternity journey. The majority (25) were involved relatively briefly and were not paid for their time. Two were involved at length and were paid for their time at a rate of £25 per hour. One of these, Williams, was involved in the funding application and was part of the research team. The research team involved two Autistic researchers (A.G. and K.W.); additionally, two Autistic doctoral researchers (Rebecca Ellis and Hayley Morgan) reviewed the survey for its suitability to Autistic audiences; they were paid for their time.
Participants and ethics
Participants were recruited via relevant Facebook groups and through the social media networks of the research team. Prior to completing the online survey, participants reviewed eligibility information and were advised that they needed to be Autistic (including self-identifying or undergoing diagnosis), aged over 18 years, resident of the United Kingdom, and have lived experience of pregnancy. Eligible participants then reviewed a detailed participant information sheet, which stated that they did not have to answer any questions they did not want to. They were signposted to contact A.G. if they had any questions or to relevant sources of pregnancy and Autism-related support if they were distressed. Informed consent was recorded via the Qualtrics platform. The research received ethical approval from the School of Health and Social Care, Swansea University. When the survey closed, 10 participants who provided their contact details were randomly selected to receive a £20 Amazon gift voucher.
Measures
The full survey instrument is available in Supplementary Data. The survey comprised four parts: demographics (see Table 1 and Supplementary Data, pp. 1–5), health care barriers, use of aids to communicate needs related to Autism with health care providers (reported separately), 27 and “maternity experiences.” The maternity part included sections on experiences of “pregnancy” (see Supplementary Data, pp. 14–18), “birth,” and associated health care (see Supplementary Data, pp. 20–26), which are covered in this article. Due to the depth of the data received, we separately reported on “pregnancy loss” 28 and “infant feeding.” 29 A mixture of open and closed questions was used. The seven open-text prompts related to pregnancy and birth focused on:
Participant Demographics
M, mean; SD, standard deviation.
Sharing diagnosis with health professionals.
Thoughts about antenatal care, including communication, pain, sensory issues, receiving information, and emotional impacts.
Birth experiences, including variation from birth plans, communication, pain, sensory issues, receiving information, and emotional impacts.
Recommendations to improve care.
All closed questions can be seen in Tables 2 and 3. The majority utilized a 5-point Likert scale with a sixth option of “prefer not to say,” with scales ranging from “always” to “never” and “strongly agree” to “strongly disagree.”
Changes to Sensory Experiences During Pregnancy and Impacts of Changes
NB, prefer not to say responses are excluded from the table.
Experiences of Maternity Appointments
Data analysis
The survey was open from February 10 to March 31, 2022. Participants who completed any questions related to pregnancy or birth in addition to demographics were included in the analysis. Quantitative data were analyzed within IBM SPSS (Version: 28.0.1.1) by C.G., overseen by A.B. Analysis included descriptive statistics, and chi-square and Kruskal–Wallis tests were undertaken to investigate differences between Autism diagnosis and demographics. Questions with open-text responses were subjected to a six-stage reflexive thematic analysis 30 led by A.G., using NVivo (version: R1). A.G. undertook familiarization and coding (stages 1 and 2) of the data alone. She then presented this to K.W. and A.B., who reviewed, discussed, and agreed on the analysis while combining codes into themes (stage 3), reviewing themes (stage 4), defining and naming themes (stage 5), and writing it up (stage 6). In practice, this meant sharing documents prior to the meeting, with documents containing summaries with some quantification used to show how prominent particular concepts were within the data. Meetings were sometimes as a three and sometimes A.G. and another researcher.
Researcher positionality
A.G. and K.W. are Autistic; C.G. and A.B. are not. All four authors are white, highly educated women with lived experience of receiving maternity care, although A.G. has not given birth. A.G. and A.B. are experienced maternity care researchers who have over 10 and 20 years of experience in the field, respectively. Our disciplinary backgrounds are sociology (A.G.), social policy (A.G. and K.W.), and psychology (C.G. and A.B.). Epistemologically, A.G., the study lead, subscribes to Critical Autism Studies 31 and Feminist Disability Studies, 32 both of which aim to work with communities and to use research to actively improve society. K.W. is a director of Autistic UK, an organisation led by Autistic people for Autistic people, and has significant policy and research knowledge related to Autistic health care.
Results
We report our results in relation to demographics, sensory experiences during pregnancy, and maternity care. Our reporting of maternity care includes the thematic analysis. Within the tables reporting closed text responses, we provide responses by diagnostic status as well as for the whole sample.
Demographics
There were 193 survey participants who had given birth, a mean of 2.07 times (range 1–7 births; see Table 1). At the time of data collection, the mean age of parents was 36.51 (range: 19–63), and the mean age of their children was 7.28 (years; range: 0.24–39.24). All participants identified as Autistic. Almost half (47.8%) had been diagnosed as Autistic; another quarter (25.4%) were undergoing diagnoses; “other responses” included self identifying as Autistic and health professionals, or knowledgeable family or friends advising they sought an Autism assessment. Most participants preferred to speak (85.1%), were cisgender (85.1%), of white ethnicity (91.0%), and were educated to undergraduate degree or above (58.1%). In response to the question: “Do you have any physical/mental health conditions or disabilities lasting or expected to last 12 months or more? Please include things other than being Autistic here,” three-quarters (74.6%) of participants reported that they were disabled in relation to a condition not related to being Autistic, with this having some (64.2%) or a high (20.9%) impact.
A series of chi-square and Kruskal–Wallis tests were conducted to investigate whether the Autism diagnostic status groups differed on each of the demographic variables (see Table 1). No significant effects were identified; all results were p > 0.5.
Sensory experiences during pregnancy
A high percentage of participants reported that during pregnancy they experienced increased sensory issues in relation to smell (79.2%), touch (62.6%), sound (48%), and light (33.5%) “always” or “most of the time” (see Table 2). Most participants reported that these increased sensory issues led to increased discomfort (75.3%), anxiety (76.2%), and distress (58.7%), as well as shutdowns (44.6%) and meltdowns (40.6%), at least half the time. In addition, 16 participants reported an “other” impact of increased sensory issues, including pain, insomnia, changes in appetite, depression, paranoia, migraines, increased stimming, executive functioning issues, tiredness, irrational anger/sadness, and dissociation.
Maternity care
Of 166 participants who answered the question, over half (58.4%) did not know that they themselves were Autistic during their maternity treatment (see Table 3). Of the remaining 69, only 23 participants (13.9%) reported that most or all antenatal staff knew that they were Autistic. Considering attending maternity appointments, 41.9% of respondents had somebody, such as a friend, partner, or doula, with them “most of the time” or “always.” For those who did not, 19.2% reported that COVID restrictions were the reason. Most participants (75.7%) generally wanted to have someone with them while attending all appointments. Almost one-fifth (19%) of participants reported somebody communicating on their behalf during appointments, always or most of the time. The vast majority of participants (86.4%) reported “masking,” “most of the time,” or “always” when receiving care. Only around a third of participants reported feeling understood and listened to during the appointment, “most of the time” or “always.” Sixty percent of participants reported that they were not asked to consent prior to physical examinations more than half of the time. Furthermore, over one-third of participants (35.4%) reported that things were “never,” or only “sometimes,” explained in a way they could understand.
Thematic analysis
In total, 144 (74.6%) participants provided a response to at least one of the open-text questions, and 143 of these provided data that were sufficient to be coded as part of our thematic analysis. We developed three overarching themes from our reflexive thematic analysis. They are inter-related, as shown in our thematic map (Fig. 1). The themes are health professionals’ knowledge of Autism, systemic issues impacting on providing Autism-friendly care, and impacts of inaccessible maternity care on Autistic people.
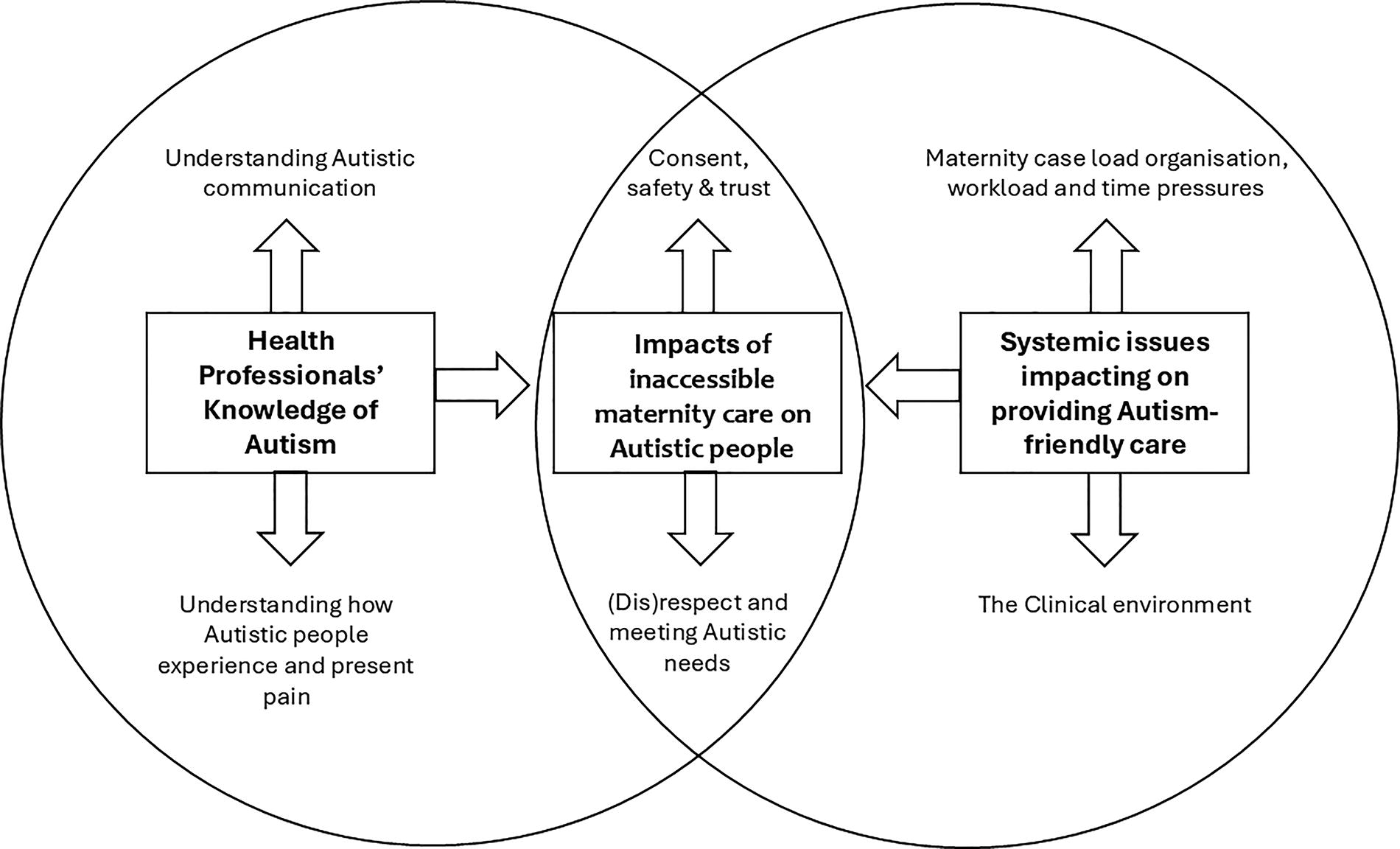
Thematic map.
We use direct quotations in the reporting of our findings and use demographic descriptors (see Table 1) to situate longer quotations. Where content is added to quotations to aid understanding, we use square brackets. Minor typographical errors remain where we feel that they do not disrupt readability.
Overarching theme: Health professionals’ knowledge of Autism
This theme focuses on health professionals’ knowledge of Autism as evidenced by their reported interactions with participants. Overall, participants felt that maternity staff did not understand Autism or their needs as an Autistic person: “They had zero understanding.” Some participants tried to educate staff about neurodivergence: “I often had to explain autism to [health care professionals],” although it was not always well received. Participants’ reports were able to be split into two subthemes: understanding Autistic communication and understanding how Autistic people experience and express pain. The overwhelming majority of responses were negative.
Subtheme: Understanding Autistic communication
Communication issues were commonly reported by participants throughout the data. The most common experience was not being listened to. Some participants articulated feelings of Autistic communication not being understood by staff: “Communication was difficult—it was as if I didn’t express things in the correct/expected way.” For many participants, this led to feelings of being ignored or disbelieved:
I was generally ignored and one point told I was lying and needed to stop making it up, [but] they had forgotten to put a catheter in and my bladder was about to explode… (Diagnosed primarily speaking white woman, aged 38, with an undergraduate degree)
Moreover, some participants noted that they were unable to communicate their needs during birth:
During the birth of my daughter, I completely shut down, I could not speak or open my eyes. … I just spent a long time waiting for permission to push as I thought that [was] what I had to do. … Once they confirmed that I could. … She was out I wish they had been clearer on that sooner. (Diagnosed white non-binary person, aged 47, with an undergraduate degree)
Some of these participants noted that their partner communicated vocally on their behalf, often reinforcing what participants had already been saying: “Due to my sensory issues, my mum helped me get the support I needed, after being ignored and left for 36 hours, my mum spoke to a midwife…” However, participants reported that partner communication was sometimes rejected by health professionals.
Participants noted that the use of indirect or vague language in health professionals’ instructions or questions could be confusing. For example, one noted that when they were asked “how much do you drink?” they had incorrectly recorded her as a “heavy drinker [of alcohol]” because she thought she was being asked about her consumption of water and responded accordingly. The use of vague questions could also result in participants not sharing relevant information when they had a minor concern: “I would never volunteer information or bring up problems but I appreciated [being asked] specific questions.”
Furthermore, Autistic masking, including appearing to communicate in a “normal” way and not having co-occurring learning disabilities, led to a minority of participants noting that their needs as an Autistic person were not understood by staff. For others, frequent questions were either “humoured” or responded to negatively: “she hated it when I questioned her…” Many participants suggested that clearer, and preferably multimodal, information was required.
Subtheme: Understanding how Autistic people experience and express pain
Many participants said that their pain was misunderstood by staff. In many of these accounts, there was an implicit understanding that Autistic pain presentations are different to those of non-Autistic people, such as not showing their pain outwardly in neurotypical ways, including “[giving] birth without making a sound” and “I wasn’t crying or displaying pain normally even though it was extremely painful.”
However, most of the misunderstood participants reported that they had provided a clear verbal description of their pain or made a verbal request for pain relief. These refusals resulted in “conflict,” “frustration,” and inadequate pain relief:
In my first labour (before 4 cm [cervical dilation]) I told a midwife I was in pain and asked for paracetamol, which she denied and told me I had a low pain tolerance. This really affected me emotionally and I did not ask for pain relief again in the first birth. (Diagnosed primarily speaking white woman, aged 34, with a National Vocational Qualification)
Inadequate pain relief was described by many and appeared to arise from health professionals not believing the birthing people were in pain, trivializing pain and actively refusing requests for medication. In a small number of cases, participants reported that painful examinations were not paused or stopped when they reported extreme pain: “I screamed the place down and was told to stop fussing.” Alongside this, further examples included: “[being] told off by a doctor during labour for screaming in pain,” “a sonographer got annoyed and said I was weird [when a pain response happened during an ultrasound],” and “pain relief [was] taken away when needed” during a postnatal examination for perineal or vaginal tears.
Although it is unusual to provide a number of participants in the reporting of reflexive thematic analysis, we feel that it is valuable to note that for 10 participants in the second stage of labor, which is when the cervix is fully dilated and they are ready to begin to push and deliver their baby, midwives did not believe that they could be close to giving birth and accordingly missed opportunities to provide care and pain relief:
My midwives … turned me away from the hospital because they said I couldn’t be in labour. I knew I was, but because I didn’t show any signs of being in pain, they didn’t even check me and sent me away. I went to the shop and rushed back to the hospital because I needed to push, they rolled their eyes … I gave birth 10 minutes later! (Undergoing diagnosis, primarily speaking white woman, aged 38, with General Certificate of Secondary Education)
I received no care as the midwife did not believe that I was in Labour because I was too quiet and not screaming in pain. I gave birth by myself in a hospital toilet. (Diagnosed primarily speaking white woman, aged 36, with a doctorate)
Another of these participants noted that they “had to beg for someone to examine me”; upon examination, they were “swiftly taken to the delivery suite.” Some of these participants noted the importance of adequately training midwives to understand how Autistic people experience and express pain: “Midwives need to understand that we do not all experience pain in the same way so they do not call us liars and tell us to stop wasting their time because they know best.”
In addition, some participants noted that a 1–10 pain scale was not a useful instrument to describe their pain and may have contributed to staff misunderstandings. A minority noted that they themselves struggled to understand their own pain due to interoceptive differences, until it was very severe, or that they were unable to communicate their pain using words.
Overarching theme: Systemic issues impacting on providing Autism-friendly care
The second subtheme related to systemic issues that impacted on the way that health professionals were able to provide care to Autistic birthing parents. Participants described a system that felt poorly designed to meet their needs, including feelings of “pressure,” “stress,” “so many changes,” and being “rushed,” alongside a sensorily aggressive environment. Their experiences are split into two subthemes: maternity case load organization, workload, and time pressures, and the clinical environment.
Subtheme: Maternity case load organization, workload, and time pressures
A lack of time was identified as a barrier to providing high-quality care throughout the maternity journey. This started with there appearing to be limited relevance and opportunity to share that they were Autistic during their first appointment. Subsequent appointments could also feel rushed; one participant described their health professional multitasking during antenatal appointments: “it always felt like a tick box exercise I felt that I was unable to communicate my needs. Looking at computer screens not acknowledging [my] presence or hearing what was being said.” This shortage of time also meant that health professionals did not have time to investigate unusual experiences or symptoms:
My care was coercive, to meet the needs and expectations of the medical professionals and sometimes abusive—[they said] that I was doing things wrong and hurting myself—eg early stage pregnancy severe pelvic pain was due to gentle pregnancy yoga and osteopathy, rather than due to undiagnosed EDS [Ehlers Danlos Syndrome]. (Diagnosed, prefers to communicate in writing, white woman, aged 48, with a Master’s degree)
Longer antenatal appointment times were recommended by many, with some recommending it should be universally available: “ultimately if staff had the time to care for people and to listen and take individual needs and preferences into account, it would suit everyone, not just autistic individuals.”
Seeing the same health professional each time (continuity of care) did not appear to be widely available. The small number who received it always reported their experiences positively:
I was under the perinatal mental health team at my hospital for my second and third births. This made a real difference and although I know autism isn’t a mental health condition, these midwives were adept at empathic care and ensuring continuity of care. Both times they helped advocate for my needs and it made a real difference. (Diagnosed primarily speaking white woman, aged 34, with an undergraduate degree)
Conversely, issues arising from lack of continuity of care were described by many, including the impact on person-centered care: “Didn’t get to build rapport with anyone and meant I was constantly having to explain things over and over again. Was very frustrating.” It also resulted in inconsistent information. At the worst, this led to hostile discussions with health professionals:
As for miscommunications, I was given a leaflet on sweeps [of the cervix to induce labour] in the lead up to giving birth, saying this could be done and was optional. The midwives confirmed this and said my consultant was very good at them. Then when I mentioned it to a different consultant he said this was nonsense and demanded to know where I had heard it as the hospital did not offer sweeps. He acted like I was going insane, when I had a leaflet at home which talked about them! He refused to believe me. Why would I lie? The information I was given towards the end of my pregnancy was inconsistent and when I repeated things I had been told (which I was certain of, as I made notes of everything and knew my stuff) I was gaslighted. (Diagnosed primarily speaking white woman, aged 35, with a Master’s degree)
Unsurprisingly, many participants explicitly recommended continuity of care to improve the accessibility of maternity care for autistic people.
Subtheme: The clinical environment
A small number of participants identified aspects of clinical environments that would be considered poor practice regardless of neurotype: “gas and air not plumbed in properly in 2003 hospital birth & ran out during home birth in 2011, felt in 2011 that this worsened my ME [Myalgic Encephalomyelitis, sometimes known as Chronic Fatigue Syndrome] experiencing unnecessary pain.”
More commonly, participants highlighted aspects of the clinical environment that particularly impacted Autistic people due to sensory processing differences. For some, this was a general feeling that the environment during birth was overwhelming: “Just the whole thing was a sensory nightmare.”
More specific comments reported: too noisy, bright lighting, too many people in the room during birth, lack of privacy having their movement restricted during birth due to fetal monitoring, and the unusual smells. Some participants described multiple sensory issues, while others focused on just one, for example:
I planned to be active and in control. Instead I had control systematically taken away from me and I became more pinned down with interventions in bright, hard rooms with no privacy. And staff openly arguing about my care. (Diagnosed primarily communicates in writing, white woman, aged 48, with a Master’s degree)
The result of these needs not being met could impact on labor: “I needed utter silence and low light to labour. Any sensory onslaught and it set off an adrenaline rush which slows things down.”
Also, in the postnatal period, being put on a ward with other new parents and babies could be very challenging from a sensory point of view: “[I] hated every second in a shared ward.” When these challenges were reported to staff, reactions were not always empathetic:
The hospital was a sensory hell. I desperately needed a private room but was put on a ward. The nurses were irritable and dismissive about my needs to be alone and quiet. I was “told off” for sleeping in the corridor on a chair but I was just trying to get a few minutes peace from the snoring and general horrendous noise of the ward. (Diagnosed primarily speaking white woman, aged 44, with A’ levels)
Furthermore, sharing their sensory needs with staff was identified as resulting in a negative response by one participant: “I was completely infantilised as a person throughout the entire experience and having known sensory issues and known mental illness only made this worse.”
Positive comments about the environment were rare but were the converse of these issues, including: “My delivery room had relaxing coloured lighting which really helped.”
Water births were commonly discussed, with the idea of birthing in water as a positive. Some participants described wanting a water birth but were not able to have this. One participant noted that they were told in advance that they were “too fat.” The remaining participants were unable to have a water birth because of being induced, baby coming too quickly, being “high risk,” needing an epidural, baby being premature, being monitored lying on their back, and not having a pool available. A small group of participants described having a water birth, and for most this was a soothing sensory experience: “[Described negative experience with a hospital birth] My next two births were home water births. They were much better for sensory control and being within my routine. I also love the sensory feel of water so felt safer.”
However, one participant noted that being in the pool provoked a strong negative sensory response for them: “I hoped for a water birth, but I could not bear the feel of water on my skin.” Another did not understand that they were allowed to move in the water so found the experience of a water birth dysregulating.
Overarching theme: Impacts of inaccessible maternity care on Autistic people
This theme is focused on the impact of inaccessible maternity care on participants. Most participants reported that their care—both antenatally and surrounding birth—did not meet their needs, and for many this led to feelings of distrust of maternity staff and birth trauma. Sometimes these issues were at least partly because of birth-related complications resulting in changes to care: “My birth plan was for a home birth but I had preeclampsia so suddenly ended up in a ward being induced. It was all a bit traumatic.”
This theme is reported in relation to two subthemes: consent, safety, and trust, which highlights many issues of treatment without informed consent, and (Dis)respect and meeting Autistic needs, which is focused on participants’ feelings about how they were generally perceived, and its impacts on how their needs were met or not.
Subtheme: Consent, safety, and trust
When asked why they did not share their diagnosis with maternity staff, some participants described that being Autistic was stigmatized and they had concerns they would receive punishing treatment, such as being forced into obstetrician led (“consultant led”) maternity care or social work involvement in the postnatal period. Only a minority of participants noted that the staff who had supported them specifically observed their choices or were respectful if a birth plan needed to change due to complications.
By contrast, reports of examinations and procedures without having given informed consent were common during birth, including vaginal examination, drugs being given, episiotomy (cutting the perineum—the skin between the vagina and anus), induction, continuous monitoring, and “stretch and sweep” of the cervix: “in labour with my first they never asked if they could do an episiotomy [before they did it] and it led to a complete meltdown mid labour.”
Among participants who reported resistance to this treatment, push back occurred. For example, a midwife who “was cross” when the participant asked for a vaginal exam to stop, coercion in relation to a vaginal exam, and trying to force agreement for an induction: “At 6 days [after my expected due date], a midwife told me if I didn’t consent to being induced they would forcibly take me to hospital and induce me against my wishes.” Even when participants were in significant pain, some reported that this coercion continued:
They never gave me a choice [about the pelvic exam during labour] and said I “have” to let them do it, I “can’t be difficult about this” “stop behaving this way” it was all very disrespectful. I was unaware I had a choice in any examination by a doctor. (Diagnosed primarily speaking white woman, aged 35, with a Master’s degree)
The importance of consent being fully informed for Autistic people, regardless of how invasive the procedure, was described by one participant, who had consented to having blood taken, but had not consented to have a canula inserted, resulting in significant distress. Others emphasized the importance of adequate processing time to allow for truly informed consent: “my HATING …”I’m just gonna” *Puts gel on me* “put this gel on you [to do an ultrasound scan]…”.
Some participants were very aware of the unequal power relations between themselves and maternity staff, with participants describing health professionals stating, or “threatening,” that they would make a referral for social work intervention, or that they could if the parent was seen as “making too much fuss” or “being difficult.”
Subtheme: (Dis)respect and meeting Autistic needs
Autistic people’s needs were reported to generally go unmet during their maternity care, as has been illustrated above in relation to communication, providing person-centered care, pain management, and consent. Most participants who responded to the open-text questions reported some aspect of their needs not being met, as illustrated here: “Not one of the people who dealt with me had any understanding and therefore offered no accommodations. They literally said I was being difficult and if I wasn’t learning disabled I should understand.”
Participants regularly reported that health professionals appeared to find them unpleasant, including feeling “disliked by staff,” being “infantilized,” and “threatened”. Staff also appeared to be irritated by Autistic ways of communicating, including reports of staff who were “annoyed,” “frustrated by my questions,” “awful and looked down their nose at me,” “disinterested and uncooperative,” “shouty,” and “horrible.” In this context, some participants worried about asking for too much or sharing their worrying symptoms: “often I felt like I was being a nuisance.” Others noted being “told off” and “dismissed.” Unsurprisingly, maternity care was viewed as “very frightening,” “horrific,” “barbaric,” “traumatic,” “belittling,” and resulting in some participants being “scared.” Furthermore, participants’ needs not being met led to them: being “anxious,” “overwhelmed,” or “terrified”; “experiencing unnecessary pain”; and “just gritt[ing] my teeth to get through it all.”
A minority of participants reported occasions where their needs were met; no participant reported only positive experiences. This included staff being knowledgeable and supportive, answering all questions, receiving continuity of care, and trying to secure accommodations for them: “the midwives looking after me tried [their] best to make sure anyone I had dealings with were made aware.” One participant noted that they had their accommodations granted, but grudgingly: “I have become better at getting my needs met, but at the expense of how I am spoken to, and treated like a monster.”
Discussion
Our study included 193 participants with lived experience of pregnancy. Participants' response to closed questions highlighted that they experienced increased sensory sensitivity during pregnancy, particularly relating to smell and touch. Moreover, they reported that this negatively impacted on their mental health and caused additional shutdowns and meltdowns, reinforcing systematic review findings. 15 While we found a similar rate of heightened smell to a previous survey, our participants reported heightened touch (63% vs. 23%), sound (48% vs. 9%), and light (34% vs. 4%) at much higher rates than has been previously identified. 24 Interestingly, over half of participants did not know that they were Autistic at the time of their maternity care, and over half were undiagnosed at the time of data collection. Although our findings were not statistically significant, possibly due to relatively small group sizes, those who were diagnosed or undergoing diagnosis at the time of data collection appeared to be similarly impacted by changes to sensory sensitivity, with both groups reporting to be more impacted than those who were self-identifying in relation to anxiety, discomfort, distress, shutdowns, and meltdowns. Sensory aspects of the clinical environment, including noise and lighting (as has been previously identified), 19 were also reported to impact on participants’ experiences of maternity care and particularly birth. While finding the postnatal ward overwhelming has been reported in a general population, 33 sensory pain appeared to impact our Autistic participants throughout more of their maternity care, as is well established. 15
Within maternity care, most participants quantitatively reported routinely “masking,” irrespective of diagnosis status, a finding previously identified in qualitative research. 18 However, for those without a diagnosis, it may be that they did not understand why something was difficult or know that they could request a change to their care, as has been reported in one autobiography. 34 Despite masking, participants reported that they were not listened to 16 and were misunderstood, 21 with rates of both reported more frequently (although not significantly so) in those undergoing diagnosis, both of which have been previously identified in surveys. Participants also reported they felt unsupported overall, which has not been assessed quantitatively previously. Comparing our quantitative findings regarding maternity care with those from the open-text responses, we feel that both sets of findings are consistent with no conflicting data, with the extent of feeling unsupported and negative experiences of maternity care clearly articulated, alongside the impact of this on them. Research on health professionals from a range of areas of medicine highlights that health professionals lack knowledge of Autism, can find communicating with Autistic people challenging, and that they may hold stigmatizing views of Autistic patients. 35 Responses to open-text questions appeared to be generally aligned to this, with miscommunication clearly articulated. 25
Specifically relating to pain, our participants regularly reported two avenues of miscommunication: one, they had clearly communicated their pain using verbal speech but were ignored, and two, difficulties reporting how much pain they were in. Challenges in conveying the extent of pain to maternity staff have been previously reported by Autistic participants 17 ; however, we feel that our analysis extends the severity of this. For example, 10 participants reported that they were in the second stage of labor, with the baby almost about to be born, and were still not believed by maternity staff. Furthermore, some respondents reported that they were denied pain relief or faced judgmental comments for requiring it, causing distress and some participants to not request analgesia further and repeating a finding briefly mentioned in previous research on the Autistic birth experience.18,20 There is evidence from a general population that unmanaged pain in labor is associated with birth trauma, 7 chronic pain, and postpartum depression. 36 Combined with the known higher prevalence of postnatal depression for Autistic people, 21 this highlights an urgent need for Autistic birthing pain to be adequately managed.
A smaller proportion of our participants highlighted that they struggled to understand health professionals’ communication to them, something that has been identified as more common in Autistic birthing parents compared with non-Autistic peers. 21 Furthermore, a minority of participants noted that they were unable to verbally express their needs, as has been previously identified, 18 although it should be noted that this was a much smaller number than those who reported that they had their clearly expressed needs ignored. In the context of miscommunications and being unable to communicate needs, partners played an important role in communicating with maternity professionals for one-fifth of participants, which has not previously been found in research. That said, almost half of our participants rarely had somebody attend maternity appointments with them, which was mostly unrelated to the COVID-19 pandemic. However, less than a fifth wanted to attend appointments alone. Partners and advocates can play an important part in ensuring the rights of Autistic adults are met in health care, 37 and thus for those without a supporter, the provision of suitably trained doulas may be worthy of exploration. This may be cost-neutral in some contexts, such as the United States, due to associated lower rates of cesarean-section births. 38
Furthermore, the lack of consent identified previously22,23 in qualitative studies and in our own quantitative findings was clearly articulated by many respondents in their descriptions of maternity care, with over a third not understanding the way things were explained to them, and almost half not given the option to decline physical examinations—something that has not previously been assessed quantitatively in Autistic people. Again, those who were undergoing diagnosis reported these at a higher (although not significantly so) rate than those who were diagnosed or undergoing diagnosis. Data from AIMS Ireland suggest that 68% of women in a general population gave consent for all tests, procedures, and treatments during birth, 39 and thus, it may be that Autistic people are less likely to receive care that prioritizes their consent, although the difference in country may also account for this. Open-text responses identified that this lack of explanation and consent included vaginal examinations and being pressured by health professionals to continue painful treatment.
Lack of control during birth is associated with birth trauma, 13 and while we did not ask a specific question on birth trauma, open-text responses highlighted issues previously associated with birth trauma, including repeated difficult communication with staff, 12 feeling misinformed, 13 and significant and sometimes lasting distress. 7 Moreover, Autistic women are known to be at much higher risk of sexual assault than their non-Autistic peers, with one study reporting that 90% had a history of sexual assault. 40 For sexual abuse survivors in a general population, not being given the choice to consent during maternity treatment could be triggering and retraumatizing. 41 Additionally, Autistic people with a history of sexual assault have noted that their abusers tactics included gaslighting and coercion, 42 which Autistic people may find harder to understand than non-Autistic people. 43 Some of our participants reported aspects of their care, which could be perceived as aligned to gaslighting and coercion, which may be additionally retraumatizing. As such, Autistic people with a history of sexual assault may be retraumatized by maternity care experiences that are similar to those reported by our participants.
Our participants reported that staff appeared to have limited time, and this may have contributed to many of the issues reported. Additionally, continuity of care was atypical, as is found in a general population, 44 although previous research has found that sharing an Autism diagnosis may result in continuity of care being provided. 19 In this context, we find it unsurprising that participants reported few positive examples of communication between themselves and their maternity professionals. Alongside system-level barriers, and while we do not know the neurotype of the health professionals involved, it may be that the double empathy problem—where non-Autistic people expect Autistic people to behave neurotypically, while they do not have to change their behavior to meet Autistic needs—is occurring. 45 It has been further theorized that in health care settings, there may be an additional lens of lay patient/expert provider to add to the double empathy problem, leading to a “triple empathy problem.” 46 This may account for some of the instances where our participants reported that they were confused or did not understand what was happening. A more neurodiversity affirming approach to Autism may result in less expectation for Autistic people to change should providers and services be unable to remove system-level barriers to Autism-friendly care. 47
Implications for practice
One of the strongest recommendations from our participants was for continuity of care. Participants noted that this did not appear to be routinely available. The advantages of having continuity of care are well documented in a general population, including patient satisfaction and lower rates of preterm birth, but they also provide particular benefit to those who have complex needs or who are marginalized. 48 An additional recommendation was for there to be more time available during antenatal appointments to meet the needs of Autistic people, an accommodation that has been recommended for other groups with increased adverse pregnancy outcomes. 49 Although our participants did not request it, we believe that using trauma informed approaches to maternity care 50 may have particular benefits for Autistic people. This is in light of the high levels of misunderstandings and lack of consent reported in our study, alongside the known higher incident of sexual violence 40 and greater propensity toward posttraumatic stress disorder. 14 Arguably, some of our participant experiences would be indicative of poor maternity care experiences regardless of neurotype, such as failing to obtain consent. Accordingly, we believe that implementing these service changes for all service users would be of benefit through the principle of Universal Design. 51 This approach may have particular benefits for undiagnosed Autistic people and those who do not feel comfortable to share their diagnosis, as well as other marginalized groups.
The barriers participants reported in relation to meeting Autistic needs have been found in other research, which has also highlighted that these barriers result in adverse health outcomes. 52 The complexity of removing these barriers in routine health care services has been highlighted in a realist analysis. 53 Accordingly, we suggest that Autistic people should be offered the opportunity to be referred to continuity of care maternity teams if specialist Autism in pregnancy services are not available. Wherever possible, Autistic people should be given private rooms during inpatient treatment and should be offered a private waiting area. Noise and light within clinical environments were felt to be particularly challenging, and accommodations relating to this would reduce the pain felt from the sensory environment, potentially making examinations and treatment more tolerable.
Although Autism is a lifelong disability, many of our participants had not yet been diagnosed when receiving maternity care. As such, it is essential for staff working in maternity services to understand the communication style, pain presentation, and sensory needs of Autistic people. Many of our participants highlighted that they had clearly articulated their needs using spoken words, but that this had been ignored. This included in relation to severe pain and babies being very close to being born. A smaller number struggled to articulate their needs. As such, quality improvement interventions should be focused on providing knowledge to all maternity professionals about how Autistic people communicate. Regardless of neurotype, it is essential that informed consent is gained. Many participants suggested that communication should be multimodal, with services providing information to take away after appointments, and this may result in greater levels of informed consent. In addition to this, it may be that when supporting Autistic people, maternity staff need to answer more (and sometimes many more) questions to allow the person to feel comfortable consenting. They should also allow for additional processing time, so that it is available if required.
Strengths and weaknesses
We received 193 responses to our online survey, and participants provided in-depth open-text accounts in addition to completing closed-text questions, building on knowledge from previous qualitative studies. Our team was led by an Autistic researcher, and our research design was influenced by consultation with the Autistic community and other Autistic researchers. However, our participants were a motivated sample responding to a social media advertisement. This may account for a high percentage of participants being white, cisgender, and highly educated. Additionally, many of our sample said they were disabled in addition to being Autistic, which may have influenced their responses. We did not ask participants if they had a learning disability. Together, this means that our findings may not reflect all Autistic experiences. Furthermore, many of our participants were not diagnosed, which may have impacted their care. Moreover, as this is a relatively understudied area, we did not put a limit on how recently a participant needed to have given birth, the mean age of children was seven, and the oldest “child” was 39 years old at the time of data collection. This means that participants may have been impacted by recall bias, 54 and some participants’ experiences may not reflect current practice. A further issue is that our study, like many others, was primarily focused on the health care participants had received. Future research could usefully focus on the wider aspects of maternity, including relationships with partners and families and how pregnancy impacts education and employment.
Conclusion
Our research highlights many challenges experienced by Autistic people during their UK-based maternity care, some of which have been reported in research undertaken in other countries. Moreover, there was a high degree of reporting of concepts known to be associated with birth trauma in a general population, including poor quality interactions with maternity staff, feeling that they were not well informed regarding treatment and feeling unsupported. There is an urgent need for evidence-based improvements in the health care given to Autistic birthing people. Our study suggests improvements are required in relation to knowledge of Autism, particularly focused on communication and pain expressions, continuity of care, longer appointment times, and improvements to the sensory environment.
Footnotes
Acknowledgments
The authors acknowledge Eleanor Healer, Rebecca Ellis, and Hayley Morgan who reviewed a draft of the survey. Carol McIntyre undertook data cleaning, and Danielle Bird proofread the article. The authors wish to thank the administrators of the Facebook groups who facilitated recruitment and the participants who took time to complete the survey.
Authorship Confirmation Statement
A.G.: Conceptualization, methodology, formal analysis, data curation, writing—original draft, writing—reviewing and editing, and funding acquisition. C.G.: Formal analysis, writing—original draft, and writing—reviewing and editing. K.W.: Conceptualization, methodology, formal analysis, writing—reviewing and editing, and funding acquisition. A.B.: Conceptualization, methodology, formal analysis, supervision, writing—reviewing and editing, and funding acquisition. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
A.G. is a nonexecutive director for Disability Wales. K.W. is a nonexecutive director for Autistic UK. The other authors report no conflicts of interest.
Funding Information
The study was funded by Swansea University’s Accelerate Healthcare Technology Centre.
a
We capitalize “Autistic” and Autism throughout this article as a marker of culture, community, and identity.
b
The term “stimming” refers to a range of different behaviors, including moving one’s body or making a particular vocalization, which soothes an Autistic person. They often impact on one or more sensory systems.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.