
Abstract
Background:
Autism terminology is highly controversial. The debate regarding person-first and identity-first language is particularly well-studied, but the present study explores views on different terms commonly used to describe autism, such as “disorder,” “disability,” and “difference.” Furthermore, unlike prior studies, this study explores how terminology views are related to identification with the neurodiversity movement (NDM).
Methods:
We collected usable survey data from 475 participants, 271 of whom were autistic and 204 of whom were non-autistic interested parties (e.g., family members, professionals). Participants rated perceived appropriateness of 13 terms as descriptors of autism. They also indicated whether they had heard of neurodiversity and the social model; if yes, they respectively completed a brief measure of NDM identification and/or answered an item rating support for the social model.
Results:
Overall, participants rated the terms “condition,” “developmental,” “disability,” “difference,” “neurodiverse,” “neurodivergent,” “neurominority,” and “neurotype” as more appropriate than neutral, whereas “deficit,” “disorder,” “illness,” “psychopathology,” and “syndrome” were seen as inappropriate. As participants identified more strongly with the NDM, they rated the terms “neurodiverse,” “neurodivergent,” “neurominority,” and “neurotype” as more appropriate; however, they rated “condition,” “deficit,” “disorder,” “illness,” and “syndrome” as less appropriate. In non-autistic people only, perceived appropriateness of “developmental” decreased with increasing neurodiversity identification. In autistic participants only, perceived appropriateness of “disability” increased with greater neurodiversity identification.
Conclusion:
Both autistic and non-autistic participants in this study robustly preferred neurodiversity-aligned terms, such as “neurodivergent” and “difference,” to traditional terms assuming pathology and deficiency. Participants also generally approved of the term “disability,” particularly autistic participants identifying with the NDM, aligning with the NDM’s recognition of both autism-related strengths and challenges. Although we cannot rule out sample bias, our data suggest an emerging consensus supporting discussion of autism in positive or neutrally descriptive ways or through acknowledging challenges in a nonderogatory manner.
Community Brief
Why is this an important issue?
People have many different opinions about the words we should use to describe autism. For example, some people use words like “disorder” and “deficit” to describe autism. Some autistic people think these words are offensive and harmful.
What was the purpose of this study?
This study explored how people feel about different words that are often used to describe autism. We wanted to know if people who are more supportive of the neurodiversity movement like different words than those who support it less.
What did the researchers do?
A total of 271 autistic people and 204 non-autistic people with connections to autism (including family members and researchers/professionals) completed our online survey. They rated how appropriate they felt different words were for describing autism. We also asked whether they supported the neurodiversity movement.
What were the results of the study?
Participants (including autistic participants) often said that the words “neurodivergent,” “neurodiverse,” “neurotype,” “difference,” “disability,” “neurominority,” “developmental,” and “condition” were appropriate. The terms “illness,” “deficit,” “psychopathology,” “disorder,” and “syndrome” were often seen as inappropriate.
Neurodiversity movement supporters often rated “neurodiverse,” “neurodivergent,” “neurominority,” and “neurotype” highly. Neurodiversity supporters rated “condition,” “deficit,” “disorder,” “illness,” and “syndrome” less highly.
The more that autistic participants supported the neurodiversity movement, the more highly they rated the word “disability.” This was not the case for non-autistic participants. This may suggest that autistic people are less likely to see disability as a bad thing.
Autistic people’s views on the terms “developmental” and “difference” were not related to neurodiversity movement support. This suggests that these words were well liked by autistic people with different views about autism and neurodiversity.
What do these findings add to what was already known?
We found that support for the neurodiversity movement is connected to a range of words people think should be used to describe autism. These findings extend beyond previously studied links between awareness of the neurodiversity movement and preferences for identity-first language (e.g., autistic person). We found that many autistic people, especially neurodiversity movement supporters, are comfortable thinking of autism as a developmental disability.
What are potential weaknesses in the study?
Participants did not represent the larger community well. For example, participants came from a few mostly English-speaking Western countries. Supporters of the neurodiversity movement were probably more likely to participate in this study than people who do not support the movement. Thus, our participants probably liked certain words more or less than autism community members generally.
The study only examined participants’ views about words when they are used to describe autism. It is not clear what participants might think about words for other disabled and neurodivergent identities, like ADHD or epilepsy.
How will these findings help autistic adults now or in the future?
These findings will help people choose respectful words to talk about autism. We can respect community members using words they like. These findings show that many words that are often used to describe autism—such as “deficit” and “disorder”—are often disliked and should be avoided whenever possible. Terms like “difference” or “neurodivergent” may be preferred.
Background
Identity and respectful terminology are very important to many autistic people,1–3 similar to many other marginalized communities (e.g., groups marginalized due to race/ethnicity/indigeneity, sexuality, or gender).4–6 Much prior debate7–11 and research (reviewed by Archibald et al. 12 ) have centered around whether autism should be described using person-first language (PFL, e.g., “person with autism”) or identity-first language (IFL, e.g., “autistic person”). IFL is championed by many supporters of the neurodiversity movement (NDM). Although there is a diversity of perspectives within the NDM, a prior publication from our research group revealed that many participants in the present study defined the NDM as an evolving movement championing acceptance and thriving of neurodivergent people, advocating for societal reforms, and opposing automatic pathologization of differences. 13 The PFL/IFL debate is only one of many debates about autism terminology.14–17 Recent neurodiversity-affirming 18 guidelines challenge a variety of traditional terminology choices,15,16,19–21 but some strongly object to these guidelines. 22 Community preferences regarding broader terminology disputes are generally less well-studied than PFL/IFL disputes.
One important question is how autism should be conceived and described: for example, as a “disorder,” “condition,” or “disability”? Diagnostic manuals describe autism as a “disorder,” 23 but many autistic people regard this as offensive 2 ; the alternative “condition” is also frequently seen as offensive, 2 and opinions regarding “Autism Spectrum Condition” appear tepid even in the United Kingdom, 24 where it is most popular. 25 Relatively neutral descriptors might be alternatives to these value-laden terms. For example, autism could be regarded as a “developmental” construct 26 or “difference.” 27 One study suggests that “difference” may be particularly popular among autistic adults. 25
Another alternative, “disability,” has been rated similarly 28 or preferably 25 to “condition.” However, these findings are complicated by the ambiguity of “disability.” 7 From a medicalized perspective conceptualizing disability as the result of individual functional limitation, “disability” and “disorder” might appear virtually synonymous. Perhaps due to such semantic confusion, people outside the NDM often believe that the NDM rejects the idea of disability, although neurodiversity advocates protest this misrepresents their position.29,30 Within social and social–ecological models of disability, disability is at least partly attributable to societal barriers and oppression requiring accommodation or amelioration rather than only individual neurological or physical differences,13,31 so “disability” need not reflect a value judgment about the inherent worth or desirability of individual differences.
The NDM provides many possible descriptors of autism. After the term “neurodiversity” was introduced to describe the diversity of human minds and brains,32–35 it was applied to describe “neurodiverse” people and groups. However, some authors36,37 argue that “neurodiverse” should not be used as a synonym for “neurodivergent,” 38 which refers specifically to those with minds/brains/behavior diverging from societal standards and norms. For some, “neurominority” 37 is a more accurate way to refer to neurodivergent people. Similarly, “neurotype” describes groups of individuals sharing similar minds/brains, whether neurotypical or neurodivergent. Whether “neurotype” is considered appropriate may relate to essentialism; scholars dispute how much neurodiversity advocates essentialize autism as a discrete biological entity versus having more nuanced perspectives.27,39–44 “Neurotype” 28 and “neurodivergent” 25 attracted strong support in prior surveys; otherwise, preferences regarding neurodiversity-affirming terminology remain unclear.
Autistic people’s views on autism terminology are influenced by their identities, communities, and other characteristics. 45 Research conducted over a decade ago revealed positive associations between NDM awareness and support for IFL. 27 However, relationships between terminology preferences and NDM support—arguably more relevant today than NDM awareness—have not been studied.
One general issue affecting many prior autism terminology studies is that autism studies are seldom if ever representative,46–49 and different recruitment approaches yield participants from communities with different opinions about terminology. 12 For example, a recent study using the Pollfish online survey platform to recruit autistic people in the United States 50 reports markedly different preferences regarding IFL/IFL compared with prior U.S. studies of autistic people.25,51 Thus, conclusions that community members like/dislike certain terms may be premature. However, relating preferences to NDM support could help characterize the views of people with different perspectives, yielding more nuanced insights about how best to respect their language preferences. For example, it might help professionals and allies choose terms that are likely to be acceptable to individuals with diverse viewpoints or how to choose terms calibrated to a particular audience (while respecting specific autistic people’s preferences when known 15 ).
Methods
Participants in this study, which is part of a larger project about autism intervention preferences and the NDM,13,52 were recruited online via social media and by asking autism organizations and community leaders to disseminate study information; participants had a 1/25 chance of winning a $25 USD gift card. The UC Davis Institutional Review Board reviewed the study and determined it to be exempt research. The study required participants to complete an ∼50-minute online survey. Participants were adults with a connection to autism (self-identified or formally diagnosed autistic people, family members, researchers, clinicians, educators, other professionals, or other self-described connection). After removal of invalid/fraudulent data (n = 960 responses holistically coded as putatively invalid, after two coders achieved 98% agreement on a subset of responses, as described by Dwyer et al. 13 and Hersh et al. 52 ) and incomplete responses whose provenance could not be determined, 475 participants provided terminology preference data. Autistic participants (n = 271; 159 female, 40 male, 72 nonbinary/other) included 52 parents and 44 other family members of autistics, along with 39 researchers and 35 other clinicians/educators/professionals. Non-autistic participants (n = 204; 171 female, 30 male, 3 nonbinary/other) included 99 parents, 28 other family, 55 researchers, and 76 professionals/educators/clinicians. Supplementary Tables S1 and S2 in Supplementary Data provide further details.
Measures
These measures come from a larger mixed-methods study about community views on neurodiversity and autism intervention.13,52
NDM identification
Participants were asked, “Have you heard the term ‘neurodiversity’?” If yes, an adapted 5-item disability identification measure52,53 measured feelings about NDM, for example, “I’m glad to be a supporter of the neurodiversity movement.” Response options ranged from “Strongly Disagree” (1) to “Strongly Agree” (7). We also presented a single-item question directly asking, “Do you support the neurodiversity movement”; results involving this question are Supplementary Table S5 in Supplementary Data.
Social model of disability
Participants were asked, “Have you heard of the social model of disability?” If yes, they were asked, “Do you support the social model?” Response options ranged from “Strongly Oppose” (1) to “Strongly Support” (6).
Terminology preferences
Participants were asked: “How appropriate do you think each of these terms is as a descriptor of autism? (Please think about autism itself, not co-occurring conditions, when formulating your answers).” The words “condition,” “deficit,” “developmental,” “disorder,” “disability,” “difference,” “illness,” “neurodiverse,” “neurodivergent,” “neurominority,” “neurotype,” “psychopathology,” and “syndrome” were presented. Responses ranged from “Extremely Inappropriate” (1) to “Extremely Appropriate” (6) with Highly and Slightly In(appropriate) as intermediate scores.
Analysis
One-sample Wilcoxon tests evaluated whether participants rated terms as more or less appropriate than neutrality (i.e., 3.5). Wilcoxon–Mann–Whitney tests then compared groups’ terminology preferences. These results are presented Supplementary Table S3 in Supplementary Data and summarized in the text.
Kendall’s ordinal correlations quantified associations between NDM identification and perceived term appropriateness, separately in each group. Afterward, Kendall’s τ coefficients were converted to Pearson’s r 54 equivalents and compared across groups. 55
Supplementary analyses examined, separately in the autistic and non-autistic groups, whether terminology preferences were affected by being an autism professional (including clinicians, educators, and researchers) or by being a parent of autistic people.
Analyses were performed in R Studio. Terminology preference p-values are reported with Benjamini–Yekutieli false discovery correction 56 for 13 comparisons.
Results
Internal consistency of the NDM identification measure was excellent, Cronbach’s α = 0.94. As previously reported,13,52 most participants had heard of neurodiversity and identified as NDM supporters; NDM identification was slightly higher in autistic than non-autistic participants.a, 57 Only 81% of autistic and 55% of non-autistic participants had heard of the social model, but most who heard of it supported it.b, 58
Overall preferences
Collapsing across groups (Supplementary Table S3 in Supplementary Data), the terms “condition,” “developmental,” “disability,” “difference,” “neurodiverse,” “neurodivergent,” “neurominority,” and “neurotype” were rated significantly more appropriate than neutral (Fig. 1). The terms “deficit,” “disorder,” “illness,” “psychopathology,” and “syndrome” were rated significantly less appropriate than neutral.
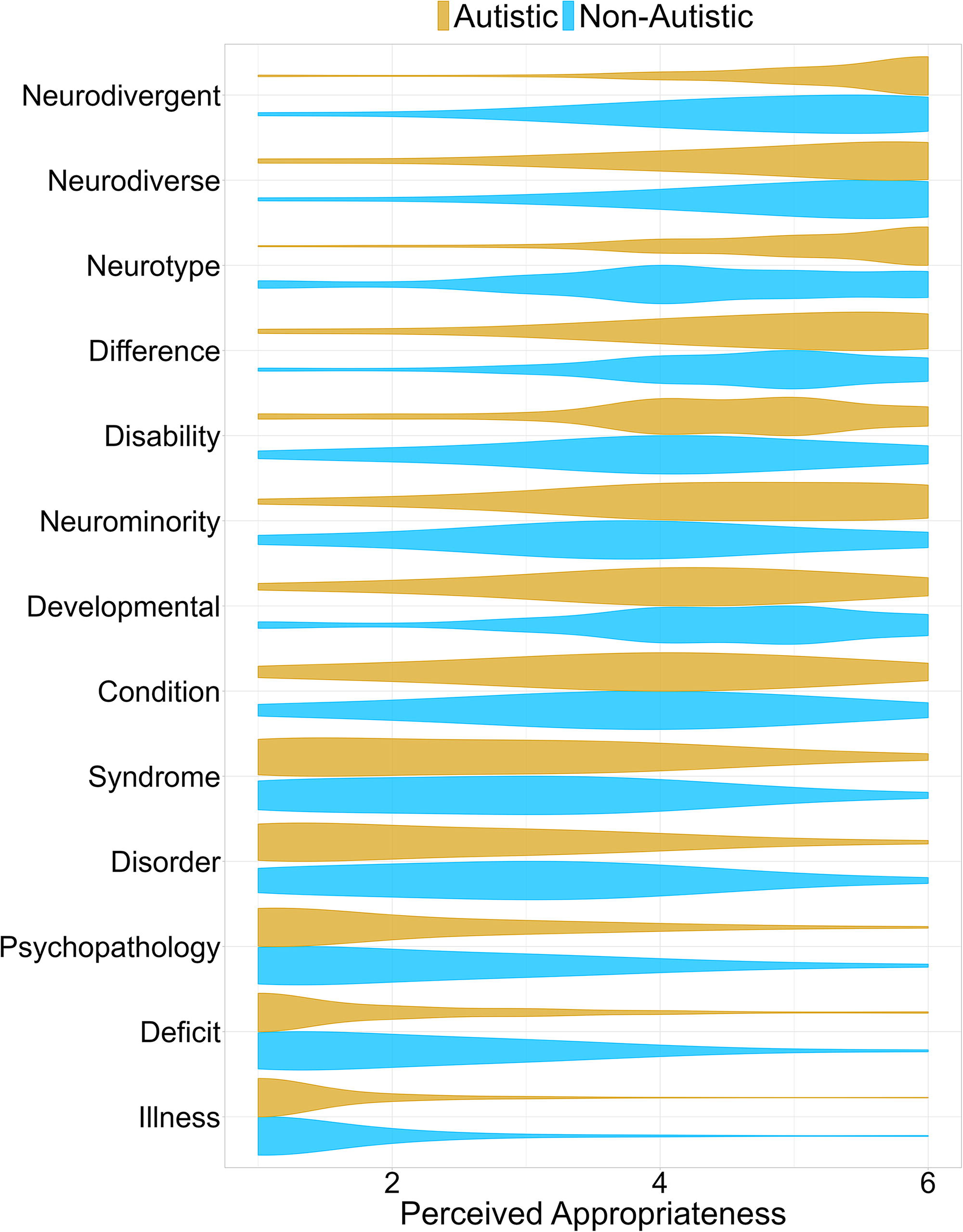
Violin plot depicting perceived appropriateness of various terms as descriptors of autism, according to autistic participants (gold) and non-autistic participants (blue). Terms are arranged in order from greatest to least mean perceived appropriateness.
Group comparisons
Groups did not significantly differ in preferences for “condition,” “difference,” “illness,” “neurodiverse,” and “syndrome” (Fig. 1; Supplementary Table S3 in Supplementary Data). Non-autistic participants rated the term “developmental,” as more appropriate relative to autistic participants, although it was rated at least slightly higher than neutral in both groups (Supplementary Table S3 in Supplementary Data).
While non-autistic participants also rated the terms “deficit,” “disorder,” and “psychopathology” as more appropriate relative to autistic participants, participants in both groups rated these terms as inappropriate overall (Supplementary Table S3 in Supplementary Data). Autistic participants rated “disability,” “neurodivergent,” “neurominority,” and “neurotype” as more appropriate than non-autistics did, but participants in both groups considered these terms appropriate (Supplementary Table S3 in Supplementary Data).
As described in the supplement, there was no evidence that terminology preferences were influenced by being an autism professional (including clinicians, educators, and researchers) or by being a parent of autistic people.
Correlations
Ratings of the appropriateness of “condition,” “deficit,” “disorder,” “illness,” and “syndrome” were negatively associated with NDM identification in both groups (Table 1; Supplementary Fig. S2 in Supplementary Data). “Psychopathology” was negatively associated among autistic participants, but only at a trend level in non-autistics. Conversely, appropriateness ratings of “neurodiverse,” “neurodivergent,” “neurominority,” and “neurotype” were positively associated with NDM identification (Supplementary Fig. S3 in Table 1, Supplementary Data). Despite a positive trend, ratings of “difference” were not significantly associated with NDM identification (Supplementary Fig. S4A in Supplementary Data).
Ordinal Associations, Specifically Kendall’s τ, Between Appropriateness Ratings for Different Terms and NDM Identification, Separately in Autistic and Non-Autistic Participants and Compared Across Groups
As Kendall’s τ coefficients were converted to the same metric as Pearson’s r before group comparisons, Zou’s 95% CI of the differences of the correlation coefficients across groups should not be directly interpreted as reflecting values of group differences in τ. (Values of τ are systematically smaller than Pearson’s r.) All p-values use the Benjamini–Yekutieli correction for 13 comparisons (13 terms).
CI, confidence interval.
Interestingly, correlations between NDM identification and terminology preferences differed across groups for “developmental,” “disability,” and “neurodiverse” (Table 1). Higher ratings of “developmental” were associated with reduced NDM identification in non-autistics, but not in autistic participants (Supplementary Fig. S4C in Supplementary Data). Ratings of “neurodiverse” were positively associated with NDM identification in both groups but more strongly among non-autistics. Rating “disability” as more appropriate was associated with greater NDM identification in autistic participants, but there was a nonsignificant-after-correction trend for it to relate to reduced NDM identification among non-autistics (Supplementary Fig. S4B in Supplementary Data).
Generally, similar results were obtained when correlations with a single-item measure of neurodiversity support were examined (Supplementary Table S5 in Supplementary Data).
Exploratory “disability” analyses
An exploratory ordinal logistic regression 59 predicting ratings of the term “disability” from whether participants were autistic and whether participants had heard of the social model found that participants aware of the social model rated “disability” as more appropriate, p = 0.001, with no effect of group and no interaction. However, supplementary analyses suggested that the association between NDM identification and ratings of “disability” did not differ across those who had/had not heard of the social model, p = 0.20 (Supplementary Table S4 in Supplementary Data). Instead, the direction of associations between NDM identification and perceived appropriateness of the term “disability” differed between autistic (positive) and non-autistic people (negative) regardless of whether they had heard of the social model, p < 0.0003 (Supplementary Table S4 in Supplementary Data).
Discussion
The present study explored perceived appropriateness of various terms as descriptions of autism in a large sample representing a variety of community members, including autistic people, family members, researchers, and professionals.
Overall, in a sample of participants mostly identifying as NDM supporters, we observed high support for neurodiversity-aligned terminology among both autistic and non-autistic respondents. The terms “neurodiverse,” “neurodivergent,” “neurominority,” and “neurotype” were all rated more positively as NDM identification increased, and they were also overall seen as appropriate. “Difference” was also seen as appropriate, although a trending positive association between ratings of “difference” and NDM identification did not attain significance in either group—possibly suggesting that the term “difference” is relatively nonpolarizing.
In contrast, when terms’ perceived appropriateness was negatively associated with NDM identification (suggesting the terms are not neurodiversity-affirming—a conclusion congruent with relevant guidelines 15 ), the terms were generally rated as inappropriate: this was the case for “deficit,” “disorder,” “illness,” and “syndrome.” “Psychopathology” was significantly negatively associated with NDM identification in autistic participants, and at a trend level in non-autistic participants, and it too was seen as inappropriate. Thus, participants did not favor terminology opposed to the NDM.
While this clearly suggests that terms such as “deficit” should be avoided in most autism contexts, there may be some contexts where this is not practical. For example, if policies require clinicians writing assessment reports to provide evidence of “deficits” to justify access to supports, then clinicians could still incorporate other aspects of neurodiversity-affirming practice, such as partnering with clients, ensuring accessibility, and post-diagnostic support.60,61
Opinions about the term “condition” were technically an exception to the general rule of neurodiversity-aversive terminology being opposed. The term did not appear NDM-aligned; autistic and non-autistic participants saw “condition” as increasingly inappropriate if they identified more strongly with the NDM. Nevertheless, “condition” was seen as more appropriate than neutral—but its median rating was only “Slightly Appropriate,” and after correction, appropriateness ratings did not differ from neutral in non-autistic participants. Thus, participants hardly appeared enthusiastic about “condition”; neurodiversity-aligned terms were more favored.
Participants’ opinions regarding “disability” appeared more complex. Although both autistic and non-autistic people generally considered the term “disability” appropriate, autistic people gave it higher ratings. People adopting social and social–ecological models of disability view “disability” as being at least partly caused by societal barriers/discrimination.13,31 In contrast, those unfamiliar with these ideas may see “disability” as individual weakness or failing. Autistic people were more familiar with the social model, and exploratory regression indicated that participants familiar with the social model viewed “disability” as more appropriate. After accounting for social model awareness, autistic and non-autistic people’s ratings no longer appeared to differ. However, follow-up analyses revealed inverse patterns of associations between NDM identification and perceived appropriateness of the term “disability” among autistic and non-autistic participants, regardless of their awareness of the social model. Among autistic people, the term “disability” was seen as more appropriate as NDM identification increased. Among non-autistic people, “disability” trended toward being seen as less appropriate by NDM supporters. As noted above, these inverse associations were seemingly not driven by social model awareness, suggesting that they may reflect different concepts of the NDM. Some neurodiversity advocates opine that people outside the NDM,30,62 including numerous neurotypical people, 63 may misunderstand the NDM as rejecting disability and disability-related support needs. Notably, in this dataset, we observed that non-autistic people were more likely to define the NDM around celebrating differences, which we interpreted in terms of “neurodiversity lite” (e.g., co-option of the NDM through marketing “superpowers”),13,64 whereas autistic people more often spoke of the NDM reforming society and promoting thriving. 13 This may reflect an understanding of the NDM more focused on practical disability-related barriers and support needs among autistic relative to non-autistic people.
Our findings regarding the term “disability” align with a recent study examining terminology preferences among autistic people internationally, in which “disability” was also highly rated. 25 Participants in that study provided diverse reasons for their ratings, including references to the social model, NDM-aligned biopsychosocial descriptions highlighting a lack of shame in acknowledging difficulties, “disability’s” utility in advocating for supports, 25 and the context dependence of desirable terms based on what they were being used to accomplish.
In this study, opinions regarding “developmental” were also complex: as non-autistic people’s NDM identification increased, they rated “developmental” as less appropriate, but no such association was observed in autistic participants. Understanding this finding is challenging, and both the study authors and peer reviewers generated varied and somewhat speculative interpretations. We briefly highlight several here. Neurodiversity groups have long applied the term “developmental” to early-onset neurodivergences, such as ADHD and dyspraxia, in a descriptive but nonderogatory manner. 65 However, it is possible that non-autistic people may be more frequently exposed to pathologizing uses of “developmental,” such as “developmental disorder” and “developmental delay,” and developmental frameworks might be cited in justifications for controversial interventions. 66 Potentially, NDM-supporting autistic participants’ comfort with “developmental” might have been elevated by personal experiences of adaptive functioning challenges14,67–69 and related (potentially unmet) support needs.70–72 Furthermore, views could relate to perspectives on autism’s etiology. However, although dynamic and transactional origins are emphasized in much contemporary developmental science, community members may instead understand “developmental” to imply innate or biological origins. 73 Autistic and non-autistic participants could have differed in underlying unmeasured factors, such as knowledge about or opinions regarding research or clinical concepts, such as diagnostic criteria and “mental age.” 74 Overall, it is unclear why NDM identification and ratings of “developmental” are inversely associated in non-autistics, but not autistic people.
Limitations
The most important limitation of this study is that, like many autism studies, the sample does not appear to be representative. As shown Supplementary Table S1 in Supplementary Data, like other online studies, 46 the autistic sample contains disproportionate numbers of late-diagnosed women and nonbinary participants. Women were also over-represented in the non-autistic sample, perhaps because caregiving and autism service provision are associated with female gender roles. Non-Hispanic White participants predominated, even though some racialized advocates have expressed concerns regarding mainstream NDM-aligned terms. 75 Although underpowered, preliminary data from this project suggest that racial/ethnic groups may differ in NDM support/identification. 76 Furthermore, the ∼50-minute survey likely created systematic barriers to research participation (e.g., if participants’ lives did not permit sufficient spare time or due to communication or reading disabilities).
We did not obtain feedback on the accessibility and interpretability of survey questions from nonacademic community members, nor did we ask about participants’ knowledge of non-English languages, or whether English was their first language. As cognate terms’ connotations and precise meanings may differ across languages, it is quite possible that participants’ knowledge of other languages and/or academic jargon may have affected their responses.
Furthermore, while we strove to recruit participants from platforms generally associated with widely different views on the NDM, we are concerned that some NDM opponents may have declined participation due to pro-neurodiversity study team members being more familiar and trusted in their own networks and because the study was advertised as being about autism intervention and “neurodiversity.” This may have resulted in an exaggeratedly pro-NDM sample, notwithstanding possible “neurodiversity lite” views within the sample. However, while true population NDM support is nuanced and difficult to assess, it does appear to be increasing: NDM awareness in this study was much greater than in past similar research, 27 although some suggest that the NDM’s rise is paralleled by increasing misunderstandings or even co-option of the NDM.63,77 Many groups have softened or reversed anti-NDM stances or adopted more neurodiversity-affirming language. If possible, future studies should aim to survey opinions from relatively representative population databases, or to at least inquire of participants how they heard about the study. However, given how central online spaces have been to the NDM’s development (and to opponents such as vaccine skeptics),27,78,79 our focus thereon may be well-suited to illuminate views of the autism community.
One further limitation may be that participants may have had different understandings of the meaning of the NDM. Notably, in a previous publication 13 exploring understandings of the NDM in the present study’s sample, we found some evidence to suggest that some participants may have operated under “neurodiversity lite” 64 interpretations. Thus, quantitative ratings of NDM support and identification may mean different things from different people.
Insufficient qualitative data about terminology preferences limit our ability to interpret patterns. The terminology preferences collected in the present study refer to autism itself. Neurodiversity supporters have emphasized that the NDM opposes the forced suppression or “treatment” of autistic differences, but that a more traditional medical approach is often compatible with the NDM and appropriate for addressing—for example—epilepsy or gastrointestinal issues.13,40,80–82 It is unclear whether such variations in acceptability of intervention aims might also be accompanied by variations in terminology preferences. Furthermore, the term “neurodiversity” emerged in an autism-focused community 35 ; levels of NDM support and neurodiversity-related terminology preference in neurodivergent communities beyond autism also require investigation. For example, might neurodiversity-related terminology preferences in other neurodivergent communities be affected by co-occurrence with autism (and thus a community’s exposure to the autistic community), or by when in development a given disability/difference is acquired?
Conclusions
Although the present study sample is not representative, most participants decisively favored autism terminology aligned with the NDM while rejecting traditional NDM-misaligned terms such as “disorder” and “deficit.” Interestingly, although autistic participants often had a slightly greater preference for NDM-aligned terms, autistic and non-autistic participants’ ratings were fairly similar overall. Unfortunately, diagnostic manuals, service systems, and many research publications continue to use or even mandate traditional, NDM-misaligned terms, which is concerning given participants’ clear rejection of those terms. Our results generally support guidelines calling on researchers and other interested parties to reconsider traditional language.15,16,19,20 However, this is not a call for unrealistically positive Pollyannaish or Panglossian terminology. One of the terms participants strongly supported was “disability,” which acknowledges challenges experienced by autistic and neurodivergent people—but crucially, to participants aware of social or social–ecological models of disability, the term “disability” should not imply inappropriate negative value judgments about the disabled individual. Thus, terms recognizing real challenges and difficulties can clearly be appropriate, but writers and speakers discussing autism should refrain from terms that might reflect negative judgments of or stigma toward autism.
Footnotes
Acknowledgments
The authors warmly thank the participants for taking the time to take part in this study. The authors thank David S. Chang for support with the removal of the invalid data.
Authorship Confirmation Statement
P.D., S.K.K., K.G.-L., and S.M.R. designed this study. P.D. and L.H.H. analyzed the study data. This article was drafted by P.D. and edited and approved by all authors. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
No authors have any specific conflicts of interest to declare, except for having been involved in the autism field for varying durations and being associated with prior publications and work using various terminology choices.
Funding Information
Funding was provided by the UC Davis MIND Institute. P.D.’s time was partially supported by an Autism Speaks/Royal Arch Masons CAPD Fellowship. L.H.H.’s time was partially supported by a UC Davis Dean Keith Simonton research award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.