
Abstract
Community Brief
Why is this an important issue?
Many Autistic adults seek mental health support from psychologists, but traditional approaches to therapy might not always be a good fit for them. Professionals such as psychologists have started using the term “neurodiversity affirming” to describe their work, and multiple Australian guidelines say that healthcare professionals should provide neurodiversity affirming care to Autistic people. However, there is no clear agreement on what neurodiversity affirming psychology practice involves. This is an important issue because Autistic adults deserve therapy that works for them, does not cause harm, and respects and supports their unique needs and strengths.
What was the purpose of this study?
We wanted to define what it means for psychologists in Australia to offer “neurodiversity affirming” support to Autistic adults.
What did the researchers do?
We used the Delphi technique, which involves gathering knowledge from people with relevant expertise (“expert panel members”) and asking questions over a series of “rounds” to reach agreement. The 28 experts who took part in this study were Autistic adults who had seen a psychologist, and Autistic and non-autistic psychologists who believed their work was neurodiversity affirming. In Round 1, we gathered the panel members’ opinions on essential aspects of neurodiversity affirming support using open-ended questions. In Round 2, panel members rated statements for importance, and in Round 3, they re-rated items that they had not agreed on in Round 2.
What were the results and conclusions of the study?
The expert panel members agreed on 104 statements that were an important part of neurodiversity affirming psychology practice. We used reflexive thematic analysis to create a model with seven principles that describe neurodiversity affirming psychology practice for Autistic adults. These principles are about psychologists having a commitment to ongoing learning about autism, creating a safe space for Autistic people to be themselves, finding ways to communicate with each individual, being authentic and humble in their work, validating Autistic experiences, providing support centered on the person, and genuinely accepting and appreciating autism as a valuable way of being.
What is new or controversial about these findings?
While Autistic advocates and psychologists have been sharing information about neurodiversity affirming psychology practice for some time, before this study, there was no research-based evidence to guide professionals wishing to adopt a neurodiversity affirming approach in their work with Autistic clients.
What are potential weaknesses of the study?
We focused on psychology practice in Australia, and don’t know whether the model might apply to people in other countries. The model we developed may be missing aspects of care that might suit males, as none of the experts in this study was male.
How will these findings help autistic adults now or in the future?
Our findings provide a guide for what Autistic adults can expect from a psychologist who claims to offer neurodiversity affirming support. This can empower Autistic adults to find this kind of support, or advocate for the kind of support that respects and values their unique way of being.
Background
Practicing from a neurodiversity affirming framework has recently gained traction within the psychology profession. This is reflective of a broader social movement and paradigm shift toward neurodiversity, 1 where previously defined neurodevelopmental “disorders” are instead conceptualized as natural variations in cognition, perception, and processing. The neurodiversity movement is framed within the social model of disability, 2 and promotes acceptance and support across the lifespan, and creating inclusive societies to improve person-environment-fit, 3 rather than a focus on the individual needing to change. The adoption of this philosophy into clinical practice has begun in recent years, 4 yet limited research-based evidence exists to guide professionals wishing to adopt a neurodiversity affirming approach in their work with Autistic clients. 5
In response to the neurodiversity movement, in Australia 6 and elsewhere, 7 the term “neurodiversity affirming” is increasingly used in clinical settings, signaling that the practitioner provides care that does not pathologize being Autistic or otherwise neurodivergent. 8 Autistic psychologists, drawing from professional and lived experience, have been central in beginning to shape and provide affirming and inclusive care for Autistic clients (e.g., Bulluss 9 ) as have Autistic advocates (e.g., Wise 10 ). Yet currently, psychologists might indicate they provide neurodiversity affirming care with no consensus on what this practice entails. Furthermore, little is known about Autistic clients’ perspectives on the type of care they find affirming. As a result, there is limited accountability for practitioners, and limited transparency for clients. Our aim was to use the Delphi methodology to define neurodiversity affirming support in the context of psychologists working with Autistic adult clients in Australia.
Autistic adults and mental health care: Why a change in practice is needed
Autistic adults have increased vulnerability to trauma, 11 and experience a high prevalence of anxiety, depression, and other co-occurring mental health conditions. 12 Furthermore, they experience reduced life expectancy linked to high rates of suicide and physical health concerns.13,14 While Autistic adults use mental health services at higher rates than non-autistic adults,15,16 they have reported dissatisfaction with the care they receive.17-19 When seeking psychological therapy and support, Autistic adults have reported challenges being understood by clinicians, feeling clinicians often have stereotyped and inaccurate views of autism, and that services developed around neurotypical norms are inappropriate for them. 18 In contrast, when psychological therapy is attuned to the needs of Autistic adults, there is potential for a supportive therapeutic relationship to develop. 20
Much of the research considering mental health support for Autistic clients has emphasized application or adaptation of mainstream therapeutic approaches. For example, schema therapy, cognitive behavioral therapy, dialectical behavior therapy, and mindfulness have been used with Autistic adults with mixed outcomes.21,22 Some aspects of treatment-as-usual meet the needs of Autistic clients, yet often adaptations (e.g., offering sensory adjustments, providing predictability) are required for accessibility. 18 However, adaptations to the content of a therapeutic approach without addressing the therapeutic process risks being ineffective and potentially harmful for Autistic clients. 23 This may be particularly the case if there is stigma or ableism on the part of the clinician, which can undermine genuine collaboration with the client. 24 Rather than only focusing on how to adapt specific therapeutic modalities, the concept of neurodiversity affirming practice seems to emphasize a fundamental cultural shift in how therapy is delivered and provided.
As argued by Lai, 25 providing care that integrates principles of the neurodiversity movement is consistent with current best psychological practice, reflecting concepts such as humanistic psychology, person-centered therapy, and the bio-psycho-social framework. Despite this compatibility with core aspects of psychology practice, there continues to be a mismatch between the service needs of, and care provided to, Autistic adults.17,26 Furthermore, health professionals have reported barriers to supporting Autistic clients, including lacking competence and confidence. 27 There is potential for positive client and practitioner outcomes from further training and guidance for psychologists adapting their practice for this population group, and this aligns with Autistic adults’ views that better tailored services are required for them. 17 Currently, there is no research-based evidence to guide psychologists or the organizations in which they work, in making such adaptations.
Neurodiversity affirming psychology practice for Autistic adult clients
The concept of providing neurodiversity affirming support has permeated national guidelines in Australia. For example, the National Autism Strategy 2025–2031, 28 the National Roadmap to Improve the Health and Mental Health of Autistic People 2025–2035, 29 and the National Guideline for the Assessment and Diagnosis of Autism in Australia 6 have recognized the importance of neurodiversity affirming approaches to support that are specific to Autistic people. Furthermore, recently updated national competencies for psychologists 30 highlight the expectation for psychologists to understand neurodiversity and to adapt their practice to provide strengths-based and appropriate support for clients with developmental disability. Yet these documents do not define neurodiversity affirming psychology practice, reflecting the lack of current research literature.
To date, neurodiversity affirming approaches have been described in perspective pieces where aspects of neurodiversity affirming practice5,31 and neurodivergence informed therapy 32 have been proposed. McGreevy et al. 33 draw on Todres et al.’s 34 conceptual framework for humanizing healthcare as a neurodiversity affirming approach for Autistic children and young people, and Naylor 35 explored the concept of neurodiversity affirming practice broadly, although this was not specific to psychologists. Given their essential role in the provision of mental health services, it is crucial that the principles of a neurodiversity affirming approach for psychologists are defined. To our knowledge there is no published research defining the principles of neurodiversity affirming practice for psychologists. This lack of definition of neurodiversity affirming psychology practice leads to three main problems as follows: (1) psychologists lack guidance on the practical steps they can take to offer neurodiversity affirming support, (2) there is no consistency in how the term is applied, and (3) there is no framework from which to establish an empirical evidence base.
The current study
Given the potential for neurodiversity affirming psychology practice to positively impact Autistic people, and the potential problems associated with the term being used without clarification, an empirically informed model is needed to provide practical guidance for psychologists and clients seeking affirming support. Our aim was to define neurodiversity affirming support within the context of psychologists working with Autistic adult clients in Australia and to develop a model to outline what neurodiversity affirming support would involve in practice. We acknowledge that neurodiversity affirming practice extends beyond autism and the profession of psychology. However, as there is a clear need for better mental health support for Autistic people, 26 and psychologists are at the forefront of mental health service delivery, we focused on these groups.
Autistic people are experts in their own experience; therefore, incorporating Autistic voices is paramount to understanding what works in therapeutic settings for Autistic clients. 36 Furthermore, psychologists already developing and implementing neurodiversity affirming practice bring expertise based on their clinical experience. As such, we used the Delphi methodology to define neurodiversity affirming practice for psychologists, informed by professional and lived experience experts.
Methods
Study design
We used a classical Delphi design (see Keeney et al. 37 ) with three rounds. Initially, expert panel members responded to open-ended questions. We used reflexive thematic analysis 38 to develop items that were presented in subsequent rounds for consensus. Each round involved an online survey using REDCap39,40 hosted at La Trobe University. We chose the Delphi technique given the limited research on neurodiversity affirming psychology practice, and as it is appropriate when assessing questions that can inform professional practice, and when community input is important. 41
Expert panelists
We sought two groups of expert panelists: (a) Autistic adults who had seen a psychologist for therapy/support as an adult, and (b) psychologists (Autistic and non-autistic) registered with Australia’s governing body (Australian Health Practitioner Regulation Agency; AHPRA) for at least 2 years who believed they have provided neurodiversity affirming support to Autistic adult clients. We welcomed involvement from people who met both sets of criteria. All panelists were 18 years or older, living in Australia, and proficient in English. Considering barriers to autism diagnosis in Australia,42,43 Autistic panelists were not required to have been formally identified by a clinician and could self-identify as Autistic (see English et al. 44 ). Autistic panelists were not required to have experienced neurodiversity affirming support, given this type of support is new, not yet clearly defined, nor widely accessible (e.g., Brede et al. 18 )
Recruitment took place in August and September 2022 via social media (e.g., professional X/Twitter accounts of the research team, Facebook interest groups) and email invitations sent to psychologists in Australia whose online profile included “neurodiversity affirming” or similar phrases (e.g., “neuroaffirming”). Interested individuals (n = 33) completed an online expression of interest form. Study leads (R.L.F. and R.J.) reviewed responses, and determined that 31 respondents met the inclusion criteria, spanned a range of locations across Australia, had a range of years of experience (if psychologists), and were balanced in representing client and psychologist perspectives.
We invited 31 individuals to participate, of whom 28 responded. The Delphi panel consisted of 28 experts, aged 24–76 years (M = 37.29, SD = 11.74), who met the inclusion criteria for the Autistic adult group, the psychologist group, or both groups. a Autistic psychologists made up the largest group, followed by Autistic adults, while the non-autistic psychologist group had the lowest representation. All three groups were comparable in age. Of the panel members who were Autistic, 84% had received a formal diagnosis, and 26% self-identified as Autistic. Panelists represented a range of gender identities, including female (68%), non-binary, nonbinary/genderqueer, agender, gender fluid, nonbinary transmasculine, and between female and no gender. All panelists had completed higher education (21% undergraduate, 79% postgraduate). Experts resided in different states and territories across Australia, including the Australian Capital Territory, New South Wales, Northern Territory, Queensland, South Australia, Victoria, and Western Australia. Most (71%) resided in major cities, with the remainder in inner or outer regional Australia. Most panel members (78%) reported their ethnicity as Australian, Caucasian, Anglo-Celtic, or White. Remaining panelists reported their ethnicity as Aboriginal Australian, African American, Asian, or Eastern European/Australian.
Procedure
We received ethics approval from the La Trobe University Human Research Ethics Committee (HREC), with reciprocal approval from the Swinburne University HREC. The study involved three rounds (Fig. 1). In each round, we emailed panelists a unique link to the online survey, which they could complete in one sitting or over multiple occasions. Panelists remained anonymous to one another during the study. Communication with panelists was managed by a member of the research team (research assistant; R.B.) who was unfamiliar with any of the panel members to prevent any possible bias (per Jünger et al. 46 ). We reimbursed panelists with an AUD 40 voucher following each round.
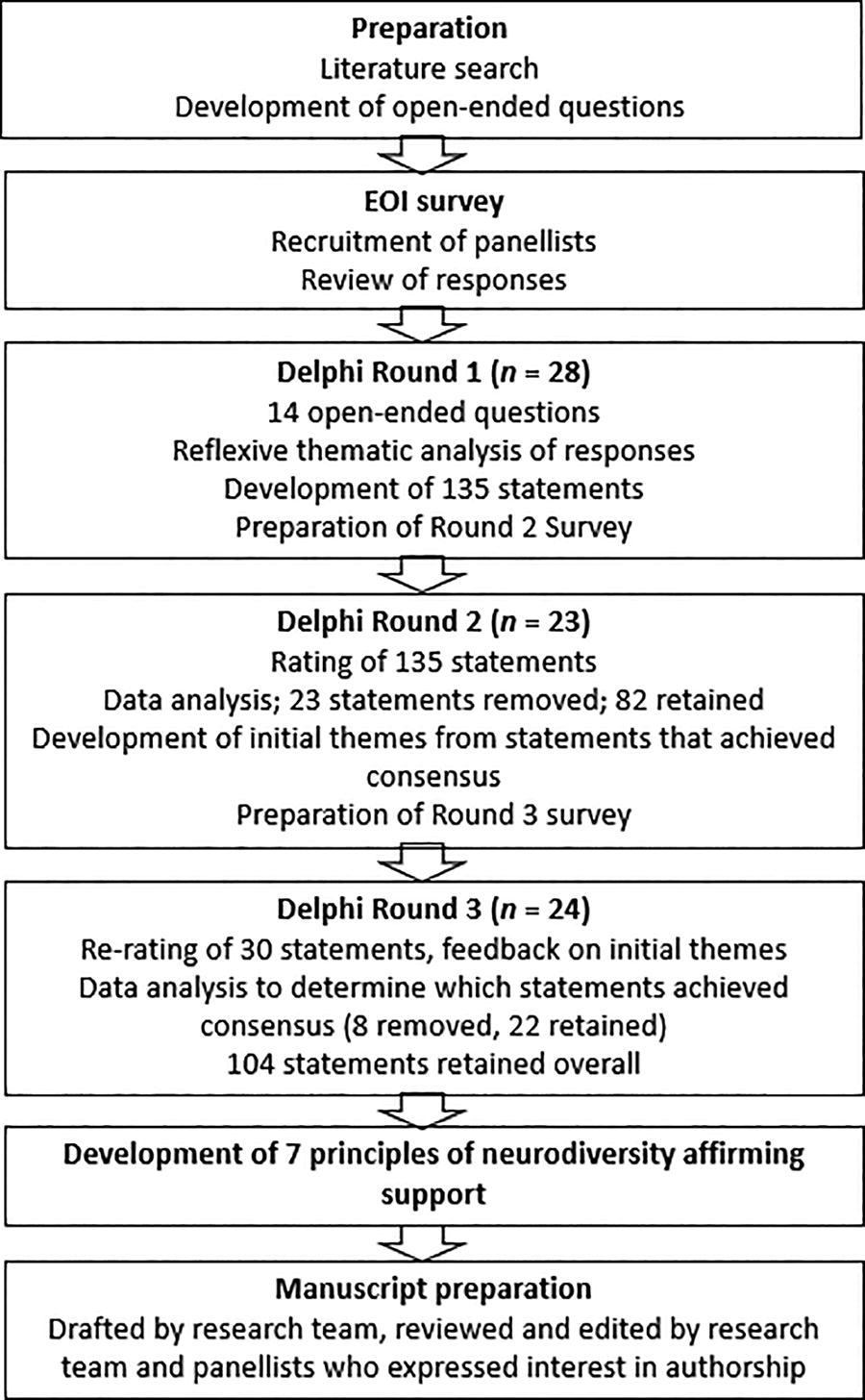
Stages of the Delphi process.
Round 1
Round 1 Data Collection
To our knowledge, there was no academic literature available regarding neurodiversity affirming psychological support at the time (July 2022). As such, we developed a set of 14 open-ended questions following discussion as a group of neurodiverse team members (R.L.F., R.J., R.B., and S.B.), three of whom are registered in Australia as clinical or provisional psychologists. Two Autistic psychologists on the research team (J.M. and M.C.), and one Autistic advisor (reimbursed for their time) then reviewed the questions. Following feedback, we decided to use the same set of questions for all expert panelists. We sent the Round 1 survey (Supplementary Data S1) to panelists in September 2022. Panelists entered demographic information (e.g., age, gender, ethnicity) before responding to the 14 open-ended questions (e.g., “In your view, what are the essential aspects of neurodiversity affirming support?”).
Round 1 Data Analysis
We used reflexive thematic analysis 38 to make sense of the Round 1 data. This approach enabled us to reflect and recognize our perspectives as individuals (e.g., lived experience, values) and as a research team (e.g., neurodiversity paradigm view of autism), and how this may impact the way in which we interpret the data. This method also allows for each response to be treated as important. Two neurodivergent (although non-autistic) team members (R.L.F. and R.B.) led the analysis of Round 1 data. While having one coder is standard practice in reflexive thematic analysis, we chose to have two primary coders for these data to improve the depth of understanding of the responses (per Braun & Clarke 38 ).
Coding took place over a 10-week period. Coders (R.L.F. and R.B.) worked both independently (coding, journaling) and collaboratively (meeting to discuss our thoughts about the data as our understanding of the data evolved) and engaged in further discussion with a third team member (R.J.). To align with the Delphi method and research aim, codes were phrased as statements about what neurodiversity affirming support involved (e.g., “The psychologist has a commitment to ongoing learning about autism”). While reflexive thematic analysis involves developing codes from the researchers’ interpretation of the data, we wanted to ensure that the voices of the panelists were central. Therefore, once codes had been developed, where possible, the statement representing each code was formed from words panelists had used. For example, we coded the statement “I think that psychologists that relate to their clients as real people, not some case study, will be more affirming for Autistic people” as “The psychologist is relatable” and presented this code as the statement “The psychologist relates to their clients as real people” in Round 2.
When we had developed the final set of codes, we sent the research team a document listing each code with a description of the meaning, example quotes from panel members, and the statement representing the code that we intended to present to panelists in Round 2. Following discussion we removed three overlapping codes. This resulted in 135 codes, written as statements.
Round 2
Round 2 Data Collection
We sent the Round 2 survey (Supplementary Data S2) to the expert panelists in December 2022. In Round 2, panelists were presented with the 135 statements, alongside feedback about how we had analyzed Round 1 data. We asked panelists to rate each statement on a 9-point scale; two scale formats (importance/agreement) were required to provide appropriate response options based on how the statements were phrased. Participants were asked to rate how important 117 statements were for providing neurodiversity affirming support (1 = Not at all important; 9 = Very important), and the remaining 18 statements on agreement as to whether the statements formed part of neurodiversity affirming practice (1 = Strongly disagree; 9 = Strongly agree). Similar 9-point scales have been used for related Delphi studies.47,48
Round 2 Data Analysis
Twenty-three panelists began the Round 2 survey; n = 22 (79%) completed it. We analyzed all collected data. Prior to data collection, we established (per Cox et al. 49 ) that items rated between 7 (Important; Agree) and 9 (Very important; Strongly agree) by at least 80% of panelists would be retained (having reached our definition of “consensus”). Items rated between 7 (Important; Agree) and 9 (Very important; Strongly agree) by 70%–79% of panelists would be included in Round 3 for re-rating, and those rated between 7 (Important; Agree) and 9 (Very important; Strongly Agree) by less than 70% would be removed from the model of neurodiversity affirming support.
The majority (82; 61%) of the 135 statements were retained, 30 b required re-rating (22%), and 23 (17%) were removed. See Supplementary Data S3 for responses. From the 82 statements that achieved consensus and were retained, the first author (R.L.F.) generated a set of initial themes. This involved organizing the statements into clusters that were interpreted as sharing an underlying meaning, and then determining the initial theme name and the meaning of the initial theme. The two study leads (R.L.F. and R.J.) discussed and further developed these initial themes, and then sent them to the research team for feedback. Minor wording changes were made for clarity; content did not change.
Round 3
Round 3 Data Collection
We sent the Round 3 survey (Supplementary Data S4) to the expert panelists in June 2023. In Round 3, panelists were presented with the 30 statements that required re-rating. We provided panelists feedback from Round 2, including the percentage of panel members who had rated each statement as 7 (Important; Agree) or higher, and their personal prior rating of the statement. We also presented panelists with the initial themes, with the option to provide feedback. Lastly, we asked panelists whether they wished to be acknowledged for their input in the article and invited them to be co-authors.
Round 3 Data Analysis
Twenty-four panelists (86%) completed the Round 3 survey. Consensus was achieved for 22 of the 30 statements (73%); the remaining eight statements (27%) were removed. Two of the eight statements were removed as less than 70% of panelists rated their importance/agreement as 7 or above. The six remaining statements did not achieve our criteria for consensus, as only 70%–79% of panelists rated these items as 7 or above, whereas at least 80% was required to achieve consensus. We decided to remove these items from the model. This resulted in 104 total statements that achieved consensus as forming the definition of neurodiversity affirming support (Supplementary Data S5).
Eighteen panelists provided feedback on the initial themes. We used this feedback on the initial themes to develop the 104 statements into seven themes that represent principles of neurodiversity affirming support in the context of psychologists working with Autistic adult clients. These are detailed in the Results section.
Panel member attrition
Eight panel members missed one or more rounds (n = 3 completed Rounds 1 and 2; n = 4 completed Rounds 1 and 3, n = 1 completed only Round 1). Of these eight, six had both professional and lived experience; one each had only lived or professional experience.
Community involvement statement
The research team is neurodiverse—comprising non-autistic, Autistic, otherwise neurodivergent, and multiply neurodivergent members. This article was authored by the research team in collaboration with 14 of the expert panelists, and the Autistic community consultant. On completion of data collection and analysis, we communicated with panelists about coauthorship, with the majority accepting and consenting to identify themselves for this purpose. These panelists contributed to editing this article, however, the results could not be altered during this process. The first six authors and the last author were members of the research team. All other authors were expert panelists and the community advisor, listed in alphabetical order.
Results
We developed seven principles (themes) that represent a model of neurodiversity affirming psychology practice in the context of psychologists working with Autistic adult clients. All 104 statements that reached consensus through the Delphi process were incorporated into the seven principles, using reflexive thematic analysis. 38 This involved discussion and consideration of underlying concepts that the statements seemed to represent. While we retained the statement phrasing within the description of principles as much as possible, slight wording changes were made to describe the meaning of principles. Similarly to Cox et al., 49 we combined some statements for clarity and to avoid repetition but ensured that all key actions within statements that reached consensus were represented. Study leads R.L.F. and R.J. facilitated the development of principles, including incorporating feedback from all research team members, over a period of approximately 8 months.
The final themes, described as principles of neurodiversity affirming psychology practice, are first shown as a model (Fig. 2), briefly outlined in Table 1, and then described in detail.
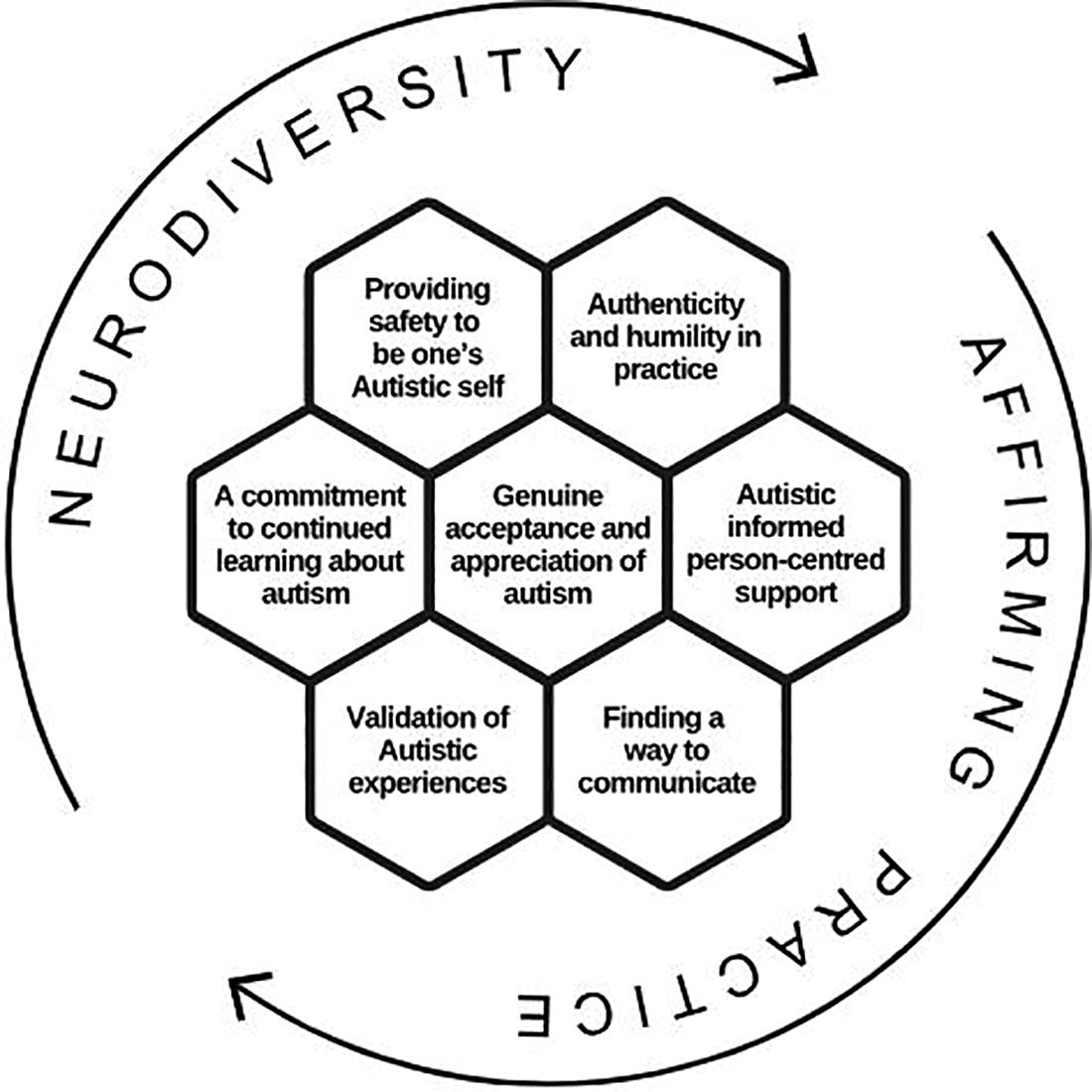
A model of neurodiversity affirming psychology practice for Autistic adult clients. Note. The figure, developed by Marie Camin, depicts the interconnected nature of the seven principles in a honeycomb, symbolic of collaboration and inspired by bees. The cyclic arrows show that the process of providing neurodiversity affirming support is nonlinear with no set starting point and involves continuously learning and adapting.
Principles of Neurodiversity Affirming Psychology Practice for Autistic Adult Clients
Working definition of neurodiversity affirming psychology practice for Autistic adult clients
In the context of psychologists working with Autistic adult clients, we define neurodiversity affirming support as follows: An approach/philosophy of psychology practice (rather than a therapeutic modality) that captures both a way of being present with clients relationally and a deep understanding of autism informed by Autistic lived experience. It focuses on providing and adapting support to align with the unique needs of each Autistic individual. This requires the psychologist to make a sincere effort to learn from Autistic people and to continue to develop this knowledge. A neurodiversity affirming approach emphasizes genuineness and common humanity, an acceptance and understanding of the way Autistic people navigate the world, as well as the humility to recognize that they might never fully understand the unique experience of each of their clients (particularly if they are non-autistic themselves). Providing safety allows Autistic people to discover, explore, and be their true Autistic self.
Principles of neurodiversity affirming psychology practice for Autistic adult clients
A commitment to continued learning about autism
This principle describes both the psychologist’s current knowledge of autism, as well as their ongoing engagement to increase their understanding and competence when working with Autistic clients. Key aspects of their understanding of autism include being trauma informed, recognizing limits to current psychological measurement tools for Autistic people, and acknowledging that standard psychotherapeutic approaches might need to be modified for their Autistic clients. Furthermore, having a sense of how Autistic people experience the world, recognizing the challenges Autistic people face, and understanding that Autistic peoples’ needs, preferences, and abilities can change both quickly and over the lifespan is also important. They are also able to guide the client in learning more about the Autistic community. Showing a commitment to continued learning means the psychologist engages in ongoing professional development, seeking to develop an understanding of Autistic culture, and prioritizing lived experience resources. This principle also requires psychologists to be reflective, knowing the extent of their autism knowledge, and showing willingness to refer on to others when this is in the client’s best interests.
Providing safety to be one’s Autistic self
A neurodiversity affirming approach may involve pacing therapy differently, allowing the client time to establish trust and safety at their individual pace—this may take longer than typically expected. Psychologists can help facilitate safety in the way the clinic space is set up, and by clarifying that the client does not need to mask or conform to non-autistic expectations in sessions. In practice, psychologists can aim to provide an environment that reduces the chance of sensory overwhelm by asking for feedback or inviting the client to make modifications based on their individual needs. They can communicate to clients that they welcome movement/stimming and provide sensory items in the therapy space. This principle involves psychologists respecting their clients as Autistic individuals, not trying to “fix” them or “reduce” Autistic traits (i.e., not promoting assimilation with the non-autistic/neuromajority), and recognizing the potential harms of masking. They use their client’s preferred language about their identity, ask about preferred pronouns, and avoid deficit-based language. If the psychologist is Autistic themselves, sharing their Autistic identity can help clients to feel comfortable. To meet this principle, psychologists need to demonstrate, through small but persistent actions, that they are listening to the client, that the environment is safe, and that it is okay and encouraged for the client to be their authentic self.
Finding a way to communicate
This principle highlights that psychologists need to recognize different communication styles of Autistic adults, proactively working to find a shared way to communicate effectively and welcoming the client’s input and guidance. This can mean understanding that some Autistic people take additional time to process information and express themselves, and some might communicate best using modalities other than speech some or all the time. They take the time to understand how each client communicates, respecting their client’s communication preferences, and they avoid making assumptions about the intent of the client’s communication. The psychologist might adapt by using clear and direct communication and incorporating visual or written mediums into their work. Finding a way to communicate includes being patient, flexible, accommodating, and willing to do things a different way (e.g., no pressure for eye contact). Engaging in this care principle also involves asking clients for feedback on what has and has not been helpful and checking in to make sure they are explaining things in a way that makes sense to their client.
Authenticity and humility in practice
This principle emphasizes that to provide neurodiversity affirming care, the psychologist needs to be genuine, caring, compassionate, nonjudgmental, and sincere in a way that fits for their clients. A sense of authenticity and humility can be facilitated by psychologists relating to their clients as fellow humans, and working to create a more equal and balanced relationship rather than portraying an overly professional persona, while working within ethical and professional boundaries. Neurodiversity affirming psychology practice involves the psychologist being actively self-reflective and open to feedback from Autistic clients, as well as willing to be wrong, which requires awareness of their own limitations. They are curious, which helps them to learn from their clients and take the time to understand the individual needs of each client. This may help the client feel more at ease when relating to and developing trust in the psychologist.
Validation of Autistic experiences
Providing neurodiversity affirming care requires the psychologist to wholeheartedly believe their client’s experiences and seek to both understand and value their client’s worldview. They view and treat Autistic clients as the experts in their own lives and validate their experiences. To do this, psychologists need to continually reevaluate and reflect upon assumptions they hold about ways individuals “should” behave or think and acknowledge the perspectives of their neurodivergent clients. By being attuned to, and getting to know their Autistic clients, psychologists can better recognize when their client is having more difficulty than usual. In neurodiversity affirming practice, psychologists demonstrate complete acceptance of their clients and approach their clients as equals.
Autistic informed person-centered support
Neurodiversity affirming practice involves being person-centered, collaborative, and led by the client and their individual goals. There are times when the psychologist will be required to think and respond differently to how they would with non-autistic clients, to best match their client’s needs. At a basic level, outside of the session, accommodations can be made so that the psychology setting is more accessible to Autistic clients. This can be done through clear and simple booking systems, appointment reminders, consistent scheduling, advance notice of any changes, flexible modes of delivery (e.g., online), and letting the client know what to expect from their appointment. In addition to providing therapy, the psychologist might help the client understand what supports and accommodations are available to them so they can better advocate for themselves.
When working therapeutically with Autistic clients, psychologists are respectful of the client’s preferences and views of autism, yet where appropriate, integrate affirming concepts. This requires the psychologist to be flexible and adaptable, and to show curiosity about their Autistic client, rather than making assumptions about their experiences or Autistic identity. They recognize that the client’s neurotype may be, to different extents, an important element of their identity that permeates their experiences and influences how they interact with the world. Autistic-informed person-centered support involves psychologists taking the time to learn their clients’ interests, strengths, and needs, and providing individualized support based on this, focused on helping the client live their best Autistic/neurodivergent life. This may include making adaptations to different therapeutic approaches to suit the client’s needs. Neurodiversity affirming support is less about the specific support provided, and more about the psychologist’s approach and attitude toward the client.
Genuine acceptance and appreciation of autism
A genuine acceptance and appreciation of autism means that psychologists need to have a nuanced understanding and genuine acceptance of neurodiversity, neurodivergence, and autism, and how autism fits within the neurodiversity paradigm. They must also value social justice. They need to recognize the variation in the presentation of autism, and to appreciate that each person is different, with different needs. When providing neurodiversity affirming care, psychologists appreciate what it means for their client to be Autistic and acknowledge the strengths that come from being neurodivergent. They have unconditional positive regard for their clients. While this incorporates being strengths-based, the psychologist also needs to have a good understanding of concepts such as privilege, oppression, and marginalization, and the inequalities Autistic people experience as part of a minority group. Central to this principle involves psychologists recognizing that standard or usual approaches might not always be fitting or affirming for their Autistic clients, and in some cases, may be harmful or have caused harm in the past.
Discussion
Here we present a model of neurodiversity affirming practice for psychologists working with Autistic adult clients, developed in collaboration with expert panelists (Autistic people, and Autistic and non-autistic psychologists). To the best of our knowledge, this is the first empirically developed model of neurodiversity affirming psychology practice, informed by lived-experience expertise. The principles of the model reflect that neurodiversity affirming psychology practice is a philosophy or approach to care rather than any one particular therapeutic modality (consistent with Chapman & Botha 32 ; Lerner et al. 31 ; Naylor 35 ) and is something that may require a “fundamental mindshift” from clinicians 50 to make psychology services more accessible.
We view the seven principles of neurodiversity affirming psychology practice as interconnected, whereby all are required to provide neurodiversity affirming support. Engaging in some principles without others (e.g., being knowledgeable about autism without taking steps to help a client feel safe to be their authentic Autistic self) risks undermining genuinely neurodiversity affirming care. We do not view the model as linear, meaning for psychologists wishing to learn from and apply the model, there is no specific “starting” point; all principles involve ongoing learning, adaptation, and reflection, which are core aspects of psychology practice. 30
We recognize the uniquely valuable position of Autistic psychologists in providing professional and lived-experience informed training and supervision. However, we are mindful of the potential burdens minority groups face when solely responsible for the education of others (as described in the “minority tax” in academia 51 ). To embed this model in practice, our data suggest that coming from a stance of genuine acceptance and having a nuanced understanding of the neurodiversity paradigm based on ongoing learning are essential. Application of this model may contribute to improving an unmet mental health care need (see Andoni et al. 17 ) by guiding psychologists in tailoring their work to Autistic adults.
More than standard good practice
Some components of the model of neurodiversity affirming practice appear to align with the general standards of psychology practice and to fit within expected core competencies for psychologists. However, the model adds elements that are specific to working with adult Autistic clients, and emphasizes that aspects of therapeutic practice that are encouraged as part of best practice, such as authenticity, are necessary but not sufficient when working with Autistic clients. To illustrate, all clients should feel safe to be themselves when attending therapy, which is emphasized within trauma-informed approaches (see Bendall et al. 52 ). However, based on our findings, without psychologists demonstrating awareness of experiences such as masking, and acceptance of different ways of self-regulating, Autistic clients may have more difficulty feeling safe to be themselves. Furthermore, the experience of attending therapy for adult Autistic clients may be too overwhelming to engage in meaningfully if psychologists do not have an understanding of common sensory sensitivities, differences in thinking, communicating, and perceiving social interactions, and if they do not ask clients about their needs and preferences. Some nonverbal behaviors traditionally viewed as creating interpersonal safety (e.g., prolonged eye contact) may feel threatening for Autistic clients. Therefore, working to facilitate a sense of psychological and physical safety for Autistic clients is multifaceted and requires psychologists to be well informed, and extends beyond practice as usual. While it may not be possible for some people to feel completely at ease, psychologists can aim for creating a space where clients feel safe enough to engage in therapy.
It is noteworthy that our expert panel generated and recommended the inclusion of aspects of standard care (e.g., being nonjudgmental, self-reflective, and person-centered) in the model of neurodiversity affirming psychology practice. The need to make these explicit in the model is perhaps reflective of Autistic adults reporting negative experiences when interacting with healthcare professionals.18,19 This is possibly reflective of a medical model or ableist view that contributes to stigma and reduced autonomy (see Sonuga-Barke 53 ). Or, perhaps implementing best practice principles such as client-centeredness looks different to how psychologists expect when working with Autistic clients. Without engaging in further training, psychologists might not recognize or have a framework for understanding their clients’ needs and preferences, so their approach becomes misaligned; something that could be amplified when they are not aware their client is Autistic (and clients might not feel comfortable sharing that they are Autistic 54 ). Additional consideration is needed if the Autistic client is also multiply neurodivergent. A neurodiversity affirming approach therefore needs to integrate best practice with humility and autism informed support to go beyond standard care to meet the needs of Autistic clients. This builds upon Lai’s 25 recent suggestion that mental health supports for Autistic clients do follow standard care but must be clearly informed by the neurodiversity paradigm.
There are aspects of the model that suggest current standards of ethical and professional practice in psychology might differ through the neurodiversity affirming lens. In particular, and consistent with past research, 20 our panelists highlighted the potential value of the psychologist self-disclosing their own neurodivergence, presenting a less professional persona, and suggested that standard therapeutic approaches might need to be modified for Autistic clients. It seems important to explore this further, to understand why such expressions of authenticity and genuineness—that might contrast with traditional beliefs and recommendations/practices around the psychologist–client relationship—are so important and meaningful to Autistic adults. Furthermore, this softening of traditional role definitions and approach to relating to Autistic clients may present an exciting opportunity for a more affirming, positive, and potentially destigmatizing therapy experience. 53
Developing an evidence base
We acknowledge that Autistic advocates and psychologists have been sharing information about neurodiversity affirming psychology practice for some time. The model we have developed is aligned with suggestions from other researchers. For example, Chapman and Botha 32 argue that clinicians viewing cognitive or communicative dysfunction as relational rather than an individual/intrinsic flaw of the neurodivergent person is a key component of neurodivergence-informed therapy. This requires actions we note as important, such as a nuanced understanding of autism. It also requires psychologists to recognize their role in developing a therapeutic rapport, and finding a shared way to communicate with each client. Other nonempirical work has also highlighted key components that align with the principles of validating Autistic experiences, using Autistic centered, person-centered support, and displaying a genuine appreciation of autism in designing frameworks for neurodiversity affirming interventions. 31 When synthesizing lived-experience perspectives on mental health care, Andoni et al. 17 indicated that Autistic clients are asking for a more tailored approach, practitioners with humility and understanding of autism, and adaptations and accommodations to therapies, suggesting the model we have developed is consistent with these unmet needs.
Our model is also aligned with existing research exploring neurodiversity affirming practices outside of psychology. Dallman and colleagues 55 discuss neurodiversity affirming occupational therapy as involving considering whether standard treatment and (neuronormative) goals might risk reducing elements of a person’s Autistic identity. This aligns with the principle of Autistic informed person-centered support, and the notion that support should assist clients in living their best Autistic life. Shaw and colleagues 56 discuss the fundamental importance of psychiatrists using nonpathologizing language. We agree and our principles include actions such as avoiding deficit-based language, and using the client’s correct pronouns, and preferred language about their identity. Naylor 35 developed a nonprofession-specific definition of neurodiversity affirming practice, reported in their doctoral thesis. They too describe neurodiversity affirming practice as being beyond any specific type of support, stating it involves a “philosophy of practice” (p.62). Similar to the model we developed, they describe universal factors, such as the importance of accepting the client as they are, client-centered support, and the client feeling safe. McGreevy et al. 33 discuss the conceptual framework for humanizing care 34 as a neurodiversity affirming health care approach for Autistic young people. This framework emphasizes the importance of agency (relating to our principle of Autistic informed person-centered support), and insiderness, prioritizing lived experience above preconceived and neuronormative ideas (relating to our principle around validating Autistic experiences).
At this point in time, there is a need to develop the evidence base to support clinical observations that neurodiversity affirming support leads to a better experience for Autistic clients. This model helps create a foundation upon which an evidence base can be built. Aspects of the model suggest ways in which adhering to a neurodiversity affirming approach to practice may facilitate better therapeutic outcomes for Autistic clients. For example, the relational aspects of the model reflecting shared ways to communicate, and authenticity and humility may support greater therapeutic alliance, often identified as a key factor underpinning therapeutic success across therapeutic modalities. 57 Ultimately, the current research is an initial first step in our goal of determining and informing how psychologists can best support Autistic clients to achieve their goals, improve the efficacy of mental health services for this community, and reduce the burden of mental health concerns.
Limitations
Given the parameters of the study design, specifically the focus on Autistic adult clients, and psychology practice within Australia, we do not know whether and how this model might apply in other countries or cultures. By solely focusing on autism at the exclusion of other neurodivergent identities, we generated rich data related to affirming practice for this group, but were not able to consider other neurotypes, psychology practice for those who are multiply neurodivergent, or other intersecting minority identities that might have different needs in a psychology setting. Furthermore, the model may not represent aspects of care that would best suit Autistic males, given there were no male expert panelists. In addition, all panelists had completed higher education, and thus, the study does not reflect the voices of Autistic people without university education. Lastly, given the same panelists generated content and completed consensus ratings, it is possible there are additional aspects involved in neurodiversity affirming care not captured here (i.e., what was generated was limited to the views of those involved in the study). However, given the limited published information about neurodiversity affirming practice, it was not possible to conduct the Delphi process with a literature search. Furthermore, we feel the expert panelists represent a wide range of skill, with a strength of this research being the professional and lived experience expertise of panel members.
The National Roadmap to Improve the Health and Mental Health of Autistic People 2025-203529 introduces the term “autism affirming care.” While we acknowledge the importance of specific terminology, the aim of this research was to define “neurodiversity affirming support” within the context of psychologists working with Autistic adult clients in Australia, and our research materials reflected this aim. As such, we use this term to remain true to the research process.
Conclusion
To our knowledge, we have developed the first empirically informed model of neurodiversity affirming practice for psychologists. Further research is needed to explore the utility of this model for both psychologists and clients, and to determine whether implementation of these principles supports an improved therapeutic experience for Autistic clients and potentially clients more broadly. We encourage psychologists working with Autistic clients to consider how the model presented could be incorporated into their practice, as a step toward promoting inclusivity in the psychology profession during this period of change.
Footnotes
Acknowledgments
The authors acknowledge the input from the following expert panel members: Dr. Erin Bulluss, Dr. Bianca Calabria, Mrs. Amanda Curran, Mel Giugni, Mrs. Victoria Gottliebsen, Haylea Hodges, Catherine Lamont, Dr. Joanne Lawrence, Ms. Vivien Leung, Ms. Kathryn Miklosi, Ms. Monique Mitchelson, Carol Mumme, Alison Nuske, Carly O’Sullivan, Anne Pickett, Miss Becky Roberts, Ms. Caitlin Waldie, C. A. Watts, Stephanie B. Watts, Mx Georgia Williams, and those who chose to remain anonymous. They also thank Red Levy-Knoll for their contributions, Dr. Georgina Cox for her guidance with regard to conducting a Delphi study, and Dr. Aspasia Stacey Rabba for her encouragement, support, and for sharing her experiences as a clinician with them.
Authorship Confirmation Statement
R.L.F. and R.J. conceptualized and led the study. R.L.F., R.J., and R.B. managed project administration. R.L.F., R.J., R.B., S.B., M.C., J.M., and E.K.R. contributed to project design and reviewed documents at each stage of the project. R.L.F., R.J., and R.B. managed recruitment, data collection, and conducted all data analyses. R.L.F. and R.J. wrote the first article draft, which was reviewed by R.B., S.B., M.C., J.M., and E.K.R. R.L.F. and R.J. developed the draft following feedback, which was then reviewed by all other authors. R.L.F. and R.J. managed the process of revising the article following substantial feedback from other authors and prepared the final draft. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
The authors received a grant of $14,769 from the La Trobe University School of Psychology and Public Health to support this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.