
Abstract
Abstract
The number of morbidly obese women of childbearing age greatly increased over the last decade. These women require highly specialized care during pregnancy, especially at time of delivery, because of the potential for multiple comorbidities and the increased risk for poor outcome for themselves and their infants. Hospitals need to ensure that not only is the patient prepared for delivery, but also the hospital staff and environments are prepared.
Introduction
Thirty-eight percent of female obstetricians and gynecologists identified obesity as the primary health problem for women of childbearing age. 1 Obesity is a growing trend in the United States, evidenced by increasing obesity prevalence in recent years. In 1990, no states had a prevalence of obesity greater than or equal to 15%; but in 2008, the prevalence of obesity was > 25% in 32 states. 2 See Figure 1. This health issue is greatest in the black non-Hispanic population. 3
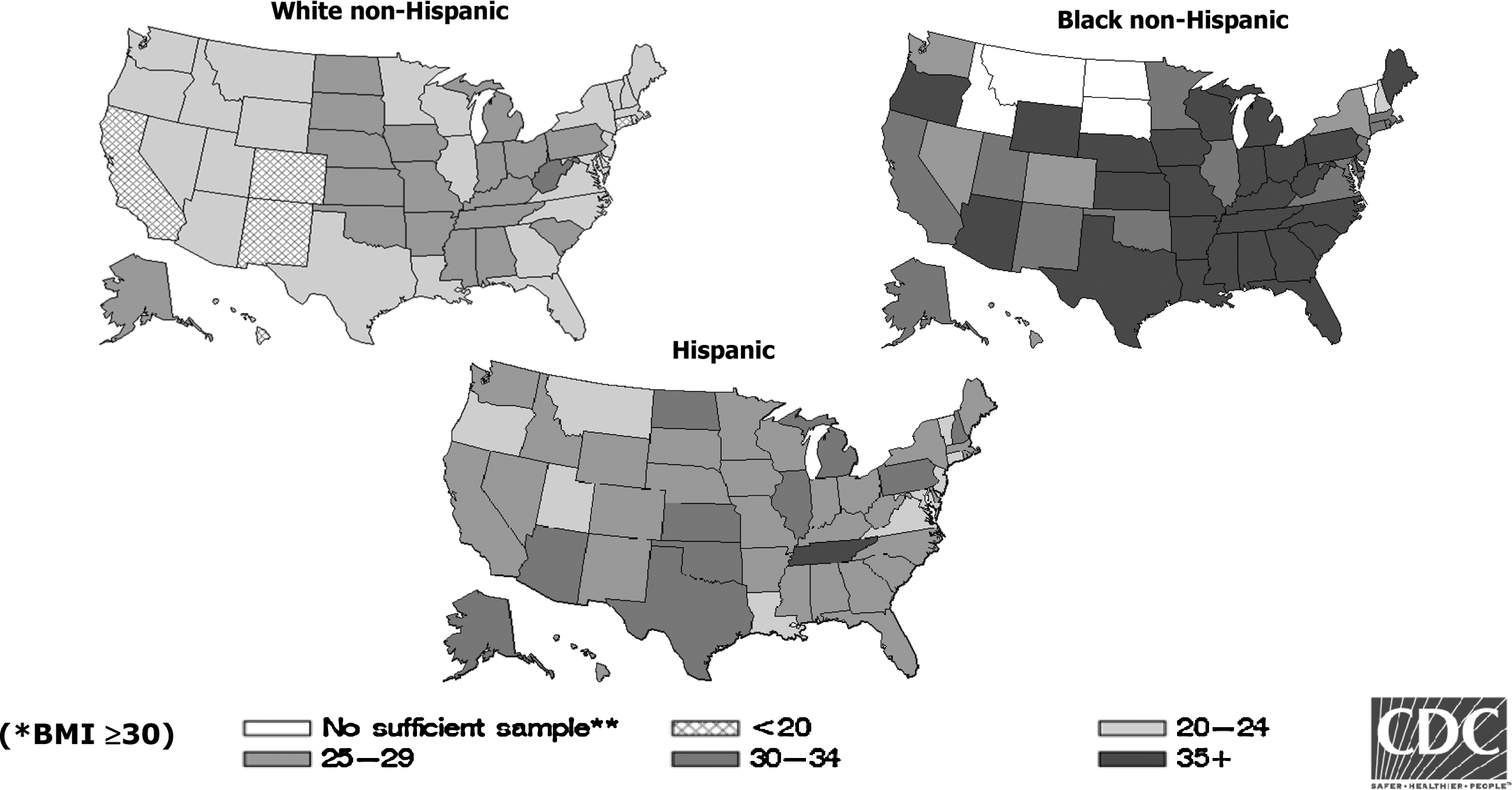
State-Specific Prevalence of Obesity* among U.S. Adults, by Race and Ethnicity, 2006–2008. Source: CDC Behavioral Risk Factor Surveillance System. 2
Impact of Obesity on Pregnancy
Obstetric complications increase with obesity, as does the risk of adverse birth outcomes. Throughout the prenatal period, obese women are at higher risk for miscarriage, preeclampsia, metabolic syndrome, hypertension, gestational diabetes, and deep vein thrombosis, not to mention the potential birth complications involved with a stillbirth, pre-term birth, or wound-healing issues.3–5
The fetus is at risk for complications including macrosomia, congenital anomalies (generally involving neural tube defects), fetal obesity, and, later, childhood obesity.3,5
What is the role of the healthcare provider in managing this growing trend of obesity in women of childbearing age? Women contemplating pregnancy should be informed of the potential effects of obesity on conception, overall health status, and the health of her fetus or newborn. Some recommend that women should achieve a normal BMI (less than 18.5–24.9) before conception. 5 Syin and colleagues investigated pregnancy outcomes after bariatric surgery and found that bariatric surgery may have a protective effect on maternal and neonatal outcome, provided that vitamin deficiencies are avoided and nutritional needs are met. 6 Further research is needed, however, before preconception bariatric surgery is recommended.
It is crucial for the healthcare provider to work closely with these morbidly obese women to effectively manage their pregnancies. Education related to appropriate weight gain, nutrition, and exercise options appropriate for each stage of pregnancy is needed throughout the prenatal period. Assessment of the health status of the mother and baby is essential. Procedures and tests based on each woman's situation need to be planned with special consideration to the impact of additional weight gained during pregnancy, which may affect the woman and/or her fetus. Specifically, visualization of the fetus via a sonogram must be well planned as picture clarity diminishes with further weight gain. 7
Case Presentation
A 34-year-old African American non-Hispanic woman, Gravida 1, Para 0 with a BMI of 83 was referred to a tertiary Level IIIC perinatal center for management of her high-risk pregnancy related to her obesity. The patient had received early prenatal care from her primary gynecologist, who then referred her to an obstetrician at 12 weeks gestation. At 25 weeks gestation, the patient was referred to an anesthesiologist for a consultation about the need for anesthesia during delivery. The anesthesiologist recommended the patient be transferred because he felt his hospital and the delivery team did not have adequate bariatric resources to provide safe care to the patient and baby.
The patient presented to our labor and delivery unit for her first prenatal visit at an estimated 35 weeks gestational age. Upon this initial visit, her weight was 577 pounds with a height of 5 feet, 9 inches and a BMI of 83. Routine prenatal labs and cultures were obtained (see Table 1). At approximately 28 weeks gestation, she was diagnosed as a Class A2 gestational diabetic (see Table 2) based on hemoglobin A1C of 7.7 (%) and as a result was placed on insulin. Upon her initial presentation in L&D, during which her home-monitored blood glucose levels were reviewed, it was apparent that her glucose levels had been inadequately controlled. Thus, her insulin dosages were substantially increased. The patient's past medical history included asthma for which she was not taking any medications. The patient stated that she had not had an attack in the last 5 years, but did have a history of one hospitalization in 2003 with an attack requiring no intubation or steroids. Past surgical history included a tonsillectomy as a child and left knee arthroscopic surgery at age 16. The patient denied any history of alcohol, tobacco, or street drug use. The patient was employed as a high school English teacher and was enrolled in a doctoral program. The patient was not married, and the father of the child was minimally involved. She had an extensive support system of family and friends.
Source: Modified from White P. Pregnancy complicating diabetes. Am J Med 1949;7:609; and Landon MB, Catalano PM, Gabbe SG. Diabetes mellitus. In Gabbe SG, Niebyl JR, Simpson JL, Obstetrics: Normal and Problem Pregnancies, 4th ed. New York: Churchill Livingstone, 2002.
At this prenatal visit, the patient was seen by the obstetric anesthesiologist. He discussed with her the types of anesthesia that could be used and the risks involved with each. It was conveyed to her that a regional anesthetic would be the first and safest form of anesthesia for delivery. It was anticipated that epidural or spinal anesthesia might not be possible since she did not have any palpable landmarks on her spine. In that case, an awake fiber-optic intubation would be used for anesthesia. She was also counseled that in an emergency, regional anesthesia would not be an option. The patient fully understood the possible plans for anesthesia care and the associated risks as outlined, and agreed to the proposed plan of care.
An ultrasound revealed that the infant was in the breech presentation. Based on this presentation in addition to her size, the team concluded that a vaginal delivery was not possible. A cesarean section was scheduled for 39 weeks gestation, approximately 4 weeks later. A multidisciplinary case conference was convened and attended by the maternal fetal medicine physician overseeing the patient's care, an obstetric anesthesiologist, a representative of the medical intensive care unit, a nurse from L&D, the nurse manager, and the clinical nurse specialist. At this case conference, a plan of care was developed and subsequently placed in the patient's chart in the event that she presented early, either in labor or with other complications.
The patient was scheduled for her next prenatal visit at the high-risk obstetric clinic 2 weeks later. Her fasting blood sugars over those 2 weeks were 120–130 mg/dL after meals, with bedtime blood sugars running 130 to 150 mg/dL. On the day of her scheduled visit, an ultrasound scan of the fetus placed the infant in the 90th percentile for growth with an estimated fetal weight of 3739 grams (8 pounds 3.88 ounces). On ultrasound visualization, the infant was also noted to have subcutaneous fat visible under the scalp, indicative of fetal macrosomia or a large-for-gestational-age infant. When the patient arrived for her prenatal visit, she stated for the last 24 hours she had been having contractions approximately every 5 minutes. She was emergently referred to the Labor and Delivery unit for further evaluation.
She was immediately placed on the external fetal monitor to allow for evaluation of fetal heart rate and uterine contractions. Her uterine contractions occurred about every 2 to 5 minutes and were mild to palpation. The fetal heart rate was reassuring with a heart rate of 150 beats per minute, moderate variability, with accelerations of the fetal heart rate and no decelerations present. A vaginal exam, noted to be technically difficult because of her body habitus, revealed her cervix was closed and firm. Because she was experiencing contractions, the healthcare team agreed it was necessary to monitor both the contractions and fetal movement. This required that the patient be admitted with plans for a scheduled cesarean section. The patient was started on nifedipine 20 mg every six hours for tocolysis (prevention of uterine contractions and labor). A peripherally inserted central catheter was placed in her left arm for intravenous (IV) access. Her management plan also included tight glycemic control with insulin to prevent neonatal hypoglycemia in the immediate post-delivery period. She was placed on an American Diabetic Association (ADA) diet. The controlled diet and her insulin regimen improved her blood glucose levels as measured by fingerstick.
The patient's condition remained stable over the next 2 days, except for some mildly elevated blood pressures (systolic blood pressures of 140–160 mmHg; diastolic blood pressures of 70–80 mm Hg) and slightly increased liver function tests (AST and ALT of 50 and 39 units/L). As a result of these diagnostic criteria, she was diagnosed as having mild preeclampsia. The healthcare providers decided that her blood pressure did not require active treatment, but continuous observation was still necessary. The nursing care plan included assessing her blood pressure, laboratory values, and other symptoms associated with preeclampsia.
As discussed during the case conference, the identified necessary bariatric equipment and supplies were obtained and available for use with this patient. They were all kept in one location in L&D until admission. Once the plan of care for the admission was verified, the equipment and supplies not already in use for the patient were relocated to appropriate areas in L&D and the inpatient perinatal unit. The nursing staff were aware of the location and use of this specialized equipment.
As planned, the patient had a cesarean section two days later. Prior to moving the patient to the operating room (OR), an arterial line was placed in her right radial artery and a continuous spinal epidural was inserted under ultrasound guidance without difficulty using an 18-gauge 5-inch needle. The patient was transferred to the OR on her bariatric bed and placed on a bariatric OR table. She was placed in the dorsal recumbent position with a left tilt and a modified semi-Fowler's position in order to facilitate ventilation and to prevent veno-caval compression syndrome that could occur as a result of the large uterus compressing the vena cava and aorta. A c-section skin incision was made using a midline vertical supraumbilical incision followed by a classical (vertical) uterine incision. The c-section proceeded in a usual fashion. The only issue that occurred during her surgery was a brief period of systolic hypotension (110 mm Hg), which was treated with two doses of ephedrine. The patient's estimated blood loss was 1500 ml. Intraoperative fluid resuscitation included 2000 ml of crystalloids and 1000 ml of Hespan. Her urine output during the surgery was adequate. She tolerated the procedure remarkably well and was taken back to L&D for post-anesthesia recovery and an overnight stay for close observation.
The patient delivered a live male infant, with Apgars scores of 9 at 1 minute and 9 at 5 minutes and a weight of 3700 grams (8 pounds 1.5 ounces). Umbilical cord gases were within normal limits (see Table 3). The infant was transferred to the normal nursery in stable condition, and the infant continued to do well in the newborn nursery. The patient had opted to breastfeed and was very successful in this endeavor.
Source: Normal arterial values from Garite TJ. Intrapartum Fetal Evaluation P425. In Gabbe SG, Niebyl JR, Simpson JL, Obstetrics: Normal and Problem Pregnancies, 4th ed. New York: Churchill Livingstone, 2002.
On the first post-operative day, her patient-controlled analgesia was discontinued and she was placed on oral pain medication. She was started on Heparin 10,000 units subcutaneously three times a day for deep vein thrombosis prophylaxis, and within 24 hours this was converted to Lovenox 100 mg twice a day. Her fingerstick blood glucoses remained within normal range, and she progressed to a regular diet by the end of the first post-operative day. Physical therapy was consulted to assist with ambulation. Occupational therapy was consulted to assist with activities of daily living and infant care.
By the end of the second post-operative day, the patient was ambulating in the halls, voiding without difficulty, and eating a regular diet, and did not require intravenous access. Both the patient and the infant were discharged on the third post-operative day in stable condition with instructions to return to L&D the following week for staple removal. Post-partum follow-up was arranged. The patient was also instructed to follow up with a bariatric specialist for outpatient evaluation.
Discussion
This case study is an example of the value of holding a multidisciplinary case conference regarding patient care during pregnancy, labor, and birth, which cannot be underestimated. The members of the team should include a maternal-fetal medicine physician, an OB anesthesiologist, and nurses and physicians from the areas where the patient may be admitted (including L&D, post-partum, and the main OR). The team should consider the need for any additional tests, any consults, and any specific equipment or supplies needed prior to and post delivery. 8
Due to the extra amount of adipose tissue that the patient has, there is an increased likelihood of additional bleeding. 9 In preparation for this risk, the patient should be cross-matched for a minimum of four units of packed red blood cells, which should be immediately available if needed. Additional diagnostic modalities should be considered including electrocardiograms, echocardiograms, a sleep study, and pulmonary function tests. The need for these diagnostic procedures should be individualized based on the patient's past medical history and clinical course. It may also be necessary to test for diabetes earlier in the pregnancy rather than at the usual 28 weeks of gestation.
A consult with OB anesthesia should be conducted as early as possible in the pregnancy so that the patient is well informed of the risks and benefits of the various types of anesthesia. 10 Depending on the patient's other comorbidities (e.g., asthma, chronic hypertension, and diabetes), and the gestational age at delivery, the infant may need to be admitted to the neonatal intensive care unit (NICU). If possible, the patient should also have a neonatal consult prior to the delivery so that the patient can be aware of potential procedures and treatments that may be required. A tour of the NICU is beneficial to decrease patient stress and anxiety. Additional consults should be considered to meet the patient's individualized needs, including a nutritionist, lactation specialist, social worker, physical therapist, occupational therapist, and bariatric specialist.
One of the most significant issues in preparing for the delivery of a baby to a morbidly obese patient is ensuring that appropriate equipment and supplies are available. Bariatric beds have mattresses that are very soft and flexible. This feature does not allow for easy access for vaginal examinations or delivery. The labor beds currently on the market were not made to accommodate the severely obese woman. 10 The bariatric equipment list should include a bedside commode, a wheelchair, a stretcher, a bariatric OR table, a scale capable of weighing patients greater than 350 pounds, and long-handled abdominal instruments in the event of a c-section. Additional supplies may include extra-long spinal needles, long speculums, an extra-large blood pressure cuff, and bariatric gowns. These equipment and supplies should be obtained and stored in an easily accessible place for when the patient presents in labor or is admitted with other complications such as preeclampsia.
While this is certainly a high-risk situation, it is important that nurses remember that the patient and her family are undergoing a life-altering experience in the birth of the infant. Nurses must support the patient's decision to carry the pregnancy. As much as possible, every effort should be made to include the family and/or significant other in the planning and implementation of the patient's care. This helps to alleviate their concerns and will help the patient through this significant life event. It is important to keep in mind that morbidly obese patients are also more at risk for post-partum depression. The patient and family should receive education about the signs and symptoms of post-partum depression and what to do if these signs and symptoms develop. It is also extremely important that members of the healthcare team monitor their own behavior, actions, and verbalizations so as to not make the patient feel stigmatized because of her weight or body habitus. 11
Conclusion
With the increase in the amount of morbidly obese women who are of childbearing age, it is important that hospitals consider how well they are prepared for the delivery of a baby to a morbidly obese woman whether it is a planned or unplanned delivery. Consideration must be given to the environmental needs with significant attention to the identification of necessary bariatric equipment and supplies. It is important that staffs are knowledgeable about the location and use of the specialized equipment and supplies. Consideration must also be given to the preparation of the staff and the patient for this high-risk delivery. When possible, a case conference during the prenatal period ensures members of the healthcare team are well informed about this high-risk patient. During the conference, the team should delineate and address the unique needs of the patient and fetus or newborn at time of delivery and the post-partum period, including lab tests, consults, and monitoring needs. The support of family and friends is also essential to help the new mother meet the physical and emotional demands of her new role.
Footnotes
Disclosure Statement
No competing financial interests exist.