
Abstract

Introduction
Incidence
The latest information from the National Health and Nutrition Examination Survey (NHANES) shows that from 1971 to 2006, the incidence of obesity in preschool-aged children (2–5 years) increased from 5% to 12.4%, for school-aged children (6–11 years) the incidence increased from 6.5% to 17%, and for adolescents (12–19 years) the incidence increased from 5% to 17.6%. These figures are more than three times the 5% goal set by Healthy People 2010. 4
Medical Consequences
Children who are overweight or obese are developing disorders that were once only found in the adult population. This includes an increased risk for cardiovascular disease including high cholesterol, high blood pressure, and abnormal glucose tolerance. 5
The Bogalusa Heart study evaluated 2,617 children between the ages of 2 and 17 years. This longitudinal study examined the relationship of pediatric BMI to adult levels of lipids, insulin, and blood pressure. The participants were reexamined at ages 18 to 37 years, the mean age of follow-up being 17 years. The data demonstrated that of the children who had a BMI in the 95th percentile in childhood, 77% had remained obese as adults. 6
Other health risks include asthma, non-alcoholic fatty liver disease (NAFLD), sleep apnea, type 2 diabetes mellitus, and psychosocial risks. 7 Obese children may also develop gallbladder disease, kidney disease, orthopedic problems, and polycystic ovarian syndrome. 8
With the increase in obesity, the incidence in type 2 diabetes mellitus (T2DM) has increased as well. T2DM accounts for 20 percent of diabetes in children aged 10–19 years of age. In addition, the rate of metabolic syndrome is nearly 50 percent in adolescents with a BMI of greater than 40. 8
Sleep apnea has serious consequences for growth and development. 9 Disturbing the normal sleep process interferes with normal physiologic processes. Children with sleep apnea were found to have poorer neurocognitive testing scores compared to obese children who did not have sleep apnea. 10 There is a correlation between obstructive sleep apnea and increased fasting insulin levels. Obesity combined with obstructive sleep apnea may lead to an even higher elevation of insulin levels. 11
Gallstones have been found in 2% of children with a BMI of greater than 30, compared to 0.6 percent in non-obese children.12,13 Non-alcoholic fatty liver disease (NAFLD) is a serious complication of pediatric obesity. Children with NAFLD are at risk for liver damage, including cirrhosis.12,13 In addition, morbidly obese children have been diagnosed with focal segmental glomerularsclerosis. If untreated, this disorder can progress to end-stage renal disease; however, it will remit with weight loss. 8
Orthopedic problems associated with childhood obesity include slipped capital femoral epiphysis, genu valga, Blount's disease, flat knee cap pressure or pain, flat foot, low back pain, scoliosis, and arthritis. 8
Psychosocial Problems
In addition to physical problems, being overweight or obese contributes to negative consequences of the psychosocial well-being of children. Quality of life scores are decreased. Obese children and adolescents experience poor body image, decreased self-esteem, depression, poor school performance, and exercise avoidance. Bullying and bias/discrimination occur both in school and in the community. Social exclusion not only alienates children but also eliminates opportunities for increased physical activity and increases sedentary time at home, where maladaptive eating habits are reinforced.14,15 Another social consequence of pediatric obesity is discrimination from their peers. 16 Discrimination from healthcare workers has also been reported. 17
Financial Implications
As a result of the increased medical needs of these patients, the financial impact on the healthcare system has been significant. Since 1979, in the 6- to 17-year-old age group, obesity related hospital costs have tripled. In 1979, obesity-related hospital costs were $35 million. In 2005, these costs increased to $14 billion. 18 Unfortunately there is little literature describing the cost of outpatient treatment for the pediatric overweight and obese population. Hampl and colleagues reported that as there are many children who are undiagnosed as overweight or obese, the economic impact of this problem is underestimated and overweight and obese children have increased healthcare expenditures similar to their adult counterparts. 19
Causes and Risk Factors
There are several potential causes of pediatric obesity, including maternal influence, sedentary activity, and eating and dietary habits.
Maternal influence
The NHANES III study determined that maternal obesity was the most significant predictor of obesity in children. Olson, Strawderman, and Dennison revealed that a mother's excessive weight gain during pregnancy was associated with a child's overweight by age 3. 20 In fact, Manum and colleagues confirmed that the effects of overweight and obesity from excessive maternal weight gain during pregnancy extended to the child's twenty-first year. 21 Children living with single mothers, those from low-income families, and those with a lack of cognitive stimulation at home were more prone to obesity. 22 An overweight child risks becoming an obese adult. Whitaker and colleagues retrospectively reviewed the charts of 854 HMO patients born in Washington State from 1965 to 1971 and concluded that parental obesity more than doubled the risk of adult obesity in both obese and non-obese children who are younger than 10 years. 23
Diet and activity
Wilson and colleagues found that an increase in sedentary lifestyle and poor diet choices and eating habits contributed to pediatric obesity. 15 Increased caloric intake of sweetened beverages and ready-to-eat processed meals, increased portion sizes in restaurants, increased number of meals eaten outside the home, decreases in outside play, and increased TV viewing and video gaming time have been implicated to contribute to pediatric obesity. 24
Review of the Literature Regarding Treatment Options
A number of studies addressed a multidisciplinary approach (medical monitoring, nutrition counseling, exercise program, and behavioral counseling) that also included family involvement.
Multidisciplinary approach involving the family
Dreimane and colleagues studied 264 participants with a mean age of 11.5 (73% Hispanic) that involved interactive nutrition and exercise sessions with behavior modification. 25 The study revealed that the addition of family support improved weight dynamics. Savoye and colleagues conducted a randomized control trial on 209 subjects of mixed ethnicity aged 8 to 16 years. 26 They concluded that a family intensive program that included diet, exercise, and behavior modification resulted in weight reduction that was maintained one year post intervention. Brehm et al. studied 57 girls 8 to 15 years of age. 27 They concluded that a multidisciplinary weight management program that included stress reduction and social support enhanced self-perception. Fulkerson et al. studied 667 males and 684 females at risk for becoming overweight. 28 They demonstrated that creating a positive family mealtime atmosphere and refraining from weight commentary resulted in greater well-being and less unhealthy weight control behaviors. An Australian study, the LEAP (Live, Eat and Play) study, studied 2,112 adolescents from all socioeconomic areas. The LEAP study illustrated that many families were willing to work with primary care providers in managing childhood obesity. 29
Multidisciplinary approach alone
Nemet and colleagues performed a randomized control trial evaluating the long- and short-term effects of a multidisciplinary approach to pediatric weight loss management. Fifty-four subjects (ages 6–16) participated in this study. 30 They concluded that the multidisciplinary approach had significant positive effects on body weight. Adkins et al. performed a correlational study on 52 African American girls, aged 8 to 10 years, evaluating an after-school program that focused on healthy eating and exercise. 31 Although they demonstrated improved BMI with increased physical activity, they concluded that family involvement would have benefited the girls. 31 Beech and colleagues evaluated 60 girls, 8–10 years of age, who attended weekly group sessions that focused on knowledge and skills. 32 They demonstrated the efficacy of a culturally relevant program geared toward the African American girls and their parents and caregivers. Chehab et al. studied 46 inner-city girls aged 12–18 years. 33 The program focused on addictive food avoidance, physical activity, and self-esteem building and demonstrated that this type of program was effective in reducing BMI. Skelton, DeMattia, and Flores conducted a study evaluating multiracial, multiethnic, multisocioeconomic children (n = 66, aged 2–18 years, M = 11 years) who were overweight, were obese, or had at least one obesity-related comorbidity. 34 The findings confirmed that a culturally diverse multidisciplinary weight reduction program was effective across diverse cultures and ethnicities. 34
Summary of Findings
The findings demonstrate that a multidisciplinary healthcare model that includes diet modification, promotion of physical activity and behavioral therapy, along with a supportive family environment is effective in pediatric weight management. In the studies that involved multidisciplinary treatment alone, the authors suggested that parental involvement would have benefited the study participants. This model is further supported by recommendations from the American Dietetic Association (ADA) and the Cochrane Collaboration. The ADA recommendations state that treatment for childhood obesity should be directed at the entire family, not just the obese child. 35
While the goal for the overweight child is weight maintenance, targeted efforts at weight loss for the obese child must be initiated. The Cochrane Collaboration examined 64 studies, of which 54 focused on lifestyle modifications (diet, exercise, and behavioral change) and 10 focused on drug treatment.14,36 These concluded that lifestyle modifications can improve outcomes for overweight at the 6- and 12-month visits. The Cochrane Collaboration suggested that sibutramine or orlistat in addition to lifestyle change were found to benefit patients; however, the benefit needs to outweigh risks of adverse events.
The American Academy of Pediatrics' (AAP) Expert Committee recommended significant changes to the assessment, diagnosis, prevention, and treatment of childhood obesity. 24 The committee reviewed and weighted all relevant data and current recommendations and established updated guidelines. They recommended more precise terminology and tightened BMI by age and percentile to identify four groups of children: underweight (BMI < 5th percentile), healthy weight (BMI 5–84th percentile), overweight (BMI 85–95th percentile), and obese (BMI > 95th percentile). The expert panel suggested that those extremely obese children with BMI > 99th percentile for age have the highest prevalence of cardiovascular risk, and identification of this high-risk group should lead to immediate treatment.
Target behaviors aimed to reduce the risk of overweight are listed in Table 1. The AAP recommendations include tertiary comprehensive multidisciplinary treatment for obese children. Children should be referred to this level of treatment after 3–6 months of traditional overweight therapy (calorie reduction and improved physical activity). Once the obese child is identified, he or she should receive the following therapy by a specialized pediatric obesity team: negative energy balance through structured diet and exercise, behavioral modification and food intake monitoring, weekly follow-up of body measurements, and a tailored family education plan and active consultation by medical subspecialists who can address existing comorbid conditions. Obese children (BMI > 95th percentile) who have significant comorbid conditions, as well as children with BMI > 99th percentile, should be referred to the pediatric bariatric surgeons, who are present within this multidisciplinary design.
Recommendations for Surgical Intervention and Bariatric Support
Surgery has been a successful treatment recommendation for severely obese adults for almost 20 years. The 1991 National Institutes of Health (NIH) consensus panel excluded those under age 18 years in their recommendations; and therefore, adolescent bariatric surgery was not recommended. 37 As a result, pediatric providers have been slow to recognize the emerging need to offer bariatric surgery as a potential treatment option for severe obesity. Dixon, Jones, and Dixon performed a systematic review of 18 eligible studies published in English. 14 The criteria included studies or reports of three or more subjects, the majority being within the pediatric age range, all less than 22 years of age at the time of surgery and with weight and BMI data for a period of at least one year prior to surgery. These included a total of 641 patients, 352 (55%) of whom underwent laparoscopic adjustable gastric banding (LAGB) and 150 (23%) of whom underwent a Roux-en-Y gastric bypass (RYGB). Four studies included results of 71 (11%) patients who underwent non-traditional operations (vertical banded gastroplasty) and 68 (11%) patients who underwent bilio-pancreatic diversion. The mean age was 16.8 years (range 9–21). Meta-analyses of the two most commonly performed operations demonstrated significant reductions in BMI for both the LAGB and the RYGB. Dixon and colleagues (2009) reported remission of T2DM in 10 of 11 extremely obese adolescents after bariatric surgery. Table 2 summarizes the results of this review. 38
Inge and colleagues recommended that children be referred to pediatric multidisciplinary centers where pediatric surgeons, specially trained in bariatric procedures, participate as an adjunct to the multidisciplinary support of these children. 39 They recommend that surgery be offered only to children who are successful participants in an ongoing multidisciplinary setting and only after success with weight management strategies has been established.
Browne and Inge summarized the current recommendations for adolescent surgical referral. 40 “Surgical candidates should be extremely obese and should have some identifiable consequence (physiological or psychological) to justify surgery.” Participation within a multidisciplinary adolescent weight management program is mandatory to measure ongoing weight loss, monitor health status, treat comorbid conditions, and provide counseling and support to the adolescent and family.
The risk–benefit decision making to recommend surgery for the adolescent population must assure ethical reasoning. 41 When comorbidities threaten the life of the adolescent, there is an ethical responsibility to utilize the knowledge from the adult population to recommend a surgical decision in the child. Evidence is emerging in the adolescent literature regarding comorbidity reduction and resolution following bariatric surgery within an adolescent weight management program.42,43 As pediatric bariatric surgery develops, long-term outcomes, comorbid conditions, quality of life, and healthcare costs need to be collected and evaluated.
Planning the Model
Based on this evidence, we are proposing a multidisciplinary tertiary team model for the treatment of pediatric obesity (Figure 1). Members of the team include a medical director, nurse practitioner, behavioral therapist, physical therapist, social worker, and nutritionist. A second tier of specialists (in pediatric endocrinology, cardiology, surgery, nephrology, and gastroenterology) will enhance the management of those with comorbid conditions. Children would enter the program by a referral from the primary care provider. Screening for comorbid conditions would occur, and, if such conditions are present, treatment would be initiated in this multidisciplinary environment. The team would facilitate appropriate identification and referral of surgical candidates. Post-surgical LAPB adjustments and ongoing surgical guidance would occur at this multidisciplinary clinic, specially targeted to adolescents.
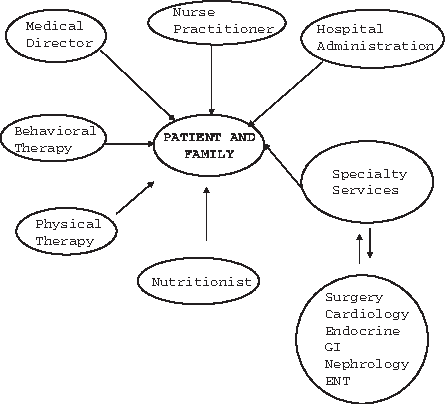
Proposed organizational structure for the comprehensive multidisciplinary childhood obesity clinic.
Areas for Further Investigation
Both prevention and treatment of pediatric obesity will be the ongoing challenge of the twenty-first century. Further research on the psychosocial determinants for behavior change and improvement in family interaction as well as cost-effective programs for primary and community care will benefit future at-risk children. 44 Finally, a combination of diet, exercise, behavioral change, and parental involvement has been shown to be modestly effective in pediatric weight loss. Those children at highest risk need to lose at least 5–10% of their body weight to reverse the comorbidities that threaten their life expectancy. 42 This population must be offered a surgical treatment option within the context of the tertiary multidisciplinary program that assures developmentally sensitive and family-focused care and careful long-term monitoring of comorbid conditions throughout their developing years. Further, tertiary data registries to collect and measure the outcomes of treatment proposals will ensure that effective treatments and outcomes are monitored effectively.
Establishing the cost-effectiveness of treatment that prevents or improves comorbid conditions will encourage policy makers and insurers to pay for treatment. Pediatric providers must be able to establish and sustain the financial viability in order to care for this vulnerable population. Reimbursement for obesity prevention and treatment must be guaranteed in order to secure success.
Summary and Implications for Nursing and Healthcare
The summary of the findings are in keeping with the recommended core competencies of the Institute of Medicine to “work in interdisciplinary teams-cooperate, collaborate, communicate, and integrate care in teams to ensure that care is continuous and reliable.” 45
Healthcare providers must focus attention toward treatment of those already morbidly obese children in addition to prevention. 46 The interventions should include a three-tiered approach as outlined by the American Academy of Pediatrics (AAP) guidelines: encouraging physical activity, a healthy diet, restriction of sedentary activities, and behavioral support for those at risk for obesity; a multidisciplinary approach for obese children; and, finally, a tertiary multidisciplinary treatment team to offer aggressive therapy to those whose lives are in danger. These programs should include the family, school, and community. 47 Multidisciplinary treatment programs can be effective in treating pediatric obesity. Unfortunately, only a small number of obese children participate in weight management programs. 30 The need exists for the establishment of more readily available multidisciplinary treatment programs.
Increasing physical activity is essential. The National Association for Sport and Physical Education (NASPE) states that children should build up to more than one hour of age-appropriate activity daily, engage in intermittent vigorous activity for more than 15 minutes, avoid extended periods of inactivity, and participate in a variety of activities. 22 The national guideline recommendation for both children and adolescents is to engage in at least 60 minutes of exercise every day of the week. 48
Conclusion
Children are not independent recipients of their care; they are cared for by parents, grandparents, extended family, and day care providers, and these adults' opinions influence the healthcare decisions made on their behalf. The pediatric multidisciplinary team approach assures sensitivity to the unique developmental considerations of the child and family and promotes support for the adherence to the commitment that long-term follow-up will be necessary. Pediatric providers are especially aware of the developmental and family-focused needs of the adolescent and are skilled at the group dynamic often necessary to influence the decision maker.
Healthcare providers should recognize that pediatric obesity not only is the child's problem but also requires support from the entire family, the community, the school system, as well as government policy makers. 49 Providers should be aggressive in managing pediatric obesity, and treatment should be combined with changes in diet plus increases in physical activity and reduction in sedentary behavior. 50
Healthcare providers must examine their beliefs and values regarding overweight children so that biases and misunderstandings can be rectified. Earlier recognition and guidelines to treat younger at-risk children should be initiated. Primary care office staff needs to be knowledgeable about the Body Mass Index (BMI) and how to sensitively discuss weight with parents and children. There should be age-appropriate anticipatory guidance for families about prevention and treatment of childhood obesity provided at each well-child visit. 51 Preventive strategies need to be applied to all children from birth onward in order to change family habits and improve lifestyle habits. 52
Pediatric obesity is a major public health concern. The potential costs to the healthcare system will be enormous if the current trends continue. The economic impact to the country jeopardizes our nation and threatens the economic stability of the entire healthcare system. Children and families must receive developmentally sensitive, multidisciplinary, multifocused care that assures sustainable weight management throughout the life span. Pediatric weight management and treatment should be tailored to the level of overweight. Those children at highest risk need access to a multidisciplinary tertiary model that offers a bariatric treatment program.
Footnotes
Disclosure Statement
No competing financial interests exist.