
Abstract
Adolescent bariatric surgery is one way clinicians are attempting to solve the problem of childhood obesity. In 2004, the Food and Drug Administration (FDA) granted investigational device exemption of the adjustable gastric band to determine the safety and efficacy of gastric banding in morbidly obese adolescents. The role of the dietitian in the multidisciplinary adolescent bariatric team is challenging. It is the responsibility of the dietitian to improve the adolescent's diet quality prior to surgery, teach the adolescent and the family the new eating guidelines after surgery, and to assess the nutritional adequacy of the diet post operatively. This article reviews the preoperative nutrition management, the nutrition guidelines followed for adolescents undergoing gastric banding surgery at Alfred I. duPont Hospital for Children, and reviews the unique challenges that working with adolescents presents to dietitians.
Introduction
Gastric banding was first approved by the Food and Administration (FDA) for use in adults in June 2001. It is a surgical weight-loss procedure that restricts the amount of food that can be consumed at one time. It is a purely restrictive procedure; therefore no malabsorption occurs with gastric band use. In 2004, the FDA granted an investigational device exemption (IDE) for use of the adjustable gastric band in adolescents in order to study the safety and efficacy of its use in this patient population.* In 2006, the Alfred I. duPont Hospital for Children received IRB and FDA approval to study the adjustable gastric band in adolescents. Since that time, 31 adolescent gastric banding surgeries have been performed. The bariatric surgery program at Alfred I. duPont Hospital for Children utilizes a multidisciplinary team approach. Team members include a physician, dietitian, exercise physiologist, psychologist, surgeon, and nurse coordinator. The team works with the adolescent and the adolescent's family for at least 6 months prior to the adolescent's surgery.
A workbook was developed by the team to guide the adolescent through the basic principles of living with the gastric band. The extensive workbook includes all the nutrition information the adolescent will need to review with the dietitian for a successful postoperative outcome. During this time, it is the role of the dietitian to work with the adolescent and their family to optimize their nutrition intake prior to surgery and to prepare the adolescent as completely as possible for the role nutrition will play in their lives after surgery. The purpose of this article is to review the nutrition guidelines developed for adolescents undergoing gastric banding surgery at Alfred I. duPont Hospital for Children, and to review the unique challenges that working with adolescents present to dietitians.
When preparing adolescents for bariatric surgery, it is paramount to keep in mind that adolescents are not “mini adults.” The adolescent should be physically mature prior to surgery; however, an adolescent often does not have the same emotional maturity or life experiences as an adult. It is important to work with the multidisciplinary team's psychologist to understand how much the adolescent can process at any given time, and to assess the adolescent's comprehension throughout the preoperative period. Keeping this in mind, the teaching of nutritional guidelines to the adolescent and the adolescent's family should be tailored to meet their unique educational needs and abilities. It has been this dietitian's experience that no assumptions should be made regarding the adolescent's nutrition knowledge base.
Nutritional information is reviewed with all adolescents and their families prior to surgery. Information includes topics such as hunger, satiety, reading food labels, calculating grams of protein, meal planning, and portion sizes. However, the manner in which the adolescent and family are taught these concepts will vary based on individual family needs. It is important to keep in mind that not only is the dietitian educating the adolescent but the adolescent's parent(s) and guardian(s) as well. Therefore it is imperative that the dietitian be able to reach both audiences with his/her teaching style.
Information Night
Prior to the adolescent's admittance into the gastric banding research study, the adolescent and a guardian are required to attend a 1-hour, informational session regarding the gastric band and the FDA study. Time is set aside during this hour to discuss the nutrition guidelines that the adolescent must follow after surgery. At this time, the dietitian also encourages the adolescent to think about how they will incorporate the nutrition guidelines into their lives, which encourages the adolescent to think about long-term nutritional changes. The nutrition guidelines reviewed during this meeting include:
• Need for a multivitamin and calcium supplementation
• Importance of adequate protein and fluids after surgery
• No use of drinking straws
• No drinking 30 min before, during, or after a meal
• Three meals per day (no grazing)
• No gum chewing
• Portion size of one cup for an entire meal
• No caffeinated/carbonated/sweetened beverages.
Initial Nutrition Assessment
During the first visit, it is important to assess the adolescent and family members' current nutrition beliefs and practices. The program at Alfred I. duPont Hospital for Children utilizes a two-page questionnaire, as well as a verbal questioning exchange. Beliefs and practices reviewed by the dietitian include:
• Consumption of sugary beverages
• Portion sizes
• Number of meals consumed away from home
• What fruit and vegetables the adolescent enjoys
• Meal skipping
• Dairy intake
• Meal times
• Sneaking food
• Meals/snacks consumed in front of a screen
• Number of snacks
• Emotional eating
• Eating out of boredom or in procrastination of homework
• Who cooks meals
• Who does the grocery shopping.
The nutrition guidelines introduced to the adolescent and family during information night are again reviewed, and the adolescent is asked what they anticipate to be the most difficult part of the guidelines to follow. The information gathered here informs the dietitian about what to focus on and revisit throughout the preoperative period.
The adolescent bariatric program at Alfred I. duPont Hospital for Children obtains nutritionally based laboratory parameters at study entry and postoperatively at 3, 6, 9, 12, 24, 36, 48, and 60 months. While there are no reports of common nutrient deficiencies in adults as a result of the gastric band, this clinic has taken precautions to monitor multiple lab values in the event that adolescents respond differently. Nutrition-related lab values assessed at this clinic include: hemoglobin, fasting blood glucose, magnesium, calcium, iron, ferritin, vitamin B12, folic acid, vitamin D25 OH, parathyroid hormone, albumin, thiamine, insulin, hemoglobin A1c, alanine transaminase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), cholesterol, high density lipoprotein (HDL), and triglycerides. Prior to the adolescent's first appointment, fasting lab work is drawn, and results are either sent or brought in for review. All nutrition-related lab values not only serve as baseline values for comparison after surgery, but they are also reviewed to determine if there are any preoperative nutrient deficiencies that need to be corrected.
If any deficiencies are noted in the lab work, they are addressed by the dietitian and physician and supplemented or monitored as medically necessary. Beginning at the first visit, adolescents are instructed to begin taking a general multivitamin with iron, as well as 1,000 mg of calcium daily. To ensure that the adolescent purchases these supplements and that the supplements are nutritionally complete, the adolescent is required to bring the multivitamin and calcium supplements to the next appointment for review by the dietitian.
Finally, hunger is reviewed. The dietitian spends time explaining that for the last 14–17 years the adolescent has become accustomed to gaining satiety by a certain amount of food, but that after surgery that will instantly change. It is essential that the adolescent begin assessing hunger and allowing the hunger to guide food intake, not external cues. The goal of a one-cup portion for meals is reviewed at every visit, and the adolescent is reminded that this portion should be the entire meal. It is also discussed that this portion size should be enough to satisfy any hunger.
A hunger scale ranging from 0 (ravenously hungry) to 10 (painfully full) is reviewed with the adolescent, and the adolescent is encouraged to maintain a hunger rating of between 3 and 7 at all times. Finally, the adolescent is instructed to keep a food and drink record throughout the pre- and postoperative period in order to promote reflection and mindful eating habits.
Teaching the Guidelines
A unique challenge of working with the adolescent bariatric population is creating effective teaching strategies for both the adolescent and the family. It is helpful to discuss with the adolescent how he/she best learns; whether the adolescent is an auditory, visual, hands-on, repetitious learner, or uses some combination of learning styles is important to know. Determining the learning style of the adolescent can help guide the dietitian's teaching to be as effective as possible. Our clinic has found hands-on learning and repetition to be effective.
Portion size is one of the more challenging topics to tackle. To meet this challenge, Play-Doh® is used to simulate portion sizes. This is a great way for the adolescent to demonstrate the exact portion sizes that will need to be consumed after surgery, as opposed to using a premade food model. The dietitian can then take the adolescent's presurgical portion size and remove part of it to illustrate how their portions will be changing after surgery. Play-Doh® is an effective tool for illustrating the portions that will fit into one cup of food, which is the postoperative recommendation. Another useful tool for reviewing portion sizes and how portion size affects the number of calories and protein consumed is the Perfect Portion® scale. The Perfect Portion® scale has a food label built into the scale that will change depending on the item code entered and weight of the item being measured.
Assessing Knowledge
Prior to receiving approval for surgery, the adolescent is required to demonstrate knowledge of the topics covered during the presurgical period. Knowledge is assessed through a variety of measures. Written quizzes are given, which include a food label quiz, as well as a general bariatric nutrition quiz (Fig. 1). Whiteboards with columns labeled “Okay” and “Not Okay” are used as an interactive knowledge assessment tool. The adolescent is given a variety of food and beverage models and is asked to place the food and drink in the appropriate column for each stage of the diet progression after surgery. This exercise allows the dietitian to provide the adolescent with immediate feedback. The adolescent is also asked to complete four sample meal plans (two liquid meal plans and two pureed meal plans) for review prior to surgical approval (Fig. 2).
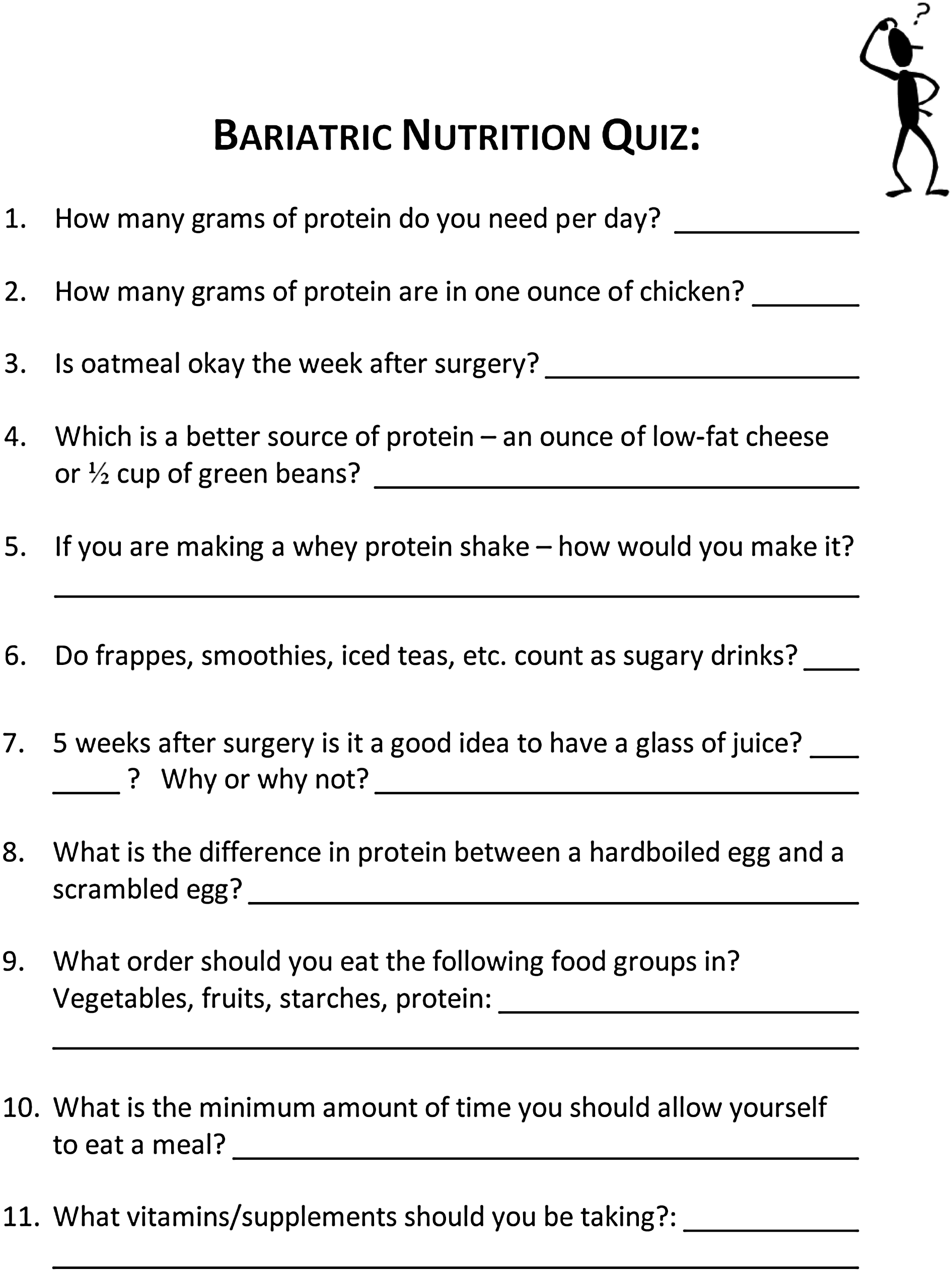
Nutrition quiz given to adolescent prior to surgery.
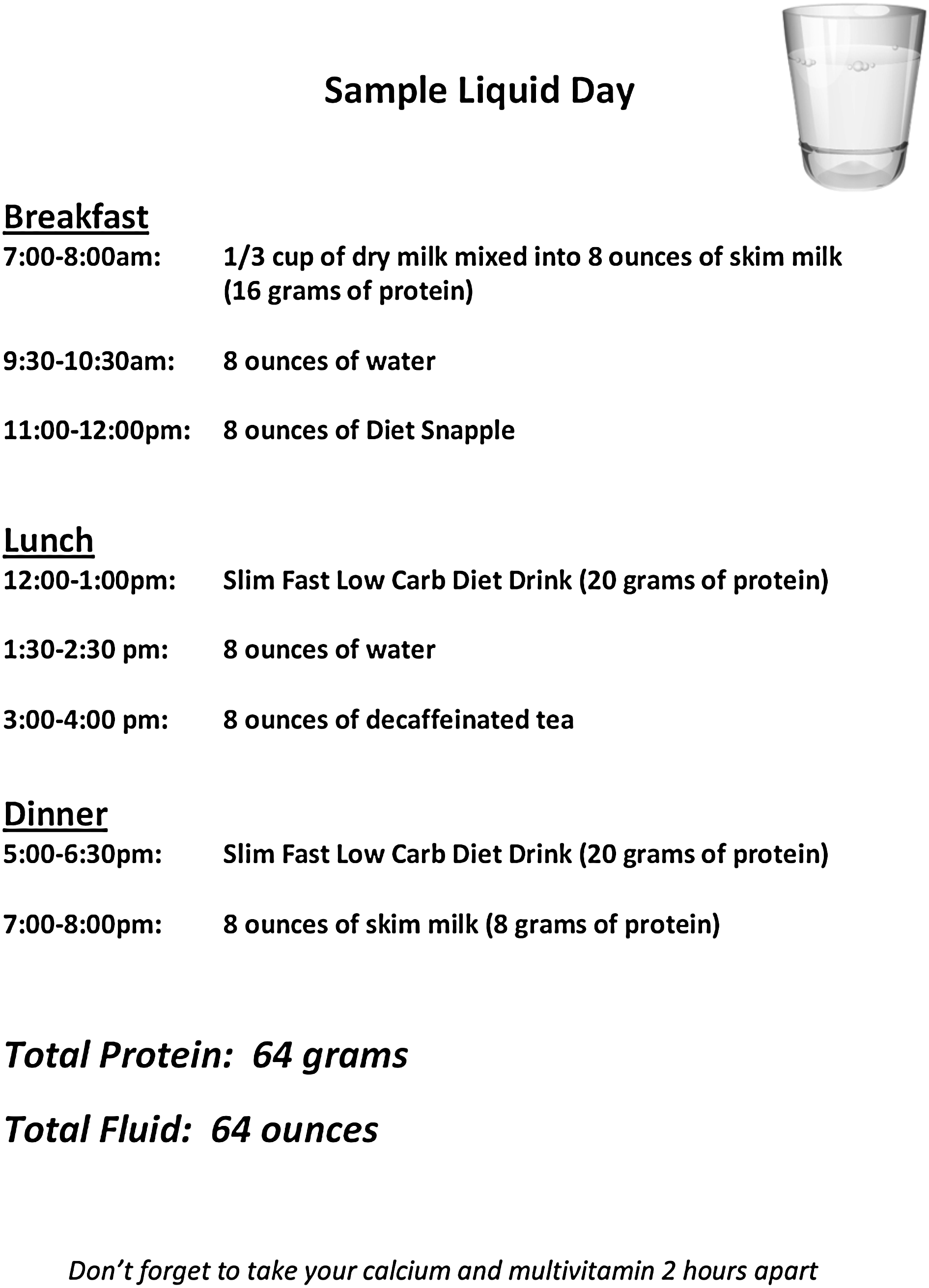
Sample daily liquid meal plan utilized during liquid diet phase after surgery.
Diet Progression
The importance of adherence to the diet progression plan cannot be overemphasized with the adolescent and the family (Fig. 3). Adolescents are encouraged to follow a healthy diet prior to surgery; however, it is not regimented until 2 weeks prior to surgery. At this bariatric clinic, the adolescent is placed on a low-calorie meal-replacement diet consisting of shakes and/or bars. The caloric level of this meal-replacement diet is determined by the adolescent's BMI. Calorie levels range from 800 to 1,320 per day. After 1 week of this meal-replacement plan, the adolescent returns for a follow-up session with the dietitian and psychologist to evaluate how the adolescent is handling the meal-replacement diet. Placement on this type of diet regimen does require medical supervision.
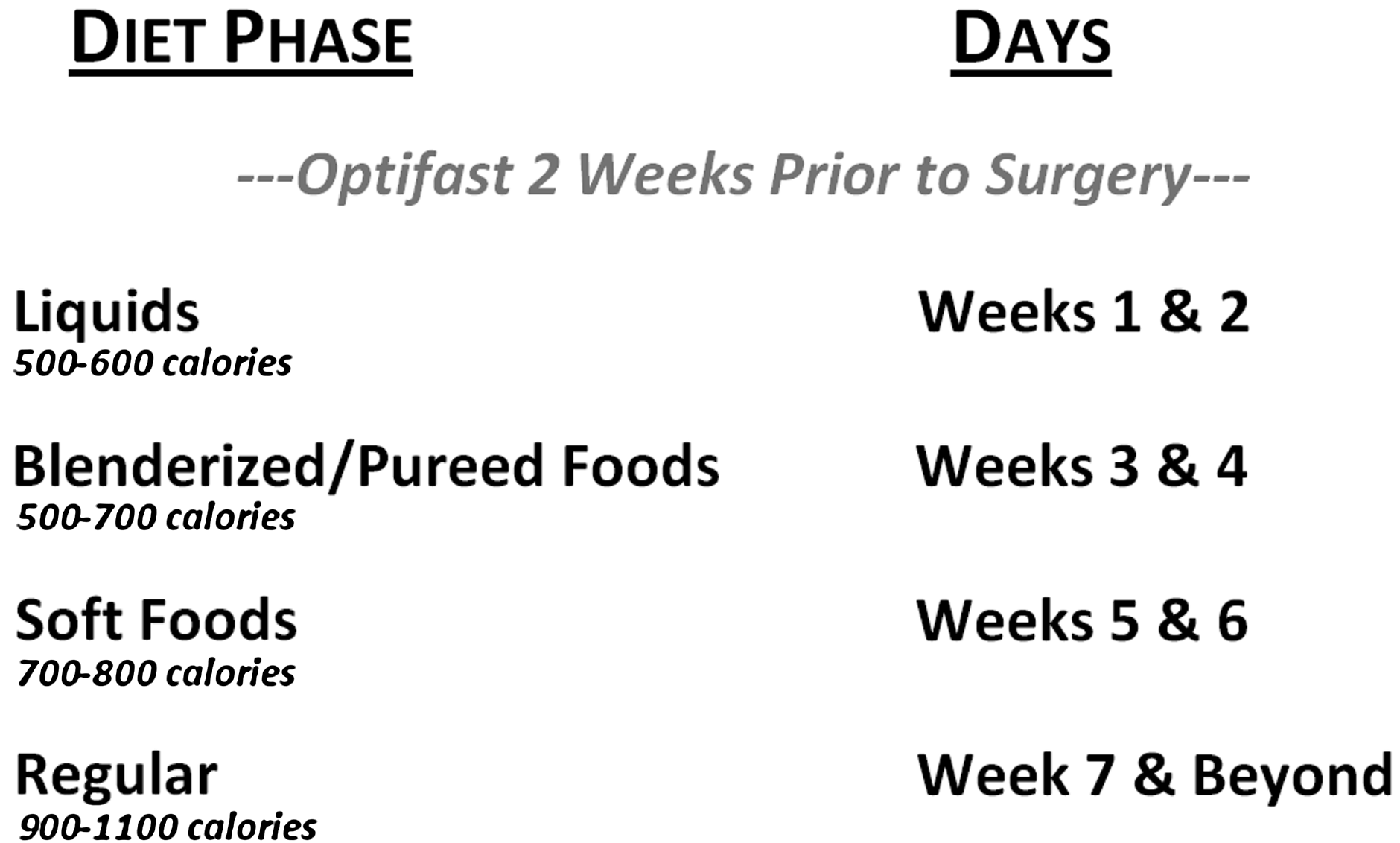
Quick reference guide for diet progression after surgery.
At our clinic, adolescents are placed on the meal-replacement diet for three reasons. First, there is evidence that a lower carbohydrate diet will help to shrink the liver, which will make surgery less complicated for the surgeon. 3 Second, the adolescent patient will need to be on a liquid diet for 2 weeks after surgery; therefore meeting with the adolescent 1 week into the meal-replacement diet to evaluate adherence and success can help provide the adolescent with support and tools that can help him/her adhere to the liquid diet postoperatively. Finally, being on a calorie-restricted diet should help kick-start the adolescent's weight loss. In our clinic, adolescent patients have experienced an average weight loss of 5.6 kg while on the two-week meal replacement diet.
The adolescent is placed on a liquid-only diet for the first 2 weeks after surgery. The daily caloric goal during this time is 500–600 calories, 60 g of protein, and a minimum of 64 oz of fluid. A mixture of nutrition supplement drinks such as Slim Fast Low Carb Diet®, Unjury®, and whey protein recipes are mixed and matched in meal plans for adolescents depending on their taste preference. See Figure 2 for a sample meal plan. Additional liquids such as broth, tea, and other calorie-free, caffeine-free beverages are also allowed during this time. It should not be assumed that the adolescent recognizes what is and what is not considered a liquid. It has been this dietitian's experience that some adolescents feel mashed potatoes, puddings, and yogurts are appropriate for their liquid meal plans. This should be discussed with the adolescent when reviewing sample meal plans.
During the third and fourth weeks after surgery, the adolescent's diet progresses to blenderized and pureed foods. During this phase, the daily caloric goal is 500–700 calories with the protein and liquid goals remaining the same as during weeks one and two. Adolescents are instructed to eat protein foods first, vegetables and fruits next, and lastly, starches and grains. Eating protein foods first is one way to make sure protein goals are met. In the preoperative period, the adolescent is given a list of appropriate foods from each food group and is instructed to create nutritionally complete pureed meal plans while keeping in mind that the entire meal should fit into one cup.
The third diet phase takes place during the fifth and sixth weeks after surgery, and includes a soft food diet. Soft foods are defined as foods that a fork can easily slice through. The protein and fluid goals remain the same; however, the daily caloric goals are now 700–800 calories per day. The soft foods phase is not reviewed in depth with the adolescent during the preoperative phase, but rather discussed in detail during the first postoperative visit. Raw fruits and vegetables, as well as stringy meats, are discouraged during this diet phase.
Postoperative week seven begins the eating patterns that are sustained for life. Long-term daily caloric goals are 900–1,100 calories, with protein goals remaining at 60 g per day with at least 64 oz of fluid consumed daily. The adolescent is cautioned that some individuals experience difficulty consuming stringy meats and bread products. The adolescent is also encouraged to spend at least 20 to 30 minutes consuming meals. The adolescent is instructed to get up and walk around if he/she experiences the sensation of food “getting stuck” in the esophagus. Additional lifelong eating strategies are also reviewed with the adolescents during postoperative group nutrition classes.
Postoperative Nutrition Management
The dietitian in the postoperative phase is responsible for assessing the adolescent's nutritional well-being. The following habits and symptoms are assessed at all follow-up visits: multivitamin and calcium supplementation compliance, portions, eating and drinking at the same time of the day, hunger, satiety, nausea/vomiting, reflux, swallowing difficulties, length of time to consume a meal, frequency of eating, and food choices. While there is no risk of malabsorption with the gastric band that would lead to nutrient deficiencies, limited intake, as well as the possibility of poor food choices, can lead to nutrient deficiencies. It is important to review nutritional lab parameters as often as they are available for trends and deficiencies. Beginning the sixth week postoperatively, saline may be added to the gastric band in order to restrict intake further. When the adolescent has the band filled, it is the responsibility of the dietitian to review how that fill will affect their intake over the next 48-hour period. When the band is filled, the adolescent is instructed to consume only liquids the rest of the day. The following day, a pureed diet is followed with instruction to consume one protein shake as well.
Nutrition Obstacles After Surgery
It has been this dietitian's experience that there are unique challenges when working with the adolescent who undergoes the gastric band procedure. For those adolescents having surgery during the school year, they need to feel comfortable packing liquid and blenderized/pureed lunches for the first 4 weeks after surgery. In our experience, schools are generally accommodating, and it is helpful if the dietitian is available to contact the school food service director or school nurse if needed in order to ensure that the adolescent has the school's support.
Another challenge for the adolescent after surgery is the ability to manage food choices when dining out with friends. As adolescents lose weight and their self-esteem improves, they tend to dine out with friends more often. It is important to give the adolescent the support and knowledge base needed to make food choices that will meet the nutrition guidelines, but not leave the adolescent feeling like an outsider.
Attempts have been made to reach out to and keep in contact with adolescents in unique ways. This bariatric clinic has created a Facebook support group that houses discussion boards, helpful links, as well as a wall for adolescents to connect with one another. It is a hidden Facebook group to ensure privacy, and is overseen by the bariatric team.
Conclusion
The role of the dietitian in the adolescent bariatric team is challenging. The dietitian must find meaningful and effective ways to educate both the adolescent and the adolescent's family. The dietitian should be responsible for ensuring nutritional adequacy of the adolescent's diet through education about food choices and portions, as well as supplementation. It is important for adolescents to understand the consequences of their choices. If the adolescent ignores the dietitian's advice and chronically overeats to the point of vomiting, the gastric band can slip, the pouch can dilate, and/or the esophagus can stretch. In addition, if the adolescent does not take multivitamin supplements as ordered and is strictly limiting their intake, there is the potential for nutrient deficiencies. As the number of adolescent bariatric surgeries increases, continued research and long-term outcome data will help the dietitian to provide the best nutritional care for the adolescent bariatric patient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
At the time of writing, the use of the gastric band in adolescents has not yet been approved by the FDA