
Abstract
Introduction:
Bariatric surgery is being recommended for select patients with diabetes for improvement in glycemic control or possibly remission of diabetes. Diabetes remission does not happen immediately. In an effort to meet the changing glycemic control needs for bariatric surgery patients safely, a project was developed using intravenous (IV) insulin on a general surgery nursing unit.
Methods:
Bariatric surgery patients were identified as requiring IV insulin in the perioperative period. Nursing education was provided, and IV insulin was administered using an established tool on the general surgery floor. We retrospectively reviewed the first 10 patients treated with the protocol compared with case-matched controls.
Results:
The protocol was utilized in 83% of the patients meeting IV insulin criteria. No hypoglycemic events occurred. There was a significant interaction effect by treatment group and time for blood glucose during the first 24 hours postoperatively. The patients on IV insulin had a significant improvement in their blood glucose compared to the case-matched controls (p=0.011). Nursing knowledge about diabetes care demonstrated an immediate improvement in scores using a pre- and post-class paired t-test (p<0.001). However, further reassessment of knowledge level 4 months after education showed a decline in knowledge scores.
Conclusions:
IV insulin can be used safely and effectively in the immediate postoperative period on the general surgery nursing unit for bariatric surgery patients with diabetes. Nurses likely will require ongoing and updated knowledge in care of the inpatient with diabetes for this high risk, low frequency intervention.
Introduction
The glycemic control benefits of weight loss are well known and well published. In 2011, a consensus working group of the International Diabetes Federation recommended that bariatric surgery should be considered as an appropriate treatment for obese patients with type 2 diabetes who have not been able to reach treatment targets. 6 More than 35% of the U.S. population were obese in 2009–2010. 7
People with diabetes are more likely to undergo surgery, particularly cardiac and bariatric surgical procedures. 8 Glycemic control in the immediate and prolonged postoperative time period for bariatric surgery patients is challenging. Changes in insulin action and β-cell function have been noted to occur in patients with type 2 diabetes mellitus within hours to days postoperatively.9,10 These changes require diligent monitoring and frequent adjustments to maintain glycemic control. Indeed, diabetes over the long-term postoperative course for many bariatric patients will completely reverse and is often termed “cured.”11,12 In patients with obesity, insulin resistance and impaired insulin secretion lead to the development of diabetes. In many cases, initial weight loss after surgery decreases insulin resistance sufficiently so that the person is able to maintain normal blood glucose levels.
Clinicians at the Duke Center for Metabolic and Weight Loss Surgery at Durham Regional Hospital (DRH) recognize the unique glycemic control needs of this patient population and consult with the diabetes management service for medication reconciliation postoperatively and at discharge. Bariatric surgical patients are often discharged within 48 hours of surgery, which leaves a short time frame to assess the physiological changes and pharmacokinetics of medications and make adjustments in the diabetes care plan during hospitalization. Administration of intravenous (IV) insulin has been recommended for the perioperative period because it allows for quick titration in the patient with acute illness. 13 IV insulin has been demonstrated as the most effective method for reaching glycemic targets due to its short half-life. Titration of the short-acting insulin infusion allows for almost immediate effects. 14 Several publications have demonstrated safe and effective use of IV insulin outside of the intensive care unit (ICU).15–18
Prior to 2011 there were policy restrictions at our hospital about the clinical setting in which patients could receive IV insulin. These settings included the ICU, cardiac step-down, and one general medicine floor. These restrictions resulted in variations in practice for postoperative bariatric patients. Glycemic control was either managed with subcutaneous insulin that often failed to meet the individual patients' needs on the general surgery nursing unit, or aggressively controlled with IV insulin when the patient was admitted to the ICU. Nurses working on the general surgery unit received specialized training in bariatric sensitivity and interventions to meet the unique nursing needs of these patients. If the bariatric patients were admitted to any other unit for IV insulin, they would often miss the benefits of having the specialized bariatric care in order to receive IV insulin. The provider admitting the patient would have to choose which had the higher priority.
In response to these issues, we conducted a quality improvement initiative to implement and evaluate IV insulin infusions in postoperative bariatric surgery patients outside of the ICU setting. In this report, we present the protocol we developed and the results of our pilot implementation.
Literature Review
Hyperglycemia is common in hospitalized patients. In a large community hospital, hyperglycemia was found in 38% of medical-surgical patients, with 26% of these patients having a history of diabetes and 12% identified as new cases of hyperglycemia. 19 Numerous observational studies have associated hyperglycemia with poor clinical outcomes in both medical and surgical patient populations, including wound infection, increased length of stay, mortality, and postdischarge morbidity.20–24
In 2009, the American Diabetes Association along with the American Association of Clinical Endocrinologists 14 published inpatient glycemic control recommendations for preprandial blood glucoses to be <140 mg/dL in patients outside of critical care with a maximum glucose excursion no greater than 180 mg/dL. Glycemic control has been demonstrated to reduce surgical complications, yet is frequently difficult to obtain with fluctuating insulin requirements due to insulin resistance, stress, varying nutritional support, and postoperative counterregulatory hormone responses.25–27
Sliding scale insulin (SSI) has been used for years to attempt blood glucose control in the hospitalized patient. As early as 1963, Robbins suggested that SSI should be eliminated, as its only advantages were it was simple to order and prevented frequent calls from the nurse to the physician. 28 SSI is reactive rather than proactive because it treats the patient only after hyperglycemia has occurred. Browning et al. conducted a MEDLINE search and reviewed 52 publications on the use of SSI. 29 From this review, they concluded there were no clinical trials to demonstrate the benefit and, as such, SSI is an inappropriate approach to blood glucose control in diabetic patients.
Regardless of clinical setting, a management plan that includes scheduled insulin therapy using basal and prandial insulin or continuous subcutaneous insulin infusion is the treatment of choice for persons with type 1 diabetes or longstanding type 2 diabetes that is no longer controllable with oral agents. 30 The American Diabetes Association and the American Association of Clinical Endocrinologists recommend hospitalized patients, outside of the ICU setting, should be managed with basal, nutritional, and correction therapy insulin rather than the use of SSI or oral antihyperglycemic agents. 14
In a meta-analysis, Buchwald found 22.3% of patients undergoing bariatric surgery had type 2 diabetes. 31 The immediate change in diet preoperatively (liquids are encouraged for all bariatric surgery patients prior to surgery) often decreases insulin requirements. The perioperative stress response increases insulin resistance. These two significant factors make predicting insulin requirements for bariatric patients very difficult postoperatively and increase the risk of both hyperglycemia and hypoglycemia depending upon the aggressiveness of the provider writing postoperative insulin orders.
Weight-based, basal–bolus insulin therapy has been repeatedly proposed for inpatient insulin therapy.32–34 However, randomized controlled clinical trials in the inpatient setting using weight-based insulin are limited. Basal–bolus insulin provided better glycemic control than SSI in two randomized controlled trials in medical and surgical patients.25,35 Notably, the RABBIT-2 Surgery trial demonstrated a statistically and clinically significant benefit in reducing the number of patients experiencing postoperative complications with basal–bolus insulin regimens, yet at a cost of increased hypoglycemia in this group. 25
Glycemic control is the goal for any hospitalized patient. This control is achieved though prevention and effective management of hyperglycemia or hypoglycemia. Fear of hypoglycemia is a barrier to both the ordering provider and the nurse administering insulin in the effective use of basal–bolus insulin therapy. 36 Cook et al. surveyed hospital staff about barriers to the implementation of glycemic control programs. 37 Sixty-one percent of respondents reported concern about causing hypoglycemia as a barrier, along with 55% who reported lack of physician endorsement. 37
Compelling evidence exists for the use of IV insulin to control blood glucose in the ICU setting, and it has been shown to prevent morbidity and mortality.21,26,38–40 However, hypoglycemia associated with tight glycemic control (targeting blood glucose 80–110 mg/dL) using IV insulin has been reported in numerous studies and associated with increased mortality in one study.21,26,38–41
Continuous IV insulin infusion has been shown to be safe and effective in controlling blood glucose in patients outside of the ICU using hourly glucose monitoring.15,17,18 Lien et al. first describe using their new nomogram for IV insulin titration in the medicine and surgery critical care units at Duke University Hospital. 16 They demonstrated that their IV insulin nomogram was efficacious and safe. Patients were more likely to have their insulin titrated in the setting of hyperglycemia without a statistically significant increase in hypoglycemia. Additionally they demonstrated that patients were three times more likely to be transitioned to subcutaneous insulin before discontinuation of IV insulin. 16 The protocol has been widely used across the hospital in the emergency department, ICU, and intermediate care units since 2005.
Davis et al. described implementing the same IV insulin infusion protocol in the same hospital on intermediate care units with nurse-to-patient ratios of 1:5 or 1:6 in 2005. 17 They used an audit and feedback method to implement the Lien–Spratt nomogram. Davis identified potential barriers among the nursing staff, including lack of knowledge and math skills. Education and easy access to calculators were implemented to overcome these barriers. The nomogram was implemented safely and successfully on general medicine units and then used on other adult inpatient units. 17
In 2009, Vinik et al. describe implementing an IV insulin protocol specifically for the non-ICU setting with goals of safety, simplicity, and glycemic control. 18 They provided inservice education about the protocol on each nursing unit. Their results demonstrated a very low incidence of hypoglycemia, a 21-hour mean duration of IV insulin, and a 9-hour mean time to the target glucose of <150 mg/dL. In the discussion, the authors indicate that hyperglycemic patients reached goal blood glucose without an increase in hypoglycemia (compared with ICU protocols and hypoglycemia rates) more quickly on IV insulin than reported by others with subcutaneous insulin. 18
Finally, Smiley et al. provided a retrospective report of using IV insulin infusion with 200 patients on general medicine and surgery units at Emory University Hospital. With a larger number of cases reviewed, the authors reported that 67% of patients reached the target blood glucose of <150 mg/dL by hospital day 2. However, they also reported that hypoglycemia, defined as at least one episode of glucose <60 mg/dL, occurred in 22% of patients. Another difference in this report compared with those previously discussed is the high rate (82%) of patients receiving nutrition and IV insulin. Smiley et al. reported a higher incidence of both hyper- and hypoglycemia in patients receiving nutrition.
For bariatric patients, use of weight-based insulin protocols as used in the RABBIT 2 Surgical trial may require insulin doses >100 units per day. 25 While tolerated by some, such large doses of insulin could lead to devastating hypoglycemia in others. In an effort to meet patients' needs better for glycemic control and postoperative nursing care, an IV insulin protocol was needed for use with the bariatric patients on the general surgery nursing unit that was safe, manageable by the nursing staff, and could assist the diabetes management service in establishing an initial subcutaneous basal insulin dose prior to discharge. In addition, nursing knowledge related to diabetes care needed to be addressed in order to gain nursing support for and safe implementation of a new protocol.
The aim of this project was to implement and evaluate an IV insulin protocol with a sample of bariatric surgery patients who were admitted to a general surgery nursing unit. Additionally, we sought to increase nurses' knowledge of inpatient diabetes care and safe administration of IV insulin.
Materials and Methods
Study design and measures
The project constituted a quality improvement initiative to implement a safe IV insulin infusion protocol using the Lien–Spratt nomogram for IV insulin titration on a general surgical nursing unit and to evaluate its use in bariatric patients (Appendix A). The Duke University Institutional Review Board approved this retrospective case-matched control review project. The project was conducted with data gathered for the 3 months after implementation of the IV insulin protocol compared to a case-matched group prior to implementation of the innovation. Data were abstracted from the billing system for procedure codes and diagnostic-related groups, and from the electronic medical record.
The first aim of the study was the evaluation of the protocol, which encompassed an assessment of safety and a comparison of blood glucose control before and after IV insulin protocol implementation among bariatric surgical patients. Given the small number of bariatric surgical patients requiring IV insulin during the study period, blood glucose values were compared with case-matched controls from bariatric surgical patients who had surgery in the prior year. The type of bariatric surgery, years of diabetes, preoperative diabetes therapy, age, race, HbA1c, body mass index, gender, admission glucose, and creatinine level may have some influence on glucose levels. Matching the patients as closely as possible for these factors allowed for closer comparison given the small number of patients meeting the inclusion criteria.
The second aim of the study was the education of the nursing staff, which involved attending a didactic 2-hour class on the nursing unit. All registered nurses providing care to the bariatric surgery patients were required to attend one class. Classes were offered at various times. Nurses were asked to attend when they were not scheduled to provide patient care, and they were paid their regular hourly salary to attend the class.
The nurse practitioner leading the project provided a 90-minute class using audience participation and specific patient case examples from recent inpatient stays. The class began with a 10-minute pre-education assessment using the Derr Insulin Use Knowledge Assessment tool (modified; Appendix B). 42 The class content included types of diabetes, basal–bolus insulin, types of insulin used in the hospital, and each one's action profile. Further discussion included initiation and titration of IV insulin using the Lien–Spratt nomogram, safe and physiologic transition from IV to subcutaneous insulin therapy, blood glucose monitoring, documentation of insulin therapy, limitations of SSI, and review of the nursing practice standard “Insulin Therapy Management in Hospitalized Adults” with particular attention to prevention, treatment, and documentation of hypoglycemia and considerations in special populations (i.e., elderly, liver or renal failure, malnourished or nil per os). Nurses were instructed to double-check insulin titration calculations with each other until they felt comfortable in titrating the insulin infusion independently. At the conclusion of the class, the attendees were asked to repeat the Derr Insulin Use Knowledge Assessment tool (modified).
Nursing knowledge was assessed using variations in scores as percentage of total correct on the Derr assessment tool collected pre-class, post-class, and 4 months after implementation of the IV insulin protocol. The Derr Insulin Use Knowledge Assessment was modified eliminating questions that were not specific to our formulary or had become outdated. Questions were added to target nursing knowledge on key components of IV insulin use. Face validity was obtained by review of experts in the diabetes field. Construct validity will need to be further investigated.
Organizational setting
Durham Regional Hospital (DRH) is a 369-bed acute care hospital that is part of the Duke University Health System. DRH serves the healthcare needs of Durham, Orange, Person, Granville, and surrounding counties in North Carolina and southern Virginia. A total of 14,122 surgeries were performed in 2010, including bariatric, general, gynecologic, urologic, and orthopedic in both the inpatient and same-day surgery areas. The general surgery nursing unit has 28 beds of which six suites are equipped to handle morbidly obese bariatric surgical patients. The Duke Center for Metabolic and Weight Loss Surgery at DRH is an American Society for Metabolic and Bariatric Surgery (ASMBS) Center of Excellence. The hospital has two operating rooms specifically for bariatric surgery, and performed 783 bariatric surgeries in 2011.
Intervention
In an effort to better meet the bariatric diabetes patients' needs for glycemic control and postoperative care, an IV insulin protocol was implemented for bariatric and general surgical patients. All patients undergoing bariatric surgery with a history of diabetes should have a HbA1c performed within 3 months prior to surgery. The protocol defined use for IV insulin starting intra- or postoperatively if the blood glucose was >150 mg/dL in the patient with a history of diabetes, taking insulin, and having an HbA1c >8%. IV insulin was also to be initiated in a similar fashion for any patient with an HbA1c >10% or in any patient with a blood glucose >300 mg/dL at any time perioperatively. IV insulin was titrated using the Lien–Spratt nomogram and continued until the morning after surgery (Appendix A). 16 The goal was to have patients transitioned from IV insulin to another form of glucose control (usually subcutaneous insulin) by 9:00 a.m. the morning after surgery unless clinically unstable.
The Lien–Spratt nomogram is a method of titrating IV insulin based on the rate of change of plasma glucose and the patient's insulin sensitivity. It simplifies the decision making to a math calculation of current rate of insulin infusion times a multiplier found on the nomogram itself. (See Appendix A). This eliminates if-then statements and columnar algorithms. However, it does not eliminate the possibility of error from math calculation or looking up prior and current blood glucose incorrectly. 16
Each patient started on IV insulin was followed by the nurse practitioners on the Endocrinology and Diabetes Management Service. The patients were seen at least daily and had electronic records reviewed with each visit and more frequently as necessary. Particular attention was paid to the titration of insulin, hourly blood glucose monitoring, and documentation of insulin infusion. The nurse practitioner was either the person initiating the insulin infusion or was notified by the postanesthesia unit of IV insulin initiation. The authors reviewed all cases occurring in the first 3 months after implementation of the IV insulin protocol for appropriate patient selection, accurate utilization of the titration nomogram, and safety of the protocol as measured by hypoglycemia events.
Using the Lien–Spratt nomogram, nurses were in direct communication with the nurse practitioners if they had any questions about the IV insulin, their patients' diabetes care, or if they were at all uncomfortable with what was happening with the IV infusion, their patient's blood glucose, or changes in patient condition. Patient safety was the highest priority.
Results
Patient clinical characteristics and blood glucose control
Education about IV insulin was complete by the second week in October 2011, and we began using the protocol with the first patient in mid-October. All bariatric surgery records from November 1, 2011, to January 31, 2012, were reviewed retrospectively for use of IV insulin. A total of 158 patients had a bariatric procedure during the review period; 61 had a known history of diabetes. IV insulin was initiated in 10 patients who met the criteria for the IV insulin protocol during the review period. Two additional patients should have had insulin started according to the criteria above but were not started on IV insulin, indicating an 83% protocol fidelity rate. One had a mean blood glucose of 131 mg/dL postoperatively and the other a mean of 234 mg/dL.
Given the small number of cases, a case-matched control was used to compare blood glucose control with patients from the prior year, as previously described. The clinical characteristics of the patients receiving IV insulin and the matched controls are presented in Table 1. The groups were equal in types of procedures with the majority being Roux-en-Y and one pair of biliopancreatic diversion with duodenal switch. Body mass index (BMI) ranged from 35–64 kg/m2 with the IV insulin group having a slightly higher, but not statistically different, mean of 47.5 kg/m2 versus 45.9 kg/m2. Two patients in the IV insulin group had creatinine ≥1.5 mg/dL (1.5 and 1.6). No one in the case matched controls had creatinine ≥1.5 mg/dL; again there was no difference in the mean creatinine between the groups. The only significant difference between those on IV insulin and the case-matched controls was race, with the controls being 80% African American and the IV insulin group being 80% Caucasian.
No episodes of hypoglycemia occurred in implementing the IV insulin infusion, nor were there any hypoglycemic events in the case-matched controls. Blood glucose control was compared using 6-hour postoperative interval means for comparison of each group. The patients receiving IV insulin had more blood glucose data points with hourly monitoring as compared to the control patients having blood glucose monitoring every 6 hours. Therefore, a factorial repeated measures analysis of variance was conducted to examine group differences in blood glucoses over time during the first 24 hours postoperatively. Power analysis for this procedure suggested that to achieve acceptable power (near 80%), the linear interaction effect is the most appropriate model for interpretation. There was a significant interaction effect between the treatment group and time of blood glucose measure during the first 24 hours postoperatively. The patients on IV insulin had a statistically significant improvement in their blood glucose as compared to the case-matched controls F(1, 18)=8.15, p=0.011.
Follow-up analysis indicated that both treatment groups showed a decrease in blood glucose over time but at very different rates (see Fig. 1). Specifically, the IV insulin group had a sharp drop from the 6-hour to the 12-hour time point, and again from the 12-hour time point to the 18-hour time point, whereas the control group showed only a slight decrease across the three time points. Based on the small sample size with longer-term glucose levels (n=9 vs. 9 at 48 hours, 6 vs. 4 at 60 hours, and 6 vs. 3 at 72 hours), individual t-tests rather than repeated measures analysis were conducted to compare treatment groups on blood glucose levels at the final three time points (48 hours, 60 hours, and 72 hours). Results showed no significant differences between groups for those time points.
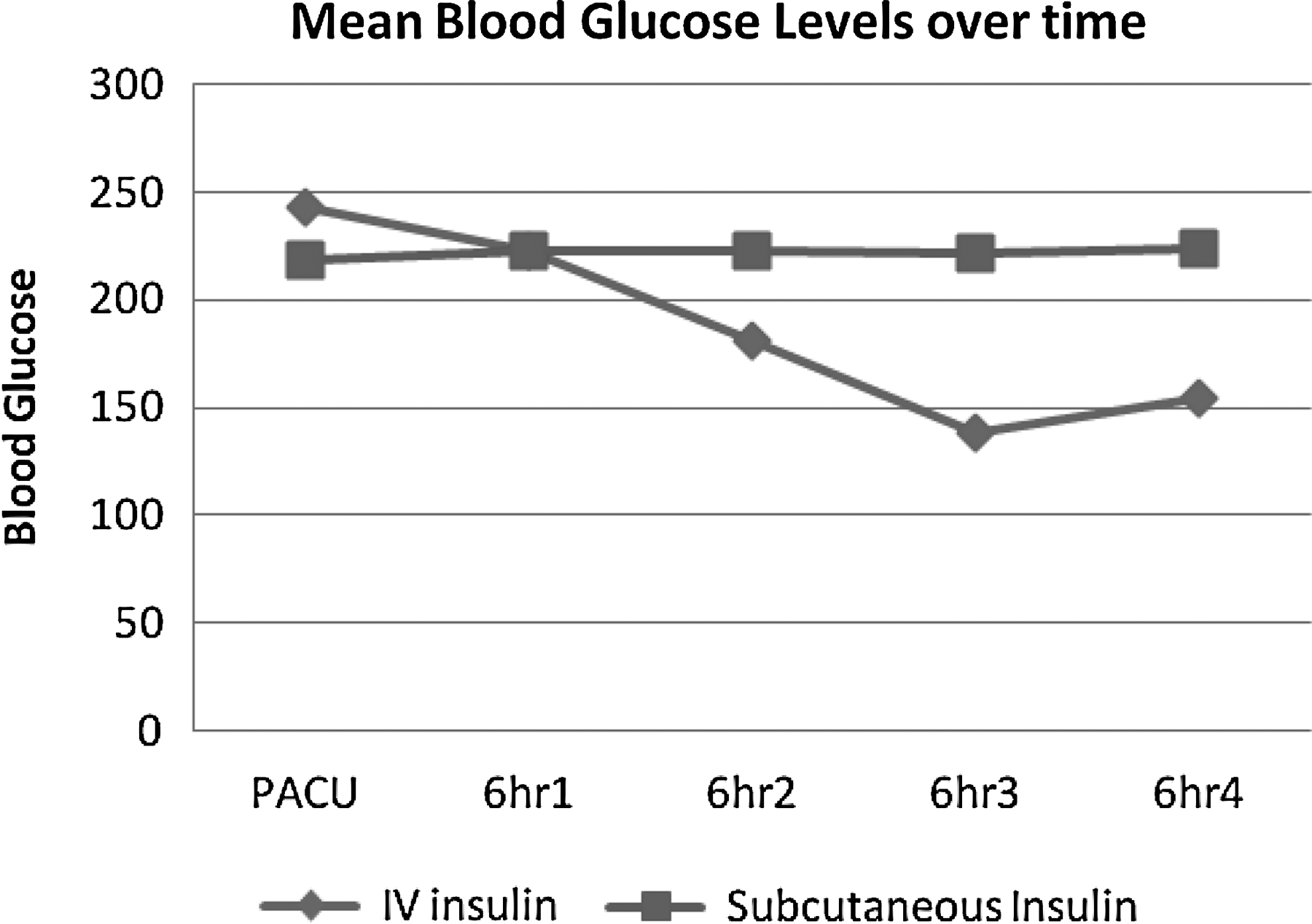
Blood glucose values for intravenous insulin and case-matched controls.
Each case on the IV protocol was reviewed for accuracy of insulin titration and frequency of blood glucose monitoring. A total of 175 blood glucose values were measured in the IV insulin group. No hourly blood glucose value was missing while the patient was on the insulin infusion. Of the 175 insulin infusion calculations, one error was made in insulin infusion rate adjustment, which provided the patient with 0.4 units/hour less insulin than the nomogram calculation. The average length of time the patient was on an IV infusion was 22 hours (±3.2).
Nursing education and knowledge assessment
A total of 29 out of a possible 30 registered nurses attended the training session for diabetes care and use of IV insulin. Each nurse attending training, except one, completed the knowledge assessment. The aggregate mean of scores improved immediately after education but declined over time (at 4 months; see Fig. 2). The immediate pre and post paired t-test demonstrated significant improvement in scores (t(27)=−6.212; p<0.001), and this was consistent with the general feedback from the nurses in the class.
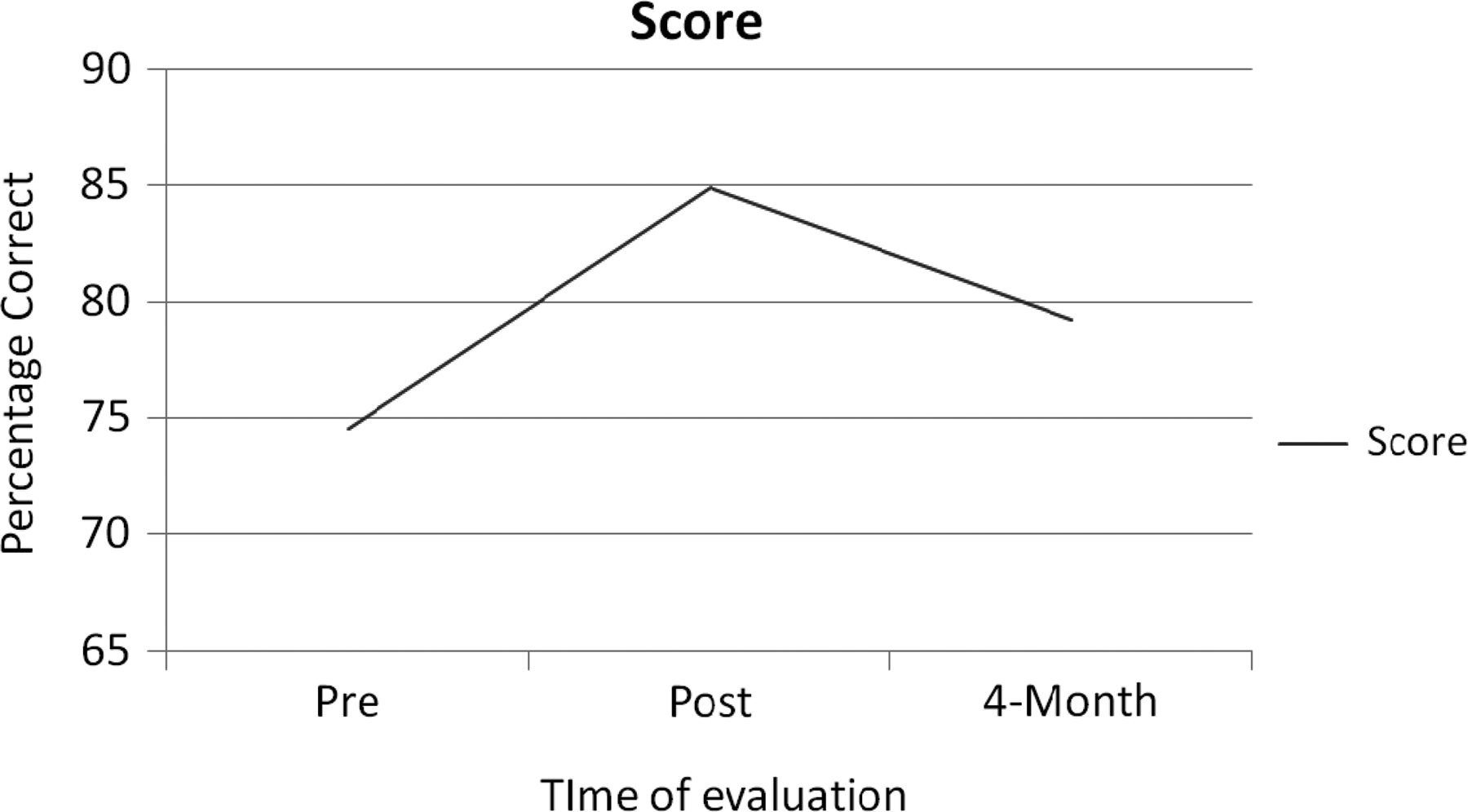
Scores on Derr (2007) Insulin Use Knowledge Assessment Tool (modified). 42
Each nurse that attended the initial class was asked to complete a knowledge assessment 4 months after implementing the IV insulin project. A total of 16 of the 28 nurses completed the follow-up test, but only 12 included an identifier that could be matched to their previous test. Looking at the mean scores on Derr 42 at all three time points with repeated measures ANOVA, there was an effect of time with the immediate improvement at the end of attending class, but from posttest to 4-month follow-up, the scores went back down (F(10)=8.246; p=0.008). This was a small subset of the nurses (12 of 28); therefore, this effect needs to be explored in a larger group. However, it does indicate a trend in loss of the knowledge gained in the class.
Nurses' feedback was sought regarding their concerns about caring for patients with IV insulin both before implementation and after the initial 4 months of protocol use. The greatest concerns prior to implementation were having the knowledge to provide safe patient care with IV insulin, the required frequency of BG monitoring, and nurse–patient ratios. At 4 months post implementation, the concerns were less but still revolved around safety issues with nurse–patient ratios, adjusting to the protocol, and having multiple patients with IV insulin (see Table 2). Of the 10 nurses who indicated having cared for a patient with an IV insulin infusion under the new protocol, seven were positive about the experience and three expressed concerns over having two patients at one time on insulin infusions.
Discussion
The objective of this project was to improve the care of the bariatric surgery patient by providing the safe utilization of IV insulin when needed on the surgery nursing unit via a method manageable by the nursing staff. IV insulin requires frequent blood glucose monitoring and has often been thought to be beyond the ability of the general nursing unit to manage safely. Several publications have documented the safe use of the Lien–Spratt nomogram outside of the ICU.15–18 According to our results, IV insulin via the Lien–Spratt nomogram is again documented as safe to be used on acute care nursing units. However, the generalizability is limited given the small sample size. Ongoing analysis of our data with bariatric patients and the Lien–Spratt nomogram is necessary.
Nursing knowledge related to diabetes care has room for improvement. This study is consistent with others published, demonstrating a lack of understanding of the pharmacokinetics of insulin and the basics of inpatient diabetes care.42–44 Surgical nurses rarely find patients admitted to their unit specifically related to their diabetes; rather diabetes is a comorbid condition. Diabetes care and medications to treat diabetes have changed dramatically over the past 10 years, making maintaining knowledge in the area a challenge in the inpatient setting.
As others have demonstrated in implementing IV insulin outside of the ICU, nursing knowledge related to inpatient diabetes care and specifically IV insulin is important in safely implementing an IV insulin infusion protocol.17,18 Vinik et al. reported higher rates of hypoglycemia when their protocol was used on patients receiving discrete nutrition. They also state the importance of physician and staff education when using their protocol. 18
In the pre-education assessment, nurses scored similarly to those in Derr et al.'s original report on nursing knowledge using the Derr tool. 42 Consistent with others' reports, some nurses were surprised at what they did not know in the pretest and were reassured with their scores after participating in class.42,45 We have demonstrated that providing education on a one-time basis does not lead to ongoing complete knowledge retention. This is particularly concerning when using a low frequency, high risk medication such as IV insulin. Having a consistent plan for education and review of insulin titration method may be critical in maintaining the safe use we have demonstrated in our first few months of IV insulin use with bariatric patients. Ongoing assessment will be necessary.
Our nurses have indicated an additional issue to address as we move forward. Currently IV insulin infusion qualifies a patient for step-down status. Having an IV insulin infusion patient (or multiple patients, as several nurse surveys indicated) along with other more acutely ill patients qualifying for step-down status may be overwhelming for the nurse. Patients with IV insulin may not need to be classified as step-down, but instead may require a nurse–patient ratio that is lower than the standard for the surgical unit. In addressing this issue, we would also need to conduct a formal cost comparison of IV insulin to subcutaneous insulin. Clearly there is an increase in the cost of resources and staff time, but there is also a clear difference in the cost of care in the ICU versus step-down status on the general surgery unit.
Identification of patients who may be candidates for IV insulin requires some additional attention. Only 82% of the bariatric surgery patients meeting the criteria for IV insulin were actually started on an infusion. Of the two not on IV insulin, perhaps one did not need the infusion as he/she had a mean postoperative blood glucose of 131 mg/dL. However, the other patient clearly needed IV insulin, with a mean blood glucose of 234 mg/dL. Coordination of identification with the surgeons and preoperative screening team may allow for earlier identification of IV insulin candidates.
The Lien–Spratt nomogram for IV insulin is used on all other units where IV insulin can be ordered in the hospital. The hospital's electronic medical record does not allow for a quick entry of the insulin infusion rates. Therefore, a paper documentation tool that has been used on other units for IV insulin infusion was continued for this unit implementation. Two of the 10 patients reviewed had records of IV insulin being ordered and blood glucose monitoring every hour, but the actual titration documentation sheet could not be located in the electronic record (scanned in from the paper record after discharge) and therefore were not included in the review of accuracy of titration.
Numerous studies have shown benefits for patients with the use of IV insulin, but most have also shown a significant increase in hypoglycemia.26,38,40,41 The Lien–Spratt nomogram used in this study did not increase hypoglycemia; in fact, there was no hypoglycemia in any patient on IV insulin. Having used the nomogram in other areas of the hospital for more than 6 years, we have anecdotally seen most patients' average blood glucose at 140 mg/dL while using the Lien–Spratt nomogram for insulin infusion titration.
One issue identified was a possible unintended increase in length of stay for patients receiving IV insulin. This is demonstrated in comparison to the case-matched controls being less likely to still be in the hospital at further postoperative time points (i.e., 72 hours). It was the express intention of the protocol not to increase length of stay and to transition patients from IV insulin to subcutaneous insulin earlier on postoperative day one. Fifty percent of patients were off the insulin infusion by noon on the day after surgery; the remainder were off by 6:00 p.m. Clearly, late transition off the insulin infusion will delay discharge. However, it is unknown if there is a clinical difference in these patients that prevented transition earlier.
A secondary objective of this project was to have data to help the diabetes management team in determining appropriate doses of subcutaneous insulin from the IV insulin titration data. Given the increase in blood glucose over time after transition from IV to subcutaneous insulin, this objective was not met. In informal discussion with the nurse practitioners on the diabetes management service, they did feel the IV insulin gave them additional data to transition more appropriately, but they still found glycemic control a challenge in the bariatric population with changing insulin resistance and nutrition.
This review of implementing a protocol for IV insulin is limited by the small number of patient cases reviewed, the short time frame, and the retrospective nature of the review. More data are needed to review the impact on the general surgery patients. However, the same nurses will be providing care and using the same insulin titration protocol. Thus an opportunity presents itself, and given the safety of the Lien–Spratt nomogram, we could also consider utilizing it in other surgical patient populations, particular orthopedics.
Summary
There is a significant opportunity for improvement in nursing knowledge as it relates to diabetes care, and one 2-hour class does not provide all the education necessary for maintaining knowledge over time. Insulin is regularly cited as one of the highest risk medications used in the hospital by the Joint Commission and American Society of Health-system Pharmacists. Commitment from nursing leadership coupled with time and resources are needed to maintain continuous learning related to diabetes care for the surgical nurse.
IV insulin can be used safely outside of the ICU with bariatric and general surgery patients using the Lien–Spratt nomogram as an insulin titration protocol. These results demonstrated no hypoglycemia and significantly improved blood glucose control in the first 24 hours after surgery. While postoperative blood glucose control has been associated with improved outcomes, further study is needed in the bariatric population to determine the role of blood glucose control in the immediate postoperative period.
Footnotes
Acknowledgment
The authors would like to acknowledge the invaluable assistance of Julie Thompson with statistical analysis.
Disclosure Statement
Melanie Mabrey discloses she is a consultant and on the speaker's bureau for Sanofi Pharmaceuticals.
Appendix A-Lien-Spratt Nomogram Appendix
Appendix B—Derr (2007) Insulin Use Knowledge Assessment Tool (Modified) 42
1. Novolin 70/30 is:
a. 70% NPH, 30% Regular b. 70% NPH, 30% glargine (Lantus) c. 70% protamine, 30% lispro (Humolog) d. 70% glargine, 30% aspart (Novolog)
2. Glargine (Lantus) is:
a. NPH b. Humalog c. Basal insulin d. Rapid-acting insulin
3. In general, a rapid-acting insulin (Lispro, Aspart, or Glulisine):
a. Peaks within 6–8 hours b. Peaks within 1–2 hours c. Peaks within 4–6 hours d. Has no peak
4. In general, NPH insulin:
a. Peaks within 4–10 hours b. Peaks within 12–24 hours c. Peaks within 2–4 hours d. Has no peak
5. Which of the following is a cloudy (rather than clear) solution?
a. Glargine (Lantus) b. NPH c. Regular d. Aspart (Novolog)
6. What is the half-life of IV insulin?
a. 5–10 minutes b. 30 minutes c. 1 hour d. 3 hours
7. The American Diabetes Association (ADA) definition of hypoglycemia is a blood level less than:
a. 50 mg/dL b. 70 mg/dL c. 80 mg/dL d. 100 mg/dL
8. In order to avoid complications when a patient is NPO:
a. Discontinue all insulin b. Continue basal insulin c. Continue only supplemental scale insulin d. Continue only rapid-acting insulin
9. Supplemental scale insulin is best used:
a. To meet basal insulin requirements b. To cover carbohydrates eaten in meals c. To correct elevated blood glucose levels d. To treat diabetes in patients previously on oral agents
10. When converting from an IV insulin to subcutaneous insulin, start subcutaneous insulin:
a. At least 1 hour before stopping the infusion b. At the same time as stopping the infusion c. 1 hour after stopping the infusion d. 4 hours after stopping the infusion
11. How frequently should blood glucose monitoring occur initially in patients on IV insulin infusion?
a. Every 30 minutes b. Every 60 minutes c. Every 2 hours d. Every nursing shift
12. Appropriate and safe use of scheduled insulin therapy is complicated by which of the following?
a. Concerns about hypoglycemia b. Variability in the nutritional status of patient c. Lack of familiarity with different insulin d. All of the above
13. Higher doses of insulin are often required for which patients?
a. Type 1 diabetes b. Stress-related hyperglycemia c. Those receiving high doses of glucocorticoids. d. All of the above
14. For patients receiving tube feedings and regularly scheduled insulin, caution may be needed in:
a. Dislodgement of the feeding tube b. Cycling feedings overnight in patients who may go home on tube feedings c. Holding tube feedings because of nausea or high residual d. All of the above e. None of the above
15. According to policy, how soon after treating hypoglycemia should you recheck blood glucose?
a. 10 minutes b. 30 minutes c. 60 minutes d. With next meal
16. Hyperglycemia in the hospital may actually be: _______?
a. Diabetes that had not been previously diagnosed b. Postoperative hyperglycemia or stress hyperglycemia c. A potential risk of diabetes in the future d. All of the above
How familiar are you with the nursing practice standard at DRH titled “Insulin Therapy Management in Hospitalized Adults”?
very familiar somewhat familiar not at all familiar unaware
How concerned are you about your ability to care for a patient with IV insulin?
very concerned somewhat concerned not at all concerned
What is your reaction when your patient has a hypoglycemic event?
Panic Alarm Concern Understand it happens
Would you call a rapid response for a low blood glucose?
Yes No Under certain circumstances
Comment: _________________________________________________________________________________________________
What concerns do you have about having IV insulin on 6-3? ________________________________________________________
___________________________________________________________________________________________________________