
Abstract
Over the past several decades, obesity has become an increasingly important problem for adolescents in the United States. As more children struggle with obesity-related comorbidities and due to the lack of sustained success with medical and behavioral weight-loss programs, the laparoscopic sleeve gastrectomy (LSG) has emerged as an effective surgical option for significant weight loss first in the adult population and now among adolescents. Nurses play an integral role in the success of the patient undergoing sleeve gastrectomy in both the preoperative and post-operative phases. Their expertise in patient education makes nurses well suited to provide patients and families with anticipatory guidance and nutritional support throughout the process. In addition, the compassion and caring that is unique to the nursing profession allows nurses to excel in the care of patients with the complex medical and psychological disorders related to obesity.
Introduction
Nutritional and lifestyle (i.e., physical activity) education to prevent children from becoming obese is an integral aspect of reversing the obesity epidemic. However, for those adolescents already categorized as obese, medical or surgical treatment becomes the only available option. There is little use of pharmacologic agents in the pediatric population due to side effects and lack of substantial weight loss. 7 Therefore, much focus has been given to bariatric surgery as an avenue to achieve a healthier lifestyle for those who have failed a medically managed, behavior modification weight-loss program. Historically, gastric bypass has been the surgery of choice for adolescents and adults. Most studies have demonstrated significant excess weight loss and resolution or improvement of most, if not all, comorbidities. 8 Unfortunately, this procedure has numerous risks and requires lifelong nutritional monitoring due to its malabsorptive nature. This has led to an increased utilization of the sleeve gastrectomy as a standalone weight-loss surgery in adults after its acceptance by the American Society for Metabolic and Bariatric Surgery (ASMBS) in its position statement in 2007. 9 More recently, the sleeve gastrectomy has gained attention in the adolescent population as being an attractive, non-device surgical option that has fewer risks than gastric bypass with similar resolution of comorbidities. 10 The sleeve gastrectomy was first introduced as the initial step of the biliopancreatic diversion and duodenal switch procedure. 11 When the biliopancreatic diversion and duodenal switch was performed in patients with a body mass index (BMI)>60, it was done as a staged procedure with the formation of a tubular stomach as the initial step. It was noticed that patients lost a significant amount of weight after this primary step in the procedure and did not necessitate the second operative stage. 12
After a sleeve gastrectomy, weight loss is thought to be achieved through reducing the size of the stomach (thus restricting food intake) and also via hormonal feedback mechanisms, which are not fully understood. 13 The decreased plasma levels of ghrelin, a hunger hormone, found in patients who have undergone a sleeve gastrectomy may be one endocrine mechanism related to weight loss following this operation. 14 In the following paragraphs, we will detail the steps needed for facility readiness, patient selection, technical aspects of the operation, role of nursing care, and the expected outcomes for adolescent patients who undergo sleeve gastrectomy for weight management.
Facility Readiness
Prior to initiating the care of the bariatric population, it is important that facilities are appropriately equipped. This can be particularly important in pediatric environments/children's hospitals, which are often initially designed to care for smaller patients. Facilities should be equipped with toilets, exam tables, and chairs that can accommodate the increased weights associated not only with the morbidly obese patients but also their families who are often also morbidly obese. In addition, patient care items such as bariatric wheelchairs, bariatric stretchers, appropriately sized patient beds, gowns, blood pressure cuffs, socks, bedside commodes, and bed pans are essential. Patient mobility assistance devices such as hovermats and lifts are also critical to patient and staff safety. Not only should this equipment be easily accessible, staff should be adequately trained and comfortable with its application. Appropriate rescue equipment should also be readily available in case of emergency situations. Large bag valve masks, long intravenous catheters, long intraosseous catheters, and code carts with appropriate doses of medications should be available. Hospital staff should be cognizant of the weight limits on stretchers, operating room tables, computed tomography scanners, and magnetic resonance imaging scanners as well. There may also be a need to determine appropriate routes of transport for these patients, as some hospitals may not have been designed to accommodate bariatric patients in all areas of the physical plant.
Patient Selection
Similar to other bariatric surgical procedures, sleeve gastrectomy patient selection is vital to long-term successful weight loss. As with adult patients, attempting a medical weight-loss trial for a period of greater than 6 months is a necessary qualifying factor for most if not all insurance companies. 15 This is despite a lack of data supporting its importance in the ultimate surgical weight-loss outcome. Even if patients are unsuccessful during this time frame, the weight-loss trial may aid in educating patients and their families on the dietary and lifestyle changes that are important to long-term postsurgical success. In addition to a medically supervised weight-loss trial, patients should also undergo a formal psychological assessment. 15 The evaluation actively determines if the patient's understanding of the long-term implications of the surgical procedure is adequate or if the patient suffers from any undiagnosed or untreated psychological disorders. Prior to any surgical intervention, candidates should undergo a thorough medical evaluation to ensure patient safety during the surgical procedure. A through medical assessment includes a complete history and physical evaluation with a focus on screening for undiagnosed, obesity-related comorbidities. Particularly common comorbidities are: type II diabetes, hypertension, sleep apnea, and metabolic syndrome. Candidates should undergo a sleep study to rule out obstructive sleep apnea prior to receiving general anesthesia. If the candidate is diagnosed with obstructive sleep apnea, the sleep apnea should be treated (usually requiring a fitting for a continuous positive airway pressure (CPAP) mask and a CPAP titration study), and an echocardiogram should be performed to rule out left ventricular hypertrophy or heart strain. 16
Technical Aspects of the Procedure
Specific technical aspects of the operative procedure vary by surgeon. However, there are some essential portions of the procedure that must be performed to ensure success. An expert panel has been developed to achieve consensus on all key aspects of the operative procedure in an attempt to standardize the operation. 13 During the operative procedure, patients undergoing the sleeve gastrectomy are placed in reverse Trendelenburg, and access is gained to the abdominal cavity through four or five trocar sites (the exact number of trocar sites differs by surgeon). The liver is retracted to expose the operative field clearly, and most importantly the gastro-esophageal junction. The fundus of the stomach is mobilized and a gastric tube ranging from 32 to 40 French (some use bigger) is inserted down the esophagus and into the stomach along the lesser curvature. This tube it utilized as a guide during the gastric dissection and to ensure that the remaining stomach after the resection is not too small. A linear reticulating stapler is used in resecting a portion of the stomach creating a long, tubular-shaped stomach, which preserves the pylorus (see Fig. 1).11–13,17 The stomach to be removed is usually placed in a bag and removed via one of the port sites. The staple line is checked using one of several methods, and as long as there is no leak from the stomach remnant, the trocars are removed and the abdomen is closed. The operation usually takes less than 3 hours, and most patients can recover on a surgical floor without the need for an ICU stay. On average, patients stay one or two nights in the hospital and are discharged to their home thereafter.
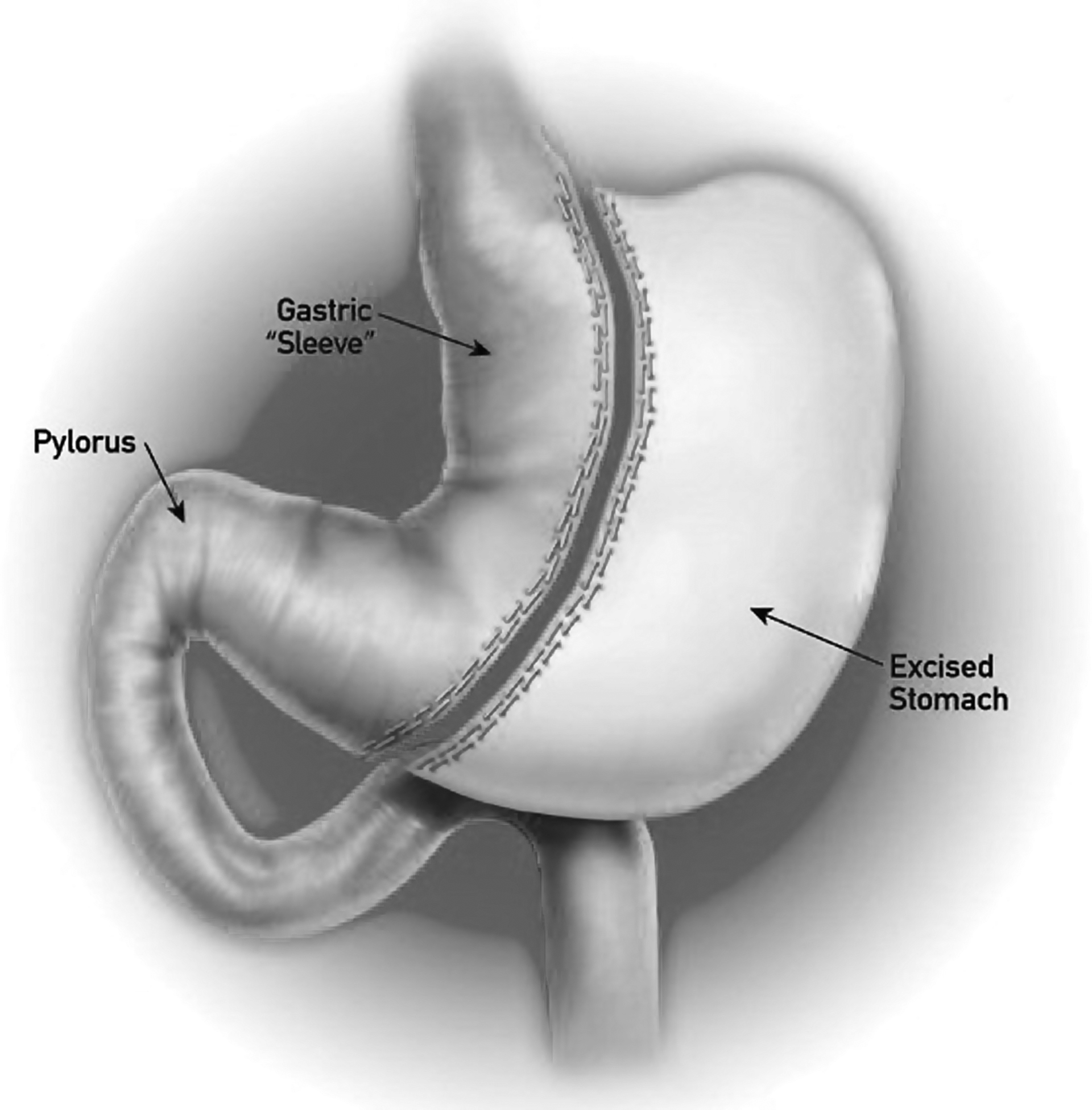
Sleeve gastrectomy.
Role of Nursing Care
Nurses play a critical role in the care of sleeve gastrectomy patients, both in the preoperative and postoperative phase. Nursing care of patients undergoing sleeve gastrectomy must be comprehensive, and nursing expertise in patient education makes them well suited to provide patients and families with nutritional support and anticipatory guidance throughout the process. In the acute postoperative phase, nurses are skilled to manage the monitoring and education that is needed by the patient. In addition, the compassion and caring that is unique to the nursing profession allows nurses to excel in the care of patients with this complex medical and psychological disorders associated with obesity.
Invaluable nursing roles in the care of adolescent sleeve gastrectomy patients include education and support of both the family and patient. Essential educational topics include appropriate expectations for the surgery and the immediate postsurgical period, potential weight loss, dietary changes necessitated by the surgical procedure, and postoperative activity goals.
An important aspect of sleeve gastrectomy success is the adaptation of postsurgical dietary requirements. By educating the patient on these dietary changes and setting realistic expectations, nurses are able to facilitate patient adherence to their preoperative and postoperative diets. Nurses are particularly impactful in encouraging success by educating the patient on the importance of the 2-week preoperative liquid diet, a protein-sparing modified fast. Depending on the nurses' comfort level, this can be completed in conjunction with a dietitian. Preoperative diets for bariatric procedures vary, but consist of high-protein, low-fat beverages. The preoperative diet is effective in shrinking the liver, making the operational procedure less problematic and reducing operative risks. 18 Immediately prior to the procedure, nurses in conjunction with surgeons should ensure all patient questions regarding the procedure have been adequately addressed.
Immediately following the sleeve gastrectomy, patients are usually transferred first to a post-anesthesia care unit (PACU) and then to a surgical care floor. Occasionally a patient with uncontrolled diabetes or hypertension or severe obstructive sleep apnea may require an intensive care unit (ICU) stay. In order to assure comfort and safety, nurses must be prepared with appropriately sized equipment for the patient and their family. Close monitoring of the patients in the postoperative period is aided by the use of a bedside cardio-respiratory monitor. Vital signs are to be checked and documented according to hospital protocol. It is essential that nurses pay close attention to changes in vital signs, as the patient's physical exam is unlikely to be reliable. Tachycardia, fever, and shortness of breath can be indicative of a staple-line leak, and the patient's provider should be notified immediately. In fact, tachycardia alone is an ominous sign and should not be overlooked or written off as merely inadequate pain control.
In the immediate postoperative period, the patient is not permitted to eat or drink. Nurses should adequately monitor intake and urine output, as hydration is maintained with intravenous fluids. It is important that urine output be calculated based upon the patient's ideal body weight and not their true body weight. Many centers will perform a contrast study on day 1 after surgery before the patient is allowed to drink fluids.
Initially, pain is controlled via intravenous pain medications, and as always pain control is monitored via hospital protocol. An effective pain-control regimen utilized in the adolescent population consists of around the clock intravenous acetaminophen, intravenous ketorolac, and intravenous morphine as needed for breakthrough pain. Minimizing the narcotic use can aid in preventing apneic episodes and overall respiratory complications, but adequate pain control is essential for early ambulation which is also critically important. Nurses should communicate with ordering physicians and pharmacy staff to ensure that medication doses are appropriate and adequate for the patient's weight, and that the right weight (ideal or actual) is used to calculate the dosing depending on the medication.
Nurses must be aware of increased risk for deep venous thrombosis in this patient population. It is imperative that patients be started on anti-coagulant therapy in the operating room. An effective protocol consists of body mass index-dependent dosing of low molecular weight heparin injected subcutaneously every 12 hours. Nurses should encourage patients to utilize sequential compression devices, often in addition to the pharmacologic agent. While sequential compression devices that wrap around the patient's lower extremities are common and therapeutic, they can be uncomfortable for patients in this population. This discomfort often leads to poor compliance and the devices are often discontinued. Foot sequential compression devices tend to cause less discomfort, and therefore result in better compliance. Patients should be encouraged to ambulate early in their postoperative course. The assistance of a nurse or physical therapist is important until it is clear they are able to ambulate alone safely.
Once a patient is started on an oral diet, they should initially be given a fluid restriction to encourage slow, consistent oral intake. Patients are not allowed to drink sugar-sweetened beverages. To minimize any additional abdominal discomfort, patients should not use straws or drink carbonated beverages. Close attention to patient's intake and output becomes more crucial, as it indicates when the patient is tolerating adequate liquids for discharge. In addition, the provider should be notified of any emesis or inability to control secretions, as this can be indicative of postoperative edema of the stomach remnant that may necessitate additional therapy prior to starting oral intake.
Some patients can go home on postoperative day 1 if they have adequate pain control, are tolerating enough oral intake (usually about 120 mL of fluid an hour), and can safely ambulate. If the patient does not meet these criteria on day 1, on postoperative day 2 increased oral intake and ambulation should be encouraged; vital signs and wounds should be closely monitored, and the patient should be prepared for discharge. Once the patient is able to be advanced to the goal intake of 120 mL an hour and the pain medications are transitioned to an oral format, the patient is safe for discharge. Patients can be discharged on liquid oxycodone in addition to liquid or chewable ibuprofen or acetaminophen. Patients should restart their preoperative medications, but they should not take any medications in a pill form. These medications should be transitioned to liquid or chewable. In addition, patients are started on a daily chewable multivitamin. This multivitamin should be continued throughout the patient's life, and nurse education must stress the importance of adherence to the daily vitamin prior to discharge.
The nursing educational role is imperative in preparation for the patient's discharge. Nurses should review the postoperative diet and discuss the importance of hydration with the patient. Of particular importance, nurses should emphasize the need to sip small frequent amounts of water. The patient is educated on signs of dehydration and when to seek further medical care. Patients should be instructed to return to the hospital or contact the office with any signs of wound infection, vomiting, increasing pain, or fever.
Expected Outcomes
After discharge from the hospital, patients return for an initial postoperative appointment within 2 to 3 weeks. At this appointment, patients are assessed for wound healing and are often progressed to the second stage in their postoperative diet—pureed foods. Once again, at this appointment the role of the nurse in patient education and encouragement is critical. Nurses educate patients about the foods that are permitted in stage two of the diet, reinforcing the importance of high-protein foods. Patients are also instructed to drink adequate amounts of water and to pay particular attention to internal cues of satiety. Food and liquid intake are separated until 3 months after surgery, and this point should also be stressed by the nurses involved in the patient care.
Patients are followed postoperatively every 3 months for a period of 1 year and every 6 months or annually thereafter. At the first postoperative visit, patients are encouraged to re-engage in a medical weight-loss clinic. These clinics provide patients with continued nutritional counseling and encouragement to meet weight loss and activity goals. Despite previous body habitus limitations, patients are encouraged to engage in a physical activity routine. Initially, patients are to be encouraged to walk and begin strength training. As patients begin to lose weight, they should increase their aerobic activity while continuing resistance training, especially of their upper body. This may help minimize sagging skin as weight loss ensues. In order to maintain adherence to an exercise routine, patient's activity is focused on areas that they inherently enjoy. Encouraging team sports also helps teens formalize an exercise routine.
The potential for nutritional deficiencies should be addressed at follow-up visits if patients exhibit symptoms. Compliance with the multivitamin and other daily medications is to be evaluated at every visit. Nutritional labs studies, lipid profiles, and blood glucose should be drawn at baseline and compared to lab work obtained at a maximum of 1 year after surgery. Some prefer to monitor laboratory values earlier in the postoperative course.
Continued psychological evaluation and treatment through the weight-loss process is important for adolescent patients. Patients are guided on how to address emotional stressors adequately and the changes they experience in their lifestyle and eating habits. The nurse's role can be vital in augmenting the psychological support provided by the clinical psychologists and the patient's own support system.
Finally, patients are encouraged to continue following up with all subspecialty providers, as a patient's medical needs may change with dramatic weight loss. Frequently, patients no longer require insulin-sensitizing medications such as metformin, lipid-lowering medications, or anti-hypertensives. Providers counsel female patients with polycystic ovary syndrome about the return of ovulation with weight loss; safe sex practices should be reinforced. In our experience, adolescents after sleeve gastrectomy procedures can expect an excess weight loss of approximately 40% with no significant operative complications. Further, initial data show a decrease or resolution in patient comorbidities. 9
Summary and Conclusions
Obesity in adolescents continues to rise in the United States, presenting unique care challenges for today's pediatricians. For the morbidly obese adolescent, bariatric surgery is an opportunity to obtain a healthy lifestyle and possibly increase their lifespan. The sleeve gastrectomy has been shown in the adult population to be a safe procedure that results in weight loss and reversal or improvement of comorbidities. Thus far these results have been confirmed in the adolescent population, but the data are still fairly new. We believe that the sleeve gastrectomy is an attractive first procedure for the morbidly obese adolescent.
Footnotes
Disclosure Statement
No competing financial interests exist.