
Abstract
Bariatric sleeve gastrectomy patients have 75% of their stomach removed, reducing the stomach volume and parietal cell mass, leaving a narrow gastric tube/sleeve. The parietal cell mass secretes hydrochloric acid and intrinsic factor, which are necessary for vitamin B12 absorption. A review of the literature indicates that a reduction in parietal cell mass could lead to a decline in serum B12 levels. A total of 72 sleeve gastrectomy patients between January 1, 2005, and December 31, 2007, were reviewed. Data collected by retrospective review until December 21, 2008, included gender, age, date of surgery, vitamin B12 supplementation, and serum B12 levels before and after surgery. Of the 72 patients, 27 patients were on B12 supplementation (38%) and 45 patients were not on supplementation (62%). Of the 45 patients not on supplementation: 24 had no postoperative B12 labs (53%), and four had no preoperative labs (9%). Seventeen (38%) had both pre- and postoperative B12 labs. The latest postoperative labs were reviewed from 0 to 39 months from date of surgery. Results of the 17 patients, using a paired t-test, showed that the average latest postoperative B12 level was 350 pg/mL±103 (247–453) compared to the average preoperative level of 394 pg/mL±148 (246–542) (p=0.04). Although B12 values were still within normal range, the study showed decline, which increases risk of nutritional deficiency over time with resultant irreversible neurological damage. A Pearson correlation demonstrated a negative trend, but it is not significant due to the small sample size. This study suggests that B12 labs should be performed routinely pre- and postoperatively. Further tests could be warranted to delineate a true B12 deficiency.
Introduction
Patient with higher BMIs (65 and above, depending on surgeon preference) or those who are at risk for a longer operative time due to heart or lung comorbid conditions often have a staged procedure. 2 These high risk patients undergoing Roux in Y would first receive the sleeve gastrectomy.2,3 The final staged procedure, which is the completion of the Roux en Y, is then performed 12–18 months later when the patient has achieved weight loss adequate to decrease their anesthesia risk.2,3
Approximately 8–10 years ago, bariatric surgeons began to notice that many sleeve gastrectomy patients lost a significant amount of weight and did not require the second stage. 4 Patients may lose between 40% and 70% excess weight loss with the sleeve gastrectomy and experience resolution of comorbidities such as diabetes, hypertension, obstructive sleep apnea, and dyslipidemia. CCHS is also using the sleeve gastrectomy in patients with diabetes who have a BMI between 30 and 40 kg/m2 as part of a clinical trial to determine improvement in diabetes management in comparison to the Roux en Y surgery and medical nutrition therapy. Currently, long-term studies of patients who underwent sleeve gastrectomy procedure are not available. 4
Sleeve gastrectomy patients have approximately 75% of their stomach resected, leaving a narrow gastric tube or sleeve. The line of resection begins at the antrum and is extended toward the angle of HIS.2,3 The result is a lesser curve gastric tube excising the fundus and greater curvature of the stomach. 3 See Figure 1 for illustration of the sleeve gastrectomy. The fundus and body of the stomach contain the parietal cells whose function is to secrete hydrochloric acid (HCL) and intrinsic factor (IF), both of which play a role in the body's ability to absorb vitamin B12. HCL is needed to maintain a sufficiently acidic environment for pepsin, another gastric secretion, to release vitamin B12 from food. IF is secreted by parietal cells to bind with vitamin B12 so that it can be absorbed in the intestine later in the digestive process.5,7

Illustration of the sleeve gastrectomy.
There is not enough research on patients who underwent the sleeve gastrectomy at the time of this study to determine which vitamin and mineral are of concern. Vitamin B12 would appear to be a concern in the sleeve gastrectomy patient due to the excision of the body of the stomach and fundus where the parietal cells are located and whose function is necessary for vitamin B12 absorption. Studies have demonstrated multiple vitamin/mineral deficiencies with bariatric surgery, including vitamin B12 with the Roux en Y surgery.8–10 Vitamin B12 deficiencies have also been demonstrated in post gastrectomy patients.11–13 These studies have shown that vitamin B12 malabsorption can result from the absorptive process being disrupted.11,13
Vitamin B12 absorption requires various steps. The vitamin B12 found naturally in foods is bound to proteins. Vitamin B12 is released from the proteins in the stomach by gastric enzymes, which require an acidic pH.5,14 Once the B12 is freed from these proteins, it is re-bound to R proteins in the stomach, which carry this B12-R complex to the duodenum.5,14 In the duodenum, proteases digest R protein and release the B12. B12 is then bound to IF, a protein synthesized by gastric parietal cells. IF is secreted in response to various factors such as consumed food and gastrin.5,14
This B12-IF complex is necessary for B12 absorption. IF protects B12 from breakdown due to intestinal bacteria in the terminal ileum where B12 is absorbed when recognized via the B12-IF complex.5,14 Any disturbance along this absorption process may result in a B12 deficiency.5,14
Methods and Subjects
The study received approval from the Cleveland Clinic Institutional Review Board (IRB).
Patients who received the gastric sleeve surgery from January 1, 2005, through December 31, 2007, were identified from the Remedy MD database, which is maintained by the Bariatric and Metabolic Institute of the Cleveland Clinic Foundation. It is a relational database that interfaces with the patients' medical record and is used to capture surgical encounters and subsequent ambulatory care office visits.
Investigators reviewed the identified patient records to collect data on gender, sex, age, date of surgery, and vitamin B12 supplementation and serum vitamin B12 levels, before and after surgery. The sample size consisted of 72 patients (53 females, 19 males). The age ranges of the patients were between 28 and 70 years of age.
The objective of this study was to assess whether the sleeve gastrectomy affected serum vitamin B12 levels postoperatively. Therefore, subjects without serum B12 levels available pre- and postoperatively and those patients who were already receiving B12 supplementation were excluded from the study. Figure 2 demonstrates the distribution of the study patients in the selected time frame who did or did not receive B12 supplementation. Of the 72 patients reviewed, 27 patients who received supplementation before or after surgery were excluded from the study. Of the remaining 45 patients, four patients without a B12 value preoperatively and 24 patients without a serum B12 value postoperatively were excluded. The resultant sample, then, contained 17 patients with serum B12 levels collected both pre- and postoperatively, and who were not supplemented. These serum B12 levels were then compared to evaluate the potential differences, if any, of the sleeve gastrectomy surgery procedure on B12 levels.
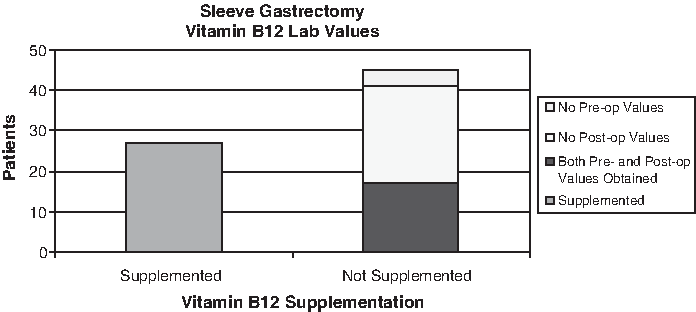
Distribution of patients regarding vitamin B12 supplementation and lab values.
Statistical Analysis
The sample size was based on those patients who received the gastric sleeve surgery from January 1, 2005, to December 31, 2007, who had not received vitamin B12 supplementation and had both pre- and postoperative serum B12 levels. The analysis was performed on 17 patients who met the criteria. The final cohort evaluated comprised five males and 12 females with an average age of 47.5 years (range 28–70 years of age), with eight patients being over the age of 50 years of age and with an average BMI of 66.8 kg/m2 (range 40.4–113).
The latest postoperative serum B12 level was compared to the preoperative level. This was decided due to the inconsistent time frame that the postoperative values were obtained. The time frame ranged from 3 months to 39 months postoperatively. Results of the 17 patients, using a paired t-test, showed that the average postoperative serum B12 level was 350 pg/mL±103 compared to the average preoperative level 394±148. The difference of 44 pg/mL is statistically significant according to a calculated p-value of 0.04. A Pearson correlation demonstrated a negative trend between pre- and postoperative surgical values, and was insignificant due to the small sample size. See Figure 3 for pre- and postoperative latest vitamin B12 values and average of data. All data were analyzed using SPSS for Windows (v17.0, 2008, SPSS, Chicago, IL).
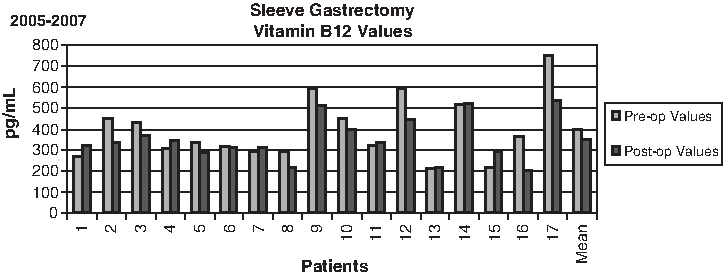
Pre- and latest postoperative vitamin B12 values and average B12 value.
Discussion
The sleeve gastrectomy procedure, which removes 75% of the stomach with resultant fundus and body of the stomach excised, can put patients at risk for vitamin B12 deficiency. Potential deficiency is due to the body's inability to absorb vitamin B12 adequately after the procedure is performed. This study suggests that the sleeve gastrectomy may have an adverse effect on serum B12 levels, as more patients had lower serum vitamin B12 levels after surgery compared to preoperative levels.
Hematologic, neurologic, and psychiatric conditions can manifest as a result of vitamin B12 deficiency.2,7 Hematologic concerns include megaloblastic anemia and pancytopenia. Neurologic events like peripheral neuropathy may be irreversible. Other adverse symptoms include lassitude, fatigue, chills, dizziness, and depression.2,7 Vitamin B12 deficiency is difficult to assess due to the fact that the serum values may be normal (normal values are 200–900 pg/mL), although the patient may manifest the abovementioned symptoms. Studies have shown that between 50% and 80% of patients have had B12 deficiencies even with a normal B12 level. 7 A more sensitive screening tool is methylmalonic acid, which will increase earlier in the deficiency compared to serum B12 levels.2,7,12 Another concern is that vitamin B12 levels decrease with age due to atrophic gastritis, and the increased use of gastric acid blocking agents may also play a role in B12 deficiency. Therefore, gastric sleeve surgery, being aged 50 years or older, and the use of gastric blocking agents may all play a role in vitamin B12 deficiency.5,7
Conclusion
The protocol for sleeve gastrectomy patients may benefit from inclusion of serum vitamin B12 levels both before and after surgery. To assess vitamin B12 absorption during the first year after surgery, a level obtained at 6 months and annually thereafter may be beneficial. If a vitamin B12 deficiency is suspected, additional testing of methylmalonic acid can determine if it is a true deficiency. Limitations of the study were, first, the small sample size. Second, older patients aged 50 years or older may have confounded the study because of their risk for vitamin B12 deficiency due to the increased presence of atrophic gastritis. The third limitation was the study's large time span of postoperative values. Additional research is needed to review a larger sample size and to assess further the effect of the sleeve gastrectomy on vitamin B12 absorption.
Footnotes
Disclosure Statement
No competing financial interests exist.