
Abstract
Significant benefits of bariatric surgery for morbidly obese individuals have been widely reported in the literature. Research interests represent a wide range of perspectives aimed at investigating a variety of clinical, economic, functional, and quality of life (QOL) outcomes. As a highly personalized and multidimensional construct, QOL has been identified as the most significant outcome of bariatric surgery. 1 QOL studies are now well reported in the literature. However, these have been limited to quantitative designs, use a wide variety of measurements that conceptualize QOL differently, and report divergent results. Few studies have explored QOL as a holistic state from the patients' perspective or examined it beyond the first postoperative year. Consequently, long-term QOL remains an elusive phenomenon despite scientific consensus on its importance as a health outcome of bariatric surgery. Discovering its subjective meaning will help inform surgical decisions and improve the course of postoperative care. Toward that end, this study employed a qualitative approach to explore the phenomenon of QOL. Using focus group methods, the study aimed to describe the meaning of QOL from the subjective experiences of individuals who had weight reduction surgery more than 2 years ago. Colaizzi's phenomenological method was used to analyze data that yielded a rich description of seven themes that form the meaning of QOL to study participants. The study lays the descriptive groundwork for a broader program of research to improve care of bariatric surgery patients.
Introduction
The research base has grown exponentially over the past decade, with studies examining outcomes from several divergent streams of thought. A newer generation of research focuses on clinical effectiveness from a patient perspective, rather than a provider view, defining it as improvements in the quality of life (QOL). 3 QOL is viewed by many as the ultimate goal of bariatric surgery that should not be neglected in bariatric outcome studies. 1 A solid research base now attests to the effectiveness of bariatric surgery in improving the QOL among individuals in the first few years following surgery.4–7 These studies reveal a more holistic definition of health, studying surgical outcomes as a lifelong and evolutionary condition rather than an endpoint following a medical intervention.
However, there is a significant lack of consistency in how QOL is defined and operationalized with numerous instruments used to measure it. Questions arise about the theoretical and conceptual clarity of these studies and the content validity of measurement tools that limit use of their findings.1,8 Further, studies are needed that explore the meaning of QOL over time to acknowledge the life-altering effects of surgery. Many studies still report results in the short term. Exploring this phenomenon among those who are at least 2 years postoperative will allow investigators to describe factors other than weight loss that may influence QOL years after surgery. Given its potentially life-altering health consequences, it is essential to investigate the long-term implications with a view toward the holistic nature of health and well-being. While longer-term studies have begun to appear in the literature, many of these are confounded by population differences and design and measurement variations.
Finally, as a subjective and context-bound phenomenon, QOL can be better understood when studied from the individual's perspective. This approach will address issues of conceptual confusion generated by findings derived from the range of generic and disease-specific instruments used to measure QOL. Designed through that lens, studies would reflect a more integrative view of health outcomes that resonates with the values and beliefs undergirding the nursing profession.
The aim of this study, then, is to explore the meaning of QOL over the long term from the perspective of patients who have experienced weight loss surgery. There were two research questions:
RQ1: What is the meaning of QOL among individuals who had bariatric surgery more than 2 years ago?
RQ2: What factors, if any, influence the QOL for these patients over their postoperative course?
Review of the Literature
The literature reporting on outcomes of bariatric surgery fall into five categories based on the dependent variable(s) being addressed in the study: (1) clinical effectiveness studies, (2) QOL studies, (3) cost effectiveness studies, (4) psychosocial outcomes, and (5) a combination of outcomes. The literature review for this study focused on QOL as an outcome of weight loss surgery.
Morbidly obese individuals face multiple obstacles in their daily living that can have a profound effect on general QOL. Savik et al. 9 conducted a randomized parallel-group trial across two medical centers. QOL outcomes based on Short Form-36 Health Surveys indicate that patients who had either gastric bypass surgery or duodenal switch procedures had improved scores at 2 years after surgery. One prospective study 10 found that there was marked improvement in QOL among 379 patients who had laparoscopic Roux-en-Y gastric bypass (RYGBP) for morbid obesity 5 years after surgery based on Bariatric Analysis and Reporting Outcome System (BAROS) scores. Conversely, another study examining long-term outcomes of laparoscopic surgery using a different technique (laparoscopic adjustable gastric banding referred to as LAGB) found neutral results on QOL scores using BAROS among patients who had surgery at least 12 years earlier. 11 However, findings reported by Schouten et al. 12 found impressive QOL improvements at 1 year for LAGB and vertical band gastroplasty (VBG) patients that were sustained at 7 years, especially for the LAGB population. Yet, the study employed other QOL measures that included select domains from the Nottingham Health Profile (NHP-I and II) and the Sickness Impact Profile (SIP).
Most studies that address QOL outcomes also measure a variety of clinical, social, mental health, and economic measures as dependent variables. Outcomes such as cardiovascular risk, 9 cardiorespiratory fitness, 13 upper gastrointestinal symptoms, 14 diabetes,15,16 sleep apnea, arthritis and hypertension, 17 and cost,18–20 as well as changes in weight and body mass index (BMI) have been examined along with QOL. However, results are generally presented as isolated outcomes with few studies analyzing the interplay of variables or their effect on QOL. One systematic review 21 investigated the predictive value of psychosocial variables, including QOL, on weight loss and mental health after obesity surgery. Results of the meta-analysis showed that obesity surgery improved both medical and psychosocial outcomes variables. Investigators concluded that QOL, where medical, psychosocial, and psychological variables merge, and its association with postoperative weight loss could not be determined.
A few studies were found that were single focused, measuring only post bariatric surgery QOL. Lier et al. 4 found an association between pre- and postoperative psychiatric disorders and health-related QOL (HRQOL) measured using the Short Form 36 (SF-36) questionnaire. Follow-up was limited to 1 year post surgery. Positive changes in QOL and body image were reported by Sarwer et al. 5 at 20, 40, and 92 weeks after gastric bypass surgery. Most improvements were seen in the first few postoperative months. A 1 year follow-up prospective study of 102 RYBG patients found improvements in physical, psychological, and social domains of the World Health Center Quality of Life Brief (WHOQOL-BREF). Another study hypothesized that greater impairments in QOL would encourage patients to choose more invasive surgeries for weight loss. 22 Researchers used three different QOL tools with results gained from analysis of variance. Patients had moderate to severe preoperative QOL impairments compared to community norms but scored similarly on QOL measures regardless of their choice of three surgical procedures. Another QOL project was a population-based cohort study conducted by Batsis et al. in the United States 6 that used a different set of three QOL instruments. Follow-up scores were collected at 4 years post surgery. Investigators reported that profound weight loss, depression treatment and absence of medical comorbidities appear to predict better QOL and functional status. Others report similar significant improvement in QOL using still other instruments for data collection.7,13
As evident in this review, studies have used a wide range of standardized and nonstandardized tools that vary widely in how they define and to examine QOL. Table 1 provides examples of various tools used in QOL studies. Instruments define QOL in terms of functional status (SF-36), self-esteem, 23 personality inventory, 21 depression, and work history. Both generic QOL instruments (HRQOL) 24 and disease-specific measures (BAROS) 25 have been used. A few studies have examined the sensitivity of QOL instruments in detecting changes following surgical intervention. However, results have failed to show consistency in reported outcomes. 3
QOL, quality of life.
To summarize, while there is significant evidence that an individual's QOL is profoundly affected by morbid obesity and improved through surgical intervention, shorter-term, quantitative studies have dominated and vary significantly in how they conceptualize and measure it. While recent studies suggest that QOL may fluctuate over the long term, they fall short of describing the emergence of trends and patterns over time. Similarly, findings indicate that several confounding factors influence both pre- and postoperative QOL, but these remain undefined and underinvestigated. Other limitations surface in studies that rely on small samples, limit follow-up to the first few postoperative years, and/or are conducted in culturally diverse locations, limiting their generalizability.
Finally, there is a glaring lack of nursing research to inform understanding of what QOL means to patients before and after weight loss surgery. Yet, as Sutton and Raines note, nurses are uniquely positioned to advocate for care that addresses the well-being of the whole person. 26 Studies are needed that employ the holistic view of health and wellness held by the nursing profession and lead to greater understanding of QOL as a subjective phenomenon of interest to nurses.
Methods and Materials
A qualitative research approach was chosen for three reasons. First, the qualitative paradigm supports the discovery of knowledge about complex, unexplored, or underdeveloped phenomena that still await concept clarification and theoretical development. QOL following weight loss surgery fits this criterion. Second, qualitative design is helpful in eliciting highly detailed and complex descriptions of what QOL actually means to those whose lives have been altered by the surgery. To date, there have been no purely qualitative studies exploring this phenomenon from patients' perspective. Third, a qualitative design allows for the discovery of associations between QOL and variables assumed to influence it as suggested in the literature.
This is a descriptive study designed from a phenomenological perspective. Simply put, phenomenology is the study of a phenomenon, or how things appear from the perspective of those who are experiencing it in their “life world.” 27 As a method of inquiry, it relies on subjects (the research participants) to use their own words, understandings, and personal experiences to describe and provide clarity about a phenomenon. Phenomenologists want to know what the experience was like to live it, not just the person's reaction to the experience. 28 Thus a phenomenological stance allows the researcher to study the meaning of an experience as it was lived by individuals, lending to rich description that goes beyond taken-for-granted accounts of it.
Design
The study used focus group methods for data collection. As a research method, focus groups have gained widespread acceptance among social science researchers as a primary, supplementary, or complimentary source of data for qualitative studies. 29 Focus groups were chosen in order to maximize representation from the bariatric surgery population. They provide an opportunity for the researchers to pose broad guiding questions that facilitate participants' ability and willingness to share their understanding of the phenomenon.
Focus groups are essentially group interviews. One distinguishing factor is their reliance on the interaction among group members as the catalyst for generating new insights and descriptions that might not emerge during individual interviews. Focus groups can be especially useful to collect data on more sensitive topics because they can provide a safer, more accepting environment for highly personal discussions. That was an important design consideration given the study's intent to explore highly personal feelings and experiences of individuals who have frequently experienced social isolation and rejection. A unique characteristic of focus groups is that participants are deliberately assigned to groups with others who share similar experiences. Homogeneity allows for more free-flowing conversation and facilitates analyses that examine the perspectives of different subgroups. 29
The research team followed Morgan's guidelines and recommendations for planning and conducting the focus groups. The first step was to categorize different subgroups in the study population based on age, gender, and years since surgery. This process is called segmentation. It allows the researcher to control the group composition carefully to achieve homogeneity. Based on the overall demographics of the potential population, the team segmented the focus groups into five categories as shown in Table 2. Ten focus groups were scheduled to offer participants more flexible options for joining. Each group was scheduled for 90 minutes as suggested by Morgan. Ultimately, seven focus groups were conducted.
Setting
A single site design was selected for three reasons. First, it allowed investigators to capitalize on the collaborative relationship and support they have with a surgeon affiliated with the institution. His support facilitated access to a database of 1,200 patients as potential recruits for the focus groups. Second, the site has been designated as a Bariatric Center of Excellence by the national Surgical Review Corporation, reflecting the setting's adherence to highest standards of care. Third, one surgeon has performed all of the weight loss surgeries in the same hospital where a specialized team of RNs provided care for these patients on a dedicated unit. This minimized variations in practice and practitioners that might confound results. All focus group sessions were held in the same comfortable hospital classroom setting that was familiar to participants who had attended education sessions there before surgery.
The interview guide
Morgan supports the four criteria proposed by Merton 30 for conducting effective focus group interviews. Discussion topics were translated into a semi-structured questioning guide to channel group interaction and allow comparisons across groups. Recommendations by Spradley 31 led to development of grand tour and follow-up questions intended to probe, clarify, and expand participants' responses.
Sample
A convenience sample was recruited from the roster of eligible patients who had weight reduction surgery from 2000 through 2009. All patients who had any type of weight loss surgery (gastric by-pass, laparoscopic banding) were invited to participate, representing a population of approximately 1,200 patients. Letters of invitation were sent to 853 eligible patients via regular mail by the surgeon who had permission from his patients to contact them for future study involvement. This procedure protected their rights to privacy as defined by Health Insurance Portability and Accountability Act of 1996 (HIPPA) and provided the nursing research team with access to a rich sample. As a recruitment incentive, each individual who attended a focus group was given a 25 dollar gift card supported with nursing research funds from the hospital. A study fact sheet describing the study and informing potential participants of their rights and freedom to consent was attached. Study investigators did not have access to patient names, addresses, or any other identifying information prior to voluntary enrollment in the study.
A total of 61 individuals participated in the study. Focus groups were limited to between 10 and 12 participants. Patients who had complications following surgery were not excluded in order to capture the full range of patients' postoperative experiences. Non-English speaking patients were excluded from the study. The organization's Nursing Research Council and Institutional Review Board approved the study proposal.
Data collection
At the start of each session, the facilitator reviewed privacy and confidentiality procedures and asked participants to complete an anonymous demographic form voluntarily. The intent was to collect self-reported information about participants' age, gender, date and type of surgery, occurrence of any postoperative complications, and overall weight loss. Facilitators used scripted opening and closing remarks and the interview guide to conduct the focus groups. Each session was audiotape recorded. The tape recordings were transcribed verbatim and scrubbed of identifiers by a trained administrative assistant. Individuals were referred to as “Participant 1,” “Participant 2,” ansd so on, or simply “a participant” when names were eliminated. Transcriptions were kept locked. Each was copied and circulated among research team members who kept them confidential once the data analysis phase began.
Data analysis
The research team analyzed data following Colaizzi's phenomenological qualitative method. 32 Colaizzi's approach offers a structured and systematic framework of seven steps for completing a complex analysis of phenomenological data. These steps are summarized in Table 3. Analysis was planned as a rigorous, dynamic, iterative process to ensure its credibility, dependability, confirmability, and transferability of findings as recommended by Lincoln and Guba. 33 It involved reading and rereading transcripts individually and collectively to identify meaningful statements, cluster similar ideas, and uncover emerging themes to answer the research question. Thematic analysis was supported by direct quotations from the focus group transcripts. The research team reviewed transcriptions both individually and during a series of meetings to build consensus on emerging themes. A large table in a dedicated space facilitated organization and categorization of the data as quotes from across focus groups were identified, categorized, reorganized, and clustered. Periodically, team members needed to regroup, document what they were thinking, seeing, and feeling about the data, and question again the analytical decisions made at previous meetings. This process was important to sustain rigor in analyzing data. It helped to reduce potential researcher bias, prevented premature closure, and kept the focus on ensuring the trustworthiness of the data.
A total of 401 significant statements were color-coded on index cards. These were initially stacked into six categories of statements that defined QOL across the perioperative trajectory. Data indicated that QOL has both positive and negative aspects and includes physical, psychological, and social dimensions as an expression of one's health. Further analysis led to expansion of the six categories into 19 statements of formulated meanings. Ultimately, these converged into seven emergent themes to define QOL. A secondary analysis 6 months later led to team consensus on the essential structure of the construct.
Results
Demographic information describing study participants is presented in Table 4. A total of 61 post bariatric surgery individuals participated in seven focus groups conducted over a 2-month period.
Most individuals had undergone gastric bypass surgery (72%) with the remainder having laparoscopic banding procedures. All stated that they had lost “significant weight.” Nine participants reported having experienced postoperative complications (14.7%). However, these were described predominantly as symptom management problems rather than surgery-related clinical complications. Most participants were married or identified a significant other in their lives (69.5%). Six individuals were divorced. However, participants did not report if they were divorced after surgery. The majority were employed (70.5%) at the time of the study.
Seven themes as the essential structure of QOL
Seven themes emerged to define the meaning of QOL among post bariatric surgery patients. Data supported their presence in every focus group, regardless of participants' gender, age, surgical procedure, or postoperative status. These themes arose as distinct but interrelated constructs that formed the essential meaning structure of the phenomenon QOL. Figure 1 illustrates these themes.
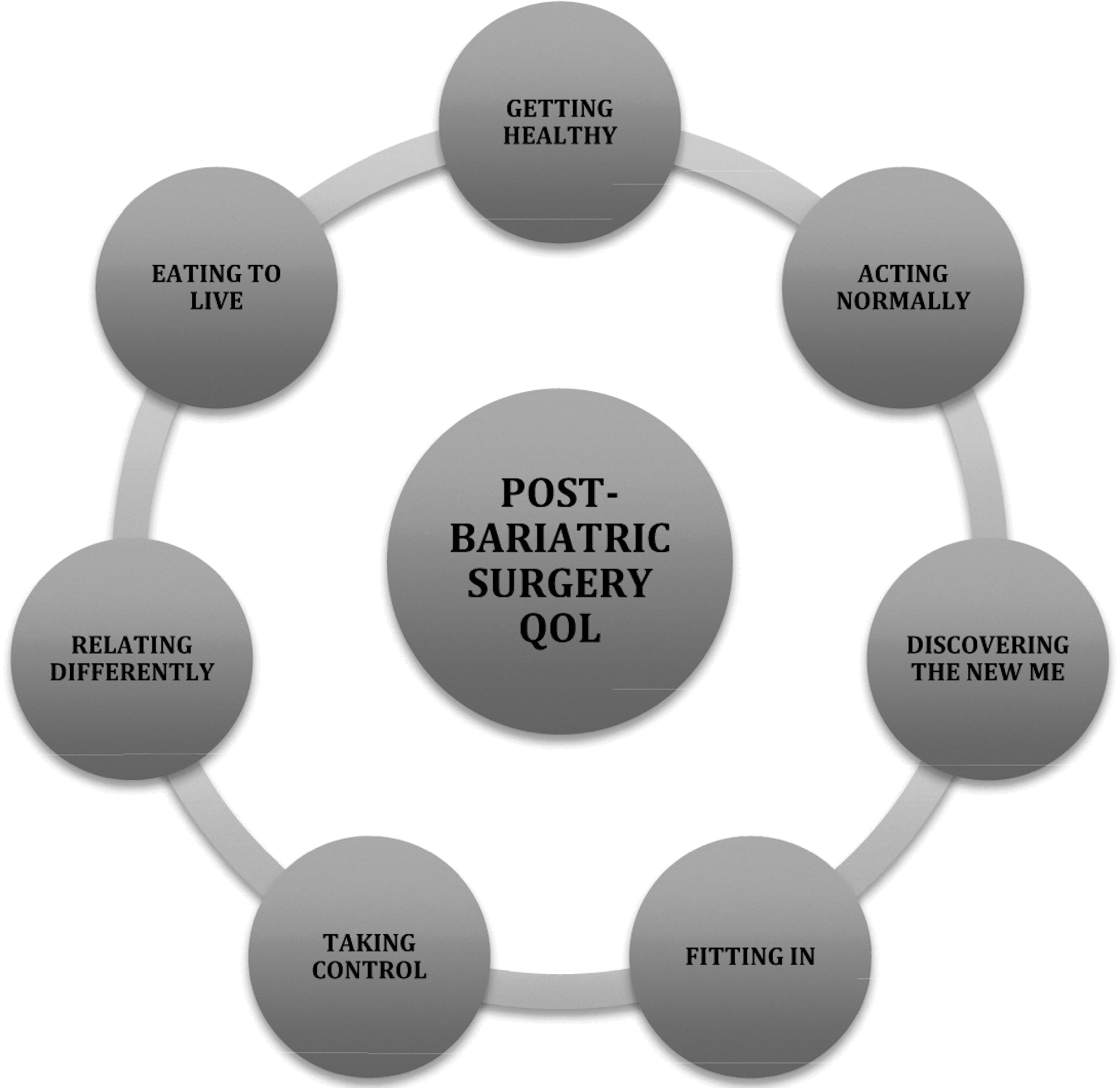
Post bariatric surgery quality of life.
1. Getting healthy
When asked to describe what QOL meant to them, participants in each focus group identified getting healthy as a predominant characteristic. Getting healthy was described in relative terms as compared to pre-weight loss comorbidities and medical dependencies that compromised QOL. Individuals identified the desire to improve health as a strong motivating force for having bariatric surgery. Consistently, descriptions of poor QOL made reference to poor health as a contributing factor. Obesity-related medical conditions such as diabetes, hypertension, sleep apnea, shortness of breath, and pain compromised health and imposed physical restrictions and medication dependencies that interfered with normal life.
Health concerns were cited as major psychological as well as physical stressor. When asked about their QOL before weight loss surgery, respondents shared feelings of frustration, anxiety, and depression related to fears about ill health and its interference with daily life and future well-being. Anxieties about health despair that interfered with QOL were uncovered in the data:
…it [health] was so bad where I couldn't even get myself off the couch. I couldn't bend over and tie my own sneakers and I would sit and cry saying I can't believe I can't do this.
…I said I have to do this. I'm going downhill. I'm falling apart.
Getting healthy emerged as a dynamic and evolving physical situation. For some participants, getting healthy meant that weight loss eliminated all prior comorbidities and that they were no longer dependent on medications. For others, being healthy meant that health had improved and they were taking far less medication. Even those who described new medical problems that arose following weight loss still referred to themselves as healthier since the surgery:
I'm healthier. I think the only down side for me is I have osteoporosis now.
I have like spinal arthritis and I get epidural shots but I have nowhere near the pain that I had even with the shots before and I don't get the shots as often as I did. That to me has been very significant.
I have issues with digestion and electrolyte stuff but I am far healthier than before. I can deal with these problems.
2. Acting normally
Acting normally surfaced as a dominant theme. Participants consistently defined QOL in terms of newfound physical abilities to perform activities of daily life. Being normal is viewed primarily as physical improvements in role functioning:
…they look at me as just a normal person even though I wasn't normal before. As if it never happened.
I remember one time getting under a desk at home to clean and I got trapped under the desk. It's an L shaped and I said to myself, “How I am going to get out?” I had to roll myself out from underneath the desk. Now I can just get underneath this and really clean.
I can bathe my grandbaby in the tub…I can shop and cook. I can stand and iron…go out for lunch.
Acting normally is the capacity to perform the self-care and role-related functions that their nonobese peers do in the course of everyday life.
You had to walk into a restaurant and ask for a chair rather than a booth. My most exciting thing is just sitting in a booth.
I can stand up at the sink and wash dishes for a long time without my shoulder and back hurting.
Regardless of other physical, social, or psychological challenges, those who have experienced long-term weight loss describe their QOL as fundamentally better because they can physically perform like “normal people” in the same roles:
I feel that I can go out and nobody is going to look at me unless I want to be looked at. I can go about my business being a human being and not be a freak.
3. Discovering the new me
This theme refers to individuals' need to integrate a new identity as a non-obese “normal” person. Feelings of confidence, esteem, and self-worth evolve from one's own internal image of self as well as from perceived impressions of others:
I told my friend who is thinking about having the surgery, you're going to develop a whole new identity than what you were.
Feeling like I can be just me. I like confident.
The capacity to reconcile differences in internal and external perceptions and to integrate a new self-identity and body image influences perceptions of the QOL:
A lot of this is in your head and my head was off when I was heavy. I didn't think I was that heavy and now that I'm thinner my head is still off because I think I'm heavy. It's all mental in my head.
I look in the mirror and I still see the old person.
Discovering the “new me” appears to evolve over time. The extent to which individuals are able to successfully integrate a new sense of confidence and self-worth varies as well:
I want to get there. I don't have the confidence to be able to say I can get through this. I'm working very hard to get there.
Part of me fought against losing weight because it was something that set me apart and it was my barrier and it was my isolation from the world. So it was hard to give me a new identity.
But still I look in the mirror and you still see the lumps and the bumps and the fat and I'm never going to be 100lbs. but I'm happy at 200. I have a positive image of myself.
Repeated references to being happy were recorded in group interactions discussing the “new me.” Being happy with better mental health, as well as improved physical well-being, was associated with improved QOL:
Most days I'm happy. I started to accept the fact that this is the size I am.
You just feel better. You're able to think straight…happier now.
4. Fitting in
Descriptions of post weight loss QOL uncover the significance of social acceptance as an essential element. One's sense of being accepted in the social order of things means that life is good again:
I think it's been a good adjustment. I'm much more social now. And I find people coming to me more. My sister and I went on a cruise in May and it was so nice people talking to you. Before, I don't think they would have.
I think you're right. In group settings like that, they would look at you and go to the next couple they wouldn't come over to the heavy people. They wouldn't talk to the heavy people. I have pictures with young couples who are socializing with us. It was nice to socialize with people.
Fitting in is described primarily in terms of what it does not mean:
I use to go to a party and find a chair and that's where I would stay the entire party. Now I go to a party and I go around visit with everybody and have a good old time. I was too embarrassed to even move around because I didn't want anyone to notice me.
Data reflect experiences of bias, ostracism, and criticism that contributed to a poor QOL before weight loss. Fitting in means not standing out. Respondents noted a heightened awareness of how they had been ostracized at work and in social settings as obese persons. In retrospect, they recognized more clearly that others had treated them negatively:
I worked for this company for 40 years and for the bulk of it I was heavy. I got passed over for assignments that I knew I could do. Now I was never the favorite child but now I'm kind of one of the favorite children. It's a different story when you're normal, you know.
Self-imposed isolation and social avoidance behaviors led to a poor QOL before weight loss:
My husband use to get upset with me because I wouldn't want to socialize at all or go to parties or anything like that.
When I was upset with my weight, my significant other would say, “Let's go here…let's go there.” I didn't want to leave the house because I was embarrassed.
Conversely, fitting in posed new challenges as individuals faced social situations that require social skills they had not developed before:
Socially, when I go out with coworkers after work on Thursday or Friday night there are guys that hit on me now that it's so ridiculous too. I never was ever prepared for what came my way…never even had a guy look at you yet alone say hi to you. So now it's kind of like my friends say, “You have five guys looking at you.” And I don't know how to handle it. I never had those alerts up I never knew anything. Now I think so if a guy wants to buy me a drink I'm like “yes!” But then, I can freak about what's next. Socially it's a new experience. It is very scary…I never had any knowledge of that.
Fitting in evolves over time:
Now I'm a little better. I had a set back because I only had lost about 70lbs and put on some weight the past year. So I'm kind of going back to some of those insecurities and self-conscious feelings and I'm trying to work through [them] though it's still better then feeling alone.
5. Taking control
This theme represents an individual's perceived sense of being able to influence or manage one's life, health, and relationships in positive ways that are satisfying and personally fulfilling:
I think happy means for me is to be in control of the things I want to be in control of. To make decisions that I want to make and not be always having to react to other things. For example I can get up and move. I am energized because things I want to do I have energy to do them. When I go into the store people want to help me now. My self-image is so different I project who I really am because I'm in control of my food and my exercise, control of my own schedule. I don't feel like other factors are taking over because I can't do this and I can't do that. And because of my emotional state, my mental state, my physical state I feel so much more empowered. I'm physically, emotionally and mentally in a better place.
Taking control meant finding ways to handle unanticipated outcomes of weight loss that could potentially compromise QOL. These were physical as well as psychological and social consequences that were not expected. They were described as surprising, perplexing, and upsetting. Individuals recounted the need to cope with them, come to terms with them, or learn new ways to deal them:
I lost the weight I expected to but I didn't realize how much it would change my life, like it's changed a lot more than I thought it would…I don't think I realized that it would make me feel as different as it did.
I thought that this would be the cure that I wouldn't get that snacking urge. I thought that would go away and it didn't. That was an eye opener; the surgery is not curing that. I had to learn to deal with things.
…I wasn't prepared for a major life style change [and] neither was my family. Neither was my wife and I think all that preparation leading up to it got me in that frame of mind and I thought I had a good idea what my life style change was going to be before it happened.
Stretched and loose skin folds are more problematic than anticipated:
I would like to see insurance companies pay for skin removal because I was fortunate to have had hernias I was able to have those done and pay a little bit more for the tummy tuck. There is nothing I can do with this.
I would love to have my legs done and in a bathing suit I have a skinny waist and these fat legs.
The point is whether it's on your waist or torso it's invasive to your life style.
Taking control is not an easy process. Uniformly, participants describe their journey toward a better QOL as hard work:
I'm still struggling. Once you make that decision you can't go back. I tore up my insides.
This struggle to manage what is happening in their lives extends to the efforts they have to make to coordinate care decisions among a variety of providers with differing opinions about how to manage health problems.
And it's just you get stuck between your [primary care doctor] PCP and then Dr. X [surgeon] and then if you go somewhere else for something else it's kind of circular even the GYN as far as estrogen you get in a circular thing. And I have to go and have bowel work with the GI Doc and I have had to change there. But they all…they all have different opinions and it is hard to coordinate everything. So I have thoughts about when I'm 70 or 80 what's going to happen because they don't know.
6. Relating differently
This theme captures the changes experienced in family, social, and work relationships after weight loss surgery.
I was involved in numerous support groups and I found it interesting that not in any of the groups that I attended did I hear about any of the psychological issues that we try and deal with or even think about. There are a large percentage of people that have psychological issues, relationship issues and family things that come out of this and I don't think the community is addressing [the relationship] issues we experience.
I had to learn how to deal with people who wanted to know why I took the easy way out.
Changes in family dynamics and in relationships with significant others were perceived as both positive and negative. Support from loved ones factored into descriptions of the quality of their lives at home:
I have been married 40 years and he's been married for 36 years and I'm concerned about my marriage. But I don't know if I have changed that much or if my wife has not come to terms with the new me.
My family constantly watches me. It's very uncomfortable and it's very uncomfortable for me to go to dinner at someone's house because they know it and they watch it. It is just really uncomfortable.
Relating differently encompassed interpersonal changes that occurred in the workplace as well. Individuals reported with a sense of pride that they now dealt differently with work expectations, suggesting that a newfound assertiveness in their response to employers and employee peers:
I used to always say, “Of course I can work Saturday.” Now I'm starting to say, “Are you on crack! I'm not working on Saturday.”
People had expectations of you that you gave them and now when I speak my mind people are a little put off. I always use to roll over.
7. Eating to live
Changes occurred in both eating patterns and individuals' attitudes toward food. Eating was now associated with physical well-being rather than viewed as a psychological need or social event. Eating to live captures how life has changed in relation to eating. This included new intolerances to certain food items as well as new cravings and nutritional challenges. In response to a question about how their QOL had been affected by the surgery, respondents noted:
Eating. I think that's where it can be misleading to some people who think that because I got my surgery, I'm set for life. But you're not set for life; you have to watch everything you eat. I'm a perfect example. I gained 17lbs. this last year.
I think what I wasn't ready for was recovery. One of the hardest things was my relationship with food. I use to tell my husband that food was not my friend. And now a lot of days it is not my friend and I never know how I'm going to feel from one day to another.
Changes in food cravings, eating habits, and preferences were described as unpredictable from one day to another, unexpected, and often unpleasant.
I'm comfortable where I am but one of the things I've learned is I don't eat. I don't have the cravings. I use to eat candy all the time and I don't even want to. I don't have the desire. I don't eat pizza. I don't know physically how that changed but it did. When I take a plate of food I take a small plate and I don't even eat it all. My dog gets the rest. But I'm not doing it in terms of diet. Something physically changed with me.
There's no safe food. There's nothing you can eat all the time and not have an issue with it.
Discussions about QOL generated spontaneous conversation about how life had changed in relation to food. Groups described eating behaviors and attitudes preoperatively that were in sharp contrast to postoperative experiences. Instead of living to eat, the daily focus had shifted dramatically to eating to live in a healthier and happier way.
So yes my quality of life has improved. The stress with the food has changed and it hasn't. I now basically can't overeat. I could but it's going to come right back up. So I don't have to worry about that all the time…the dieting and all that kind of stuff.
It made me a lot more aware of the quality of what I was eating. I think I use to eat just whatever…not anymore.
Now food nourishes my organs, not my heart.
To summarize, data analysis led to the discovery of QOL as a relative and dynamic expression of one's overall sense of well-being. Seven interrelated and inseparable themes emerged to describe its essential structure. Weight loss improves QOL because it means getting healthy, acting normally in one's role, discovering a new sense of identity as a nonobese person, fitting in socially, relating differently at work, at home, and in society, and eating to improve rather than threaten one's health and well-being.
Discussion
While findings from this phenomenological study are not generalizable, several conclusions are drawn that inform understanding of what QOL means to those who have had life-altering weight loss surgery. First, findings affirm that weight loss surgery has a profound effect on QOL that is sustained beyond the first postoperative year, as cited in an expansive base of scientific literature. Significant weight loss was the catalyst for physical, psychological, and social changes that individuals perceived as a new sense of normalcy that improved the quality of their lives. Gender, age, surgical type, postoperative status, and the occurrence of complications varied across groups. Yet, regardless of these variations, there was unanimous agreement among participants that QOL was demonstrably better because of their weight loss surgery. More recent long-term studies report similar conclusions. Individuals enjoy sustained improvements in QOL following successful weight loss surgery regardless of procedure type, comorbid conditions, or complications that occurred following surgery.10,12,14
Second, QOL emerged as a dynamic, complex, and highly subjective experience. Participants described what QOL meant to them as an evolving process rather than a constant state or static condition. Improvements in self-esteem, confidence, and social life, as well as improvements in physical health, occurred at varying rates over time. Expressions of improved psychological and social well-being were inextricably tied to improvements in physical health and functioning. Progress in “discovering the new me,” “fitting in,” taking control,” and “relating differently” occurred at different rates among participants and was reported along a continuum of positive to negative experiences. Yet, overall QOL was perceived as improved even when individuals reported negative perceptions of how they were doing in relation to these psychosocial domains. These findings advocate for a holistic definition of QOL as proposed by the World Health Organization 34 and King and Hinds 35 whose work studying QOL among oncology patients advances understanding of this phenomenon from the patient's unique perspective.
Third, physical improvements in one's clinical condition, mobility, and role functioning appear to have the strongest influence on what QOL means to this population. Findings support the work of Burton et al. 14 who found that QOL scores among those who were 3 years post laparoscopic adjustable gastric banding were improved, but were less than community standards, except in physical functioning. Similarly, a prospective study by Schouten et al. 12 found that postoperative QOL is mainly dependent on weight loss and decreased comorbidities. QOL parameters including physical ability, mobility control, mobility range, and energy level were significantly improved 7 years after bariatric surgery.
Fourth, psychological adjustments surface as the most challenging, even years after having bariatric surgery. These challenges were reported as surprising and unexpected despite extensive preoperative preparation for the life-altering nature of bariatric surgery. Descriptions of surgery as “not a cure all” and their discovery that success requires taking control in all areas of life reveal what having life-altering surgery really means. Building a new identity and a positive self-image as a nonobese person is described as a slower, more difficult process than adjusting to external changes in appearance. For many, internalizing a new sense of self was more of a struggle than dealing with the consequences of nutritional deficits, diet modifications, and body changes. Predictive studies to identify the demographic, psychological, and social variables affecting emotional adjustment in this population are underreported in the literature. However, studies have found that emotional well-being does vary among post bariatric surgery patients and is affected by such preoperative factors such as depression and the presence of psychiatric comorbidities.4,37
Fifth, individuals who experienced bias and discrimination preoperatively as obese people continue to experience it after weight loss surgery. As if experiencing the world differently, individuals communicated a heighten awareness of how they were ostracized and isolated by others because of their obesity before surgery. Positive feelings of social acceptance and self-worth following weight loss were offset by a new awareness and insight about how the obese are mistreated and ostracized in society. Worth noting, individuals reported that others, including nurses and physicians, judged them negatively because they had decided to have weight loss surgery, implying that they were “taking the easy way out.” For some, this contributed to a newfound assertiveness and self-righteousness that impacted both personal and work relationships. This finding extends the conclusions of others who have examined the extent and impact of discrimination against obese individuals. 37
Finally, eating continues to dominate as an activity of daily living in terms of time and attention. However, the reason for this shifts dramatically after surgery. Now, interest in eating focuses on nutrition and avoidance of new food intolerances rather than on satisfying some unconscious emotional need. How one feels after eating is no longer predictable. Changes in food tolerance can cause distressing and sometimes sudden physical symptoms that are particularly embarrassing in social situations. Just as when they were obese, individuals report similar concerns about what and where to eat long after surgery but for far different reasons. Others report similar findings that eating still poses one of the biggest challenges faced by postoperative bariatric patients and that this is intensified for those with eating disorders such as binge eating that existed before they had surgery.14,38
Study limitation
There are several limitations to this study. First, it was designed as a single site, single surgeon study which limits transferability of findings. Next, the design may have led to sampling bias. While inclusion criteria did not exclude those who had postoperative complications, it is possible that only individuals who had a positive surgical experience and postoperative course may have agreed to participate in the study. Also, men may have been underrepresented, and it is not known if sociocultural differences influenced participants' perceptions. Third, while research team members were trained and used the same interview script, variations in facilitators' questioning style may have influenced findings. Fourth, one taped interview was partially inaudible, which made it hard to authenticate transcribed data. Finally, study findings were shared with members of bariatric support groups rather than with those who had actually participated in the focus groups. This was done as an alternative way to conduct an audit check to establish the confirmability of findings because the contact information of focus group participants had been blinded and then destroyed before an audit check was performed.
Conclusions
Findings from this study have implications for nurse researchers, educators, administrators, and practitioners. Findings should inform subsequent research aimed at identifying patient variables and relationships among them that correlate with improvements in QOL. There is more to learn through research that focuses on demographic characteristics among bariatric surgery patients and how these might influence QOL outcomes. More research is needed to test new models for delivering care beyond the inpatient setting and to improve coordination of care across the continuum. Further, correlation studies are needed to examine the extent to which each of the seven themes influences QOL and relationships that may be present among them to explain the phenomenon more fully. On another level, more work must be done to develop valid measures of a bariatric-specific QOL assessment tool that integrates the seven themes found in this study. Existing instruments lack conceptual clarity and content consistency and fail to capture fully the evolutionary and humanistic meaning of QOL as discovered in this study.
Conclusions drawn from this study raise understanding of the challenges and struggles that individuals confront after life-altering weight loss surgery. There is an apparent need for longer-term social and emotional support, as well as help with dietary modifications. Psychological adjustments appear to be more demanding and stressful and may have a more profound effect on overall health and QOL than is currently recognized. Practitioners across disciplines can be stronger advocates for support groups that extend for longer periods of time and incorporate more intense psychological support.
Perceptions of continued discrimination and bias that persist postoperatively among these patients should not be ignored. Both nurse educators and direct care practitioners must investigate the attitudes and behaviors of nurses and other health team members that can have a distressing impact on people who are striving to internalize a new identity and build their self-esteem as nonobese persons.
As a caring practice, nursing is uniquely poised to take the lead in advancing studies and improving practice regarding health-related QOL. Nursing's legacy is rooted in a tradition of concern about the quality of patients' lives and in providing skillful and respectful care that heals the whole person. For individuals who have had weight loss surgery, healing means more than overcoming physical problems and dealing with nutritional issues. It means being productive, feeling valued, and enjoying everyday life again as well. From this perspective, nurses have much to offer in helping them along their journey toward a better QOL as advocates for compassionate, holistic care that extends well beyond the hospital experience.
Footnotes
Disclosure Statement
No competing financial interests exist.