
Abstract
Background:
This prospective study examined physical and mental quality of life up to 6 years after laparoscopic adjustable gastric banding (LAGB) and the predictive role of quality of life for weight outcome.
Method:
Forty-five LAGB patients (38 female, 7 male) filled out the short form-36 (SF-36) health survey 6 months before and 1 and 6 years after LAGB. Body mass index (BMI) was assessed. Repeated measures analyses of variance and multiple regression analyses were used.
Results:
Physical functioning but not mental well-being improved significantly between baseline and 1 year after LAGB, whereas a nonsignificant deterioration occurred for both quality of life dimensions between 1 year and 6 years follow-up. A lower mental well-being before surgery and at 1 year after surgery predicted a larger reduction of BMI at 6 years.
Conclusion:
After LAGB, physical functioning improves more clearly than mental well-being, but this improvement is not fully sustained during the 5 years that follow. Clinicians should be aware that a better mental well-being might forecast a poorer weight outcome in the long term.
Introduction
Although QOL is often assessed as a secondary outcome measure after bariatric surgery, it could also be considered a predictor of health behavior. It is possible that a low QOL obstructs health behavior because of a lack of willpower 16 or self-efficacy, the judgment of one's capability to accomplish a desired effect such as to regulate one's eating behavior. 17 In contrast, according to the Health Belief Model, 18 the perceived burden of a disease and the perceived benefits versus barriers to behavioral change determine the likelihood of behavioral change. We propose that a low QOL may be a signal that a change of health status is needed, while a good QOL may be a signal that no further action is needed. In line with this notion, lower levels of QOL have been associated with treatment-seeking behavior in obesity. 19 Severely obese persons seeking surgical obesity treatment had a lower QOL compared to other overweight and obese populations, even after adjustment for weight, 1 and in patients with unsuccessful weight loss after gastric banding, a lower mental QOL appeared a signal for conversion to gastric bypass. 20
Just after surgery, most patients are in a “honeymoon phase” in which they lose a significant amount of weight and experience an increase in function and well-being, which may explain the lack of predictive findings at short-term follow-up. After 2 years, some patients regain weight. As a consequence, the association of presurgical variables with long-term weight outcome may be higher than the association with short-term weight outcome. The aim of our prospective study was to examine the QOL outcome after bariatric surgery, as well as the predictive role of QOL for weight outcome. We expected that a lower QOL would be associated with a lower BMI at long-term follow-up.
Materials and Methods
Participants and procedure
Between November 2000 and November 2004, 156 patients underwent a laparoscopic adjustable gastric banding (LAGB) procedure at the St. Antonius Hospital Nieuwegein, the Netherlands, using the Lap-Band® system (INAMED Health, Santa Barbara, CA), following screening by a bariatric surgeon, an endocrinologist, a psychologist, and a dietitian. Surgical indications were a BMI ≥40 or a BMI ≥35 in the presence of significant comorbidity. The operation was performed according to the techniques described by Belachew et al. 21 The study protocol was approved by the Research and Ethics Committee of the hospital.
Of the 156 patients, 91 participated in a large-scale survey study, including QOL measures, 6 months before and 1 year after LAGB. Information about the dropouts has been described in our former study. 22 For the current study, we asked the 91 participating patients from this former study to fill out questionnaires again evaluating QOL. This was on average 5.9 (SD=1.0, range 4–8) years postoperatively. The 15 patients who underwent a gastric bypass between 4 and 8 years after LAGB were excluded. Of the remaining 76 patients, 2 patients had died, and 29 patients had incomplete weight records or did not return the questionnaire. The 45 participating patients consisted of 38 women and 7 men with a mean age of 48 (SD=9, range 31–64) years. Of these, 42 patients (94%) had completed vocational education or high school (one patient had completed primary education and two patients had completed college or undergraduate school).
Attrition analyses using independent t-tests revealed no differences between the 45 participating patients and the 29 patients with incomplete records with respect to age, gender, BMI (before, 1 year after, and 6 years after surgery), and physical functioning and mental well-being (before and 1 year after LAGB; all p values>0.05).
Assessments
Weight and height were measured at the St. Antonius Hospital. Preoperative and postoperative weights were determined during routine checkups in the hospital. BMI was calculated as weight in kilograms divided by the square of the height in meters (kg/m2).
For QOL assessment, the RAND short form-36 (SF-36) health survey 23 was used. Physical component summary and mental component summary scores were measured as a reflection of physical functioning and mental well-being. 24 The SF-36 questionnaire has adequate psychometric characteristics, including good construct validity, high consistency, and high test–retest stability. 25 Moreover, in patients with morbid obesity, the two summary scales of the SF-36 have proven satisfactory validity. 26
Statistical analyses
The score distributions of the QOL dimensions were sufficiently normal to allow parametric statistics. 27 Plots of regression analyses showed that the assumptions of linearity (residuals vs. predicted values) and normality (normal probability plot of the residuals) were met to apply multiple regression analyses.
Weight loss 1 year after and 6 years after LAGB was defined as the percentage of excess body mass index lost (%EBL) according to standard procedures. 28
Repeated measures analyses of variance were used to examine postoperative changes in BMI, physical functioning, and mental well-being scores. To examine the magnitude of changes in physical functioning and mental well-being, effect sizes were computed as the difference between the means divided by the pooled standard deviation (Cohen's d). Effect sizes of 0.2, 0.5, and 0.8 are considered to reflect differences of small, medium, and large magnitude respectively. 29
Because age was significantly correlated with our main variables, partial concurrent correlation coefficients—adjusting for age–were calculated between all our main variables at the different time points.
Linear regression analyses were performed to examine whether QOL before surgery and at 1 year after surgery predicted BMI outcome at 6 years. We performed two separate regressions for mental well-being and physical functioning. Baseline BMI and age were controlled for in the first step. A sample size of 45 gives the opportunity to examine the dependent variable as a function of three predictors (baseline BMI, age, and QOL) as calculated with G*Power 3: two-sided α-level of 0.05, power (1−β) of at least 0.80. 30
To adjust for gender differences in the BMI outcome at 6 years, we repeated the regression analyses for women only, but no differences were found. This method was chosen because only seven men participated. Statistical significance was set at p<0.05. Data were analyzed using SPSS for Windows (v16; SPSS Inc., Chicago, IL).
Results
Table 1 summarizes the means and standard deviations of BMI, %EBL, physical functioning, and mental well-being at the different time points. Repeated measures analyses of variance showed significant changes in physical functioning (F(2, 44)=35.09, p<0.001). Post hoc tests, with Bonferroni correction for multiple comparisons, revealed that physical functioning scores improved significantly between baseline and 1 year after LAGB (p<0.001, the effect size was large: d=1.17), whereas a nonsignificant deterioration occurred between 1 year and 6 years follow-up (p=0.055, the effect size was small: d=−.35). We did not find significant changes in mental well-being scores over time (F(2, 44)=2.45, p=0.09). The changes of mental well-being between baseline and 1 year after LAGB (d=0.32) and between 1 year and 6 years after LAGB (d=−0.21) were both small.
Higher scores indicate a better physical functioning and mental well-being.
Partial concurrent correlations (adjusting for age) of BMI with mental well-being and physical functioning were neither significantly correlated before surgery (r=0.11, p=0.48 for mental well-being, and r=−0.04, p=0.81 for physical functioning) nor 1 year after surgery (r=−0.14, p=0.38 for mental well-being, r=−0.09, p=0.56 for physical functioning). However, at 6 years after surgery, a better mental well-being (r=0.38, p=0.01) and a worse physical functioning (r=−0.39, p=0.01) were correlated with a higher BMI.
Table 2 shows the results of the regression analyses. Having entered BMI before surgery (or at 1 year after surgery) in the first step of regression analysis, in the subsequent steps, the baseline-adjusted change of BMI is predicted. All predictions were also adjusted for age. A lower mental well-being before surgery (Fchange(1, 41)=5.31, p=0.03) and at 1 year after surgery (Fchange(1, 40)=16.33, p<0.001) was associated with a decrease of BMI at 6 years postoperatively after controlling for baseline BMI (before surgery or at 1 year after surgery) and age. We did not find any prospective associations for physical functioning or for any of the predictors—mental well-being or physical functioning—when using BMI at 1 year as an outcome variable.
B=regression coefficient; SE B=standard error of B; β=standardized regression coefficient.
p<0.05; **p<0.001.
Predictors before surgery:
For mental well-being: ΔR2=0.08, p=0.03; for physical functioning: ΔR2=0.001, p=0.79.
Predictors 1 year after surgery:
For mental well-being: ΔR2=0.13, p<0.001; for physical functioning: ΔR2=0.004, p=0.54.
To examine the robustness of the findings, we computed age-adjusted correlations between the absolute level of BMI after 6 years and QOL (mental well-being and physical functioning) during the previous two assessments. A better mental well-being before surgery was significantly correlated with a higher absolute BMI at the long-term follow-up (r=0.35, p=0.02); the correlation between mental well-being 1 year after surgery and long-term BMI was r=0.29 (p=0.06). Physical functioning scores at baseline (r=−0.05, p=0.73) and 1 year after surgery (r=−0.15, p=0.35) were not significantly correlated with BMI 6 years after surgery.
To examine the clinical relevance of the findings, we compared BMI and the percentage of excess BMI loss between patients below and above the median on mental well-being at baseline. In the general population, the mean of this mental well-being score is 50 and the standard deviation is 10. For the group low on mental well-being before the operation (M=36.3, SD=7.4), the BMI 6 years later was 34.5 (SD=5.6) and the percentage of excess weight loss was 55% (SD=25). For the group high on mental well-being before the operation (M=56.1, SD=5.3), the BMI 6 years later was 39.0 (SD=6.0) and the percentage of excess BMI loss was 37% (SD=22). The group with a low mental QOL at baseline had significantly more excess BMI loss (t=2.5, p=0.02) to a lower BMI level (t=− 2.6, p=0.01) than the group with a high mental QOL at baseline. The effect sizes of the difference in absolute BMI (d=0.78) 6 years later between the groups low and high on mental QOL and of the percentage excess BMI loss (d=0.77) were both moderate. Figure 1 shows the percentage excess BMI loss at the long-term for patients low and high on mental-well-being before the operation.
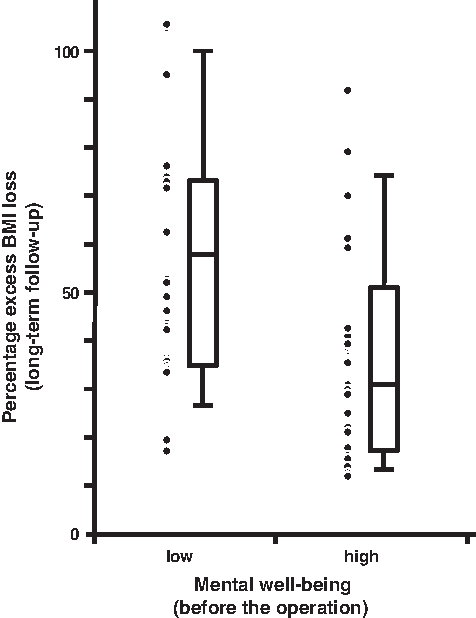
Percentage of excess body mass index loss (%EBL) at the long-term follow-up for patients with a low (left) and high (right) mental well-being before the operation. Data are shown as dots for every research participant and as boxplots. Each box represents the 25th to 75th percentile with the median in the middle. Bars outside the boxes represent the 10th to 90th percentile.
Discussion
The aim of our study was to examine QOL as an outcome after bariatric surgery, as well as a predictor of long-term (6 years) weight outcome after LAGB. Our findings showed a significant increase of QOL in the first year after LAGB for physical—but not for mental—QOL. A lower mental well-being—but not a poorer physical functioning—preceded a better weight outcome in the long-term.
Our study suggests that patients on average profit more in terms of physical functioning than in terms of mental well-being when undergoing bariatric surgery. Compared to some earlier studies on the postoperative course of QOL, our study demonstrates that QOL does not further improve with increasing postoperative time. This may reflect that patients are in a kind of “honeymoon” phase 1 year after surgery, while they are more realistic at 6 years follow-up.
We expected that the burden of a low level of physical functioning and mental well-being could be a cue to reduce weight loss further. This expectation was not confirmed for physical functioning, but we found a significant prospective association for low mental well-being with more weight loss at 6 years. There are several possible explanations for the finding that a lower mental well-being may play a role in the maintenance of the amount of weight lost at 6 years follow-up. Distressed people may seek additional resources aimed at helping them to achieve a lower body weight (e.g., a dietitian, bariatric nurse, or psychologist) or they may induce more helping behavior from bariatric professionals (e.g., nurses), who, for example, may make more appointments with these patients or tighten the gastric band more often. In a previous study, 20 we found that patients with unsuccessful weight outcome after LAGB who underwent a conversion to a gastric bypass were the ones with the lowest mental well-being. This supports the idea that patients may seek or are offered additional professional help from the bariatric team. However, our current results may also reflect that the patients who lost somewhat more weight at 6 years postoperatively were the ones who were less satisfied with the operation outcome 1 year after surgery as reflected in a lower mental well-being. Future studies should examine why patients with a lower mental well-being have a better long-term weight outcome, as this may help in the guidance of patients after bariatric surgery.
The prospective design, a long-term follow-up of 6 years, and the use of reliable and validated questionnaires are strengths of this study, but weaker points should also be indicated. One weakness is that the sample size was small because not all patients of our preoperative sample complied with our request to fill out and return the questionnaire voluntarily at 6 years follow-up. Our decision to perform an additional follow-up 5 years after intervention may also have influenced the low long-term follow-up rates. However, attrition analyses showed no differences between 29 dropouts and 45 completers with respect to age, gender, BMI, and physical functioning and mental well-being. This problem of dropouts in long-term follow-up studies is also described in other studies.32,33 Further, the data from routine checkups in the hospital suggested that there is no long-term weight loss difference between participating patients and the “real” dropouts (i.e., nonresponders). Another feature of the study is that the sample consisted of more women than men, but the higher percentage of women than men is in agreement with a previous observation that 83% of the surgical treatment population is female. 1 Finally, the results do not generalize beyond patients who did not have a gastric bypass operation afterwards.
Conclusion
Our findings demonstrate that after surgery for morbid obesity, physical functioning improves more than mental well-being and that the improvement of QOL is not fully sustained during the 5 years to follow. A lower mental well-being preoperatively and 1 year postoperatively was associated with a better weight outcome at 6 years follow-up. The bariatric team should be aware that a higher QOL is not a guarantee for a good weight outcome. Instead, weight loss maintenance may even be difficult in patients with a high QOL.
Footnotes
Disclosure Statement
No competing financial interests exist.