
Abstract
Vertical banded gastroplasty (VBG) was once a common operation for surgical weight loss. Though the operation has lost favor, there are patients that are having complications and symptoms related to the surgery. A case involving a patient with severe regurgitation, vomiting, and poor oral intake is presented. The surgical technique for reversing the VBG is detailed, including technical points of interest.
Introduction
I
Despite these advantages, long-term complications can arise. The percentage of patients with food intolerance, vomiting, regurgitation, and gastroesophageal reflux disease (GERD) is higher than with other bariatric procedures. Significant vomiting (more than once a week) can be seen in 21–48% of patients, and GERD was found in 38% at 3 years postoperatively. 4 The 5 year reoperation rate for VBG has also been reported at 25%, mostly due to patients' inability to tolerate regular foods or severe vomiting. 5 It is on this group of patients that the technique described below focuses.
Though some articles suggest that conversion to a gastric bypass may be the best option for revision of a VBG, 6 many patients that require reoperation desire the ability to sustain their own nutrition without the need for alternative supplements. Other patients have severe symptoms of regurgitation and reflux and want help controlling those symptoms. It is in this population of patients where reversal of the VBG has the most utility. It has been shown that after reversal of the VBG, patients have improved Visick scores for symptomatic reflux and no reflux symptoms in 93% of patients. 7 Therefore, reversal of a VBG should be an option for patients who have a poor quality of life due to symptoms caused by complications of a prior VBG.
Case Report
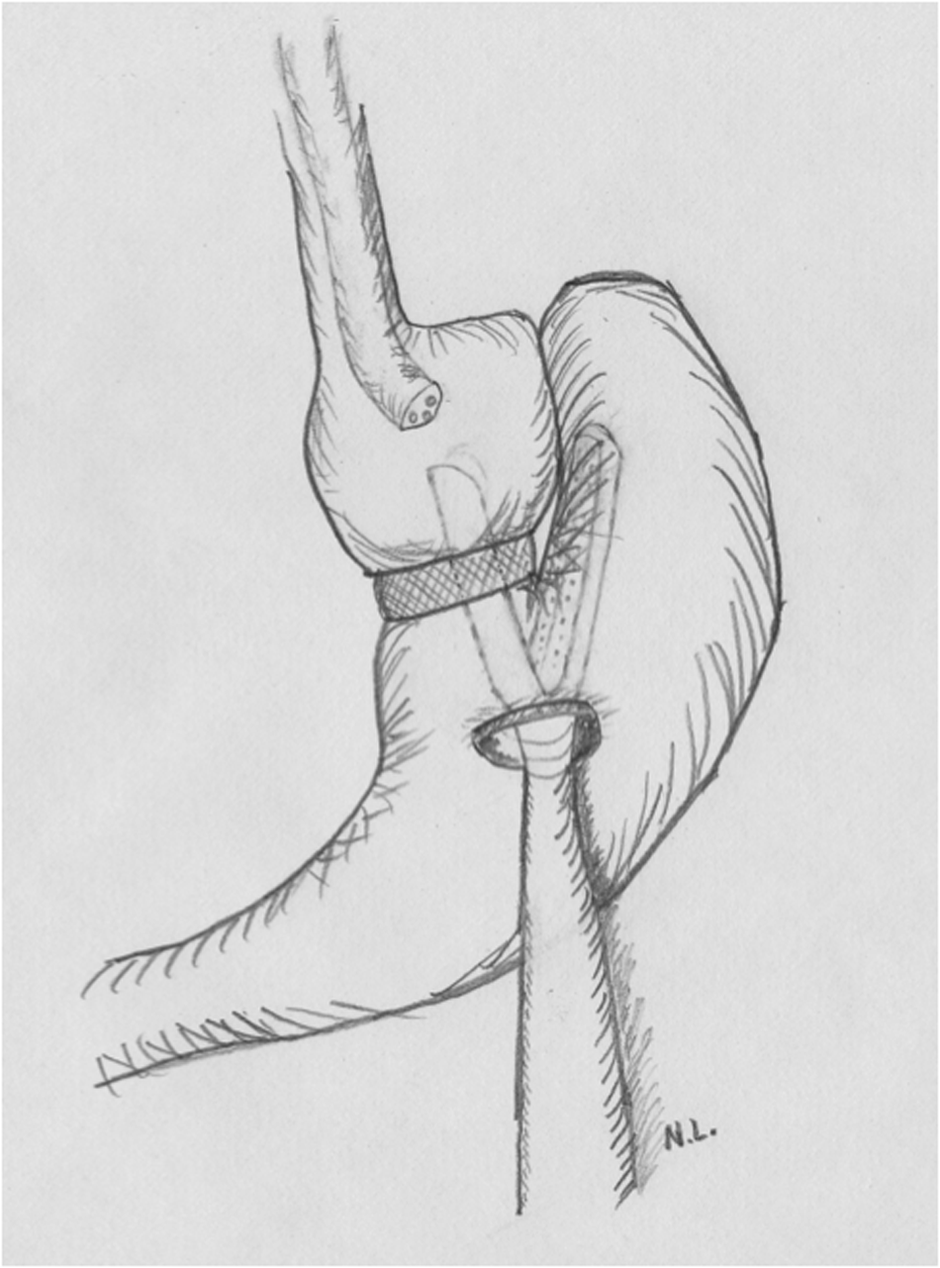
The patient is a 51-year-old woman, who had a VBG performed with the open technique 23 years prior and had a reported body mass index (BMI) of 36. She began having severe dysphagia, vomiting, and regurgitation requiring multiple endoscopies for food disimpaction. Balloon dilation was also performed at the time of disimpaction but did not improve her symptoms. Due to her poor oral intake, her nutrition was maintained with home total parental nutrition (TPN). Her BMI had decreased to 24. She was evaluated in clinic, at which time her preoperative workup was started. She underwent endoscopy and upper gastrointestinal (GI) series to evaluate her prior VBG. A representative image from the upper GI series is shown (Fig. 1). The diagram (Fig. 2) helps to illustrate the anatomy, staple line, and mesh band seen in the radiograph. The staple line is intact, and there is stenosis of the gastric pouch outlet. Preoperative esophagogastroduodenoscopy (EGD) also confirmed stenosis, in which the outlet was estimated to be 9 mm in diameter.

Preoperative upper gastrointestinal (GI) series with the band (B) and staple line (S) labeled.
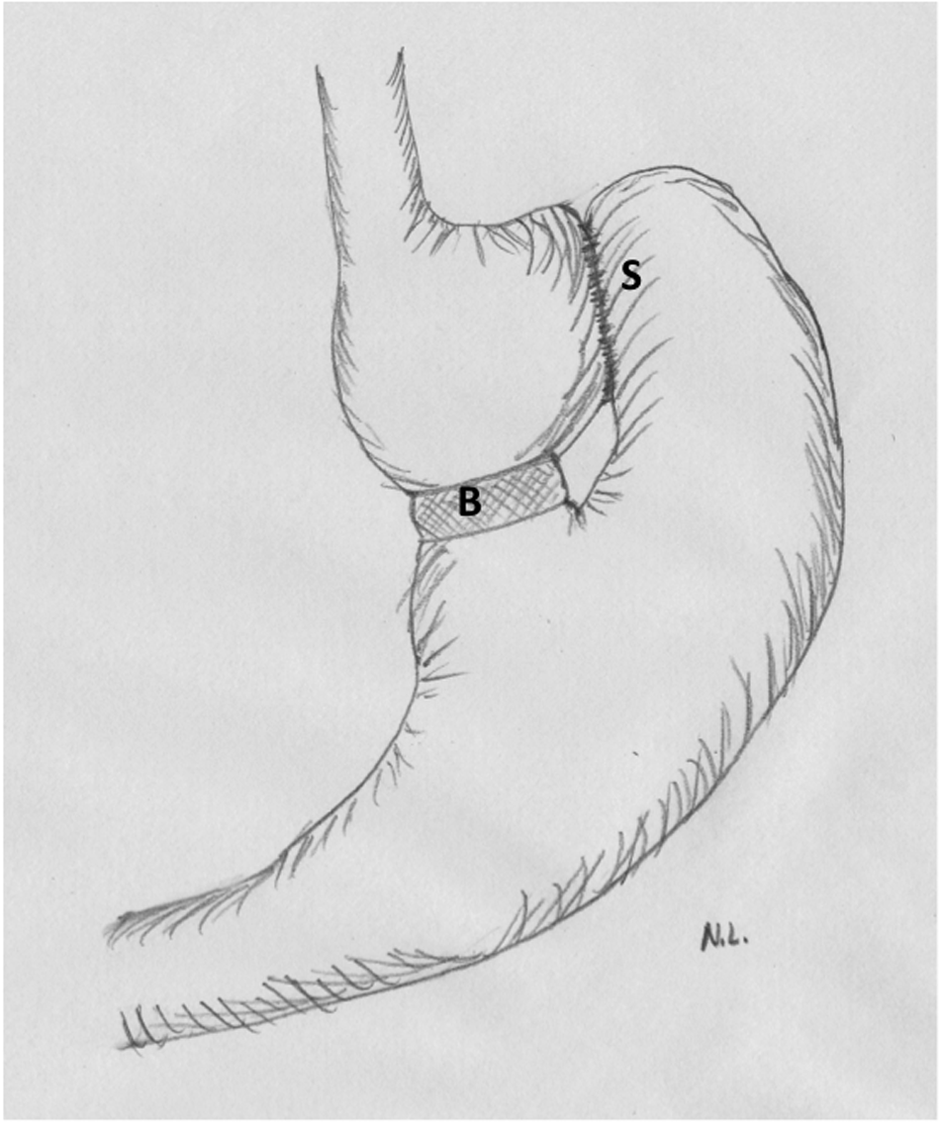
Illustration of the vertical banded gastroplasty (VBG) with the band (B) and staple line (S) labeled.
After the workup was completed, the findings were presented to the patient, and options of a revision to the gastric bypass versus a reversal of the VBG were discussed. Because of the patient's poor quality of life, inability to sustain herself with oral nutrition, no comorbidities, and significant weight loss, a reversal of the VBG was decided upon.
The patient underwent her procedure, as detailed below, with no complications. A postoperative upper GI series was performed showing resolution of the stenosis and improved passage of contrast into the distal stomach (Fig. 3). She was discharged home on postoperative day 1, tolerating a liquid diet. On short-term follow-up, the patient was off home TPN, tolerating a regular diet, and maintaining her weight. Her quality of life was much improved. She had no complaints of dysphagia, regurgitation, or reflux.

Postoperative upper GI series showing improved passage of contrast and no leak.
Technique
The patient is positioned supine on the operating table with arms out and secured using a footboard and two leg straps. The operating surgeon stands to the patient's right, the assistant to the patient's left, and the endoscopist at the head of the table. Instruments include: two 12 mm trocars, one 5 mm trocar, a 5 mm bipolar device, atraumatic graspers, a hook cautery, a laparoscopic needle driver, three 2-0 silk sutures cut 6 inches long, a 60 mm linear stapler with three reloads, and a gastroscope.
Safe entry is performed, pneumoperitoneum is achieved, and the abdominal cavity is inspected laparoscopically. The endoscope is then passed into the gastric pouch and through the stenosis, if able, to perform a careful intraluminal evaluation. The stenosis was clearly identified in our case study (Fig. 4). Once the endoscope is passed through the band, retroflexion of the scope is performed to inspect fully the upper portions of the fundus, band, and staple line.
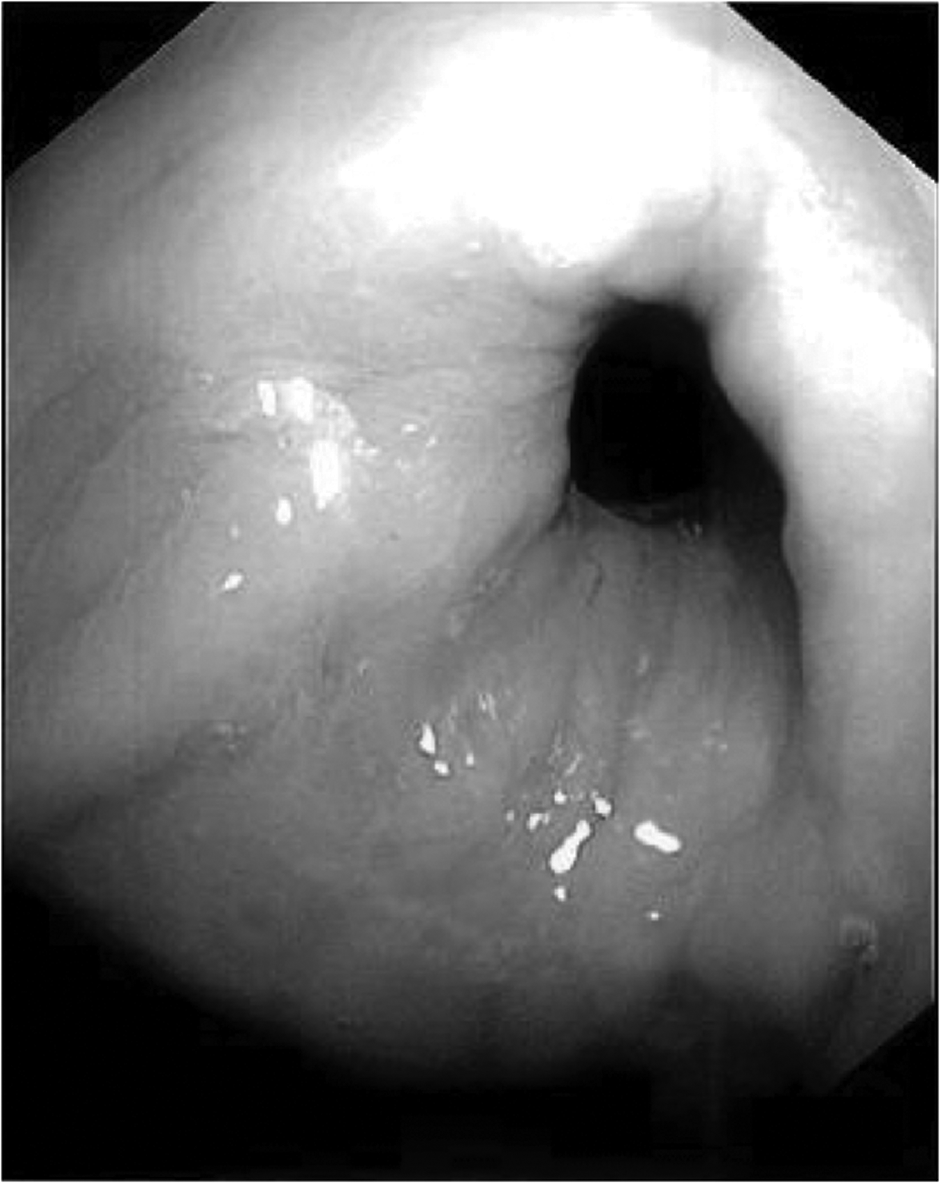
Endoscopic view of the stenosis created by the band.
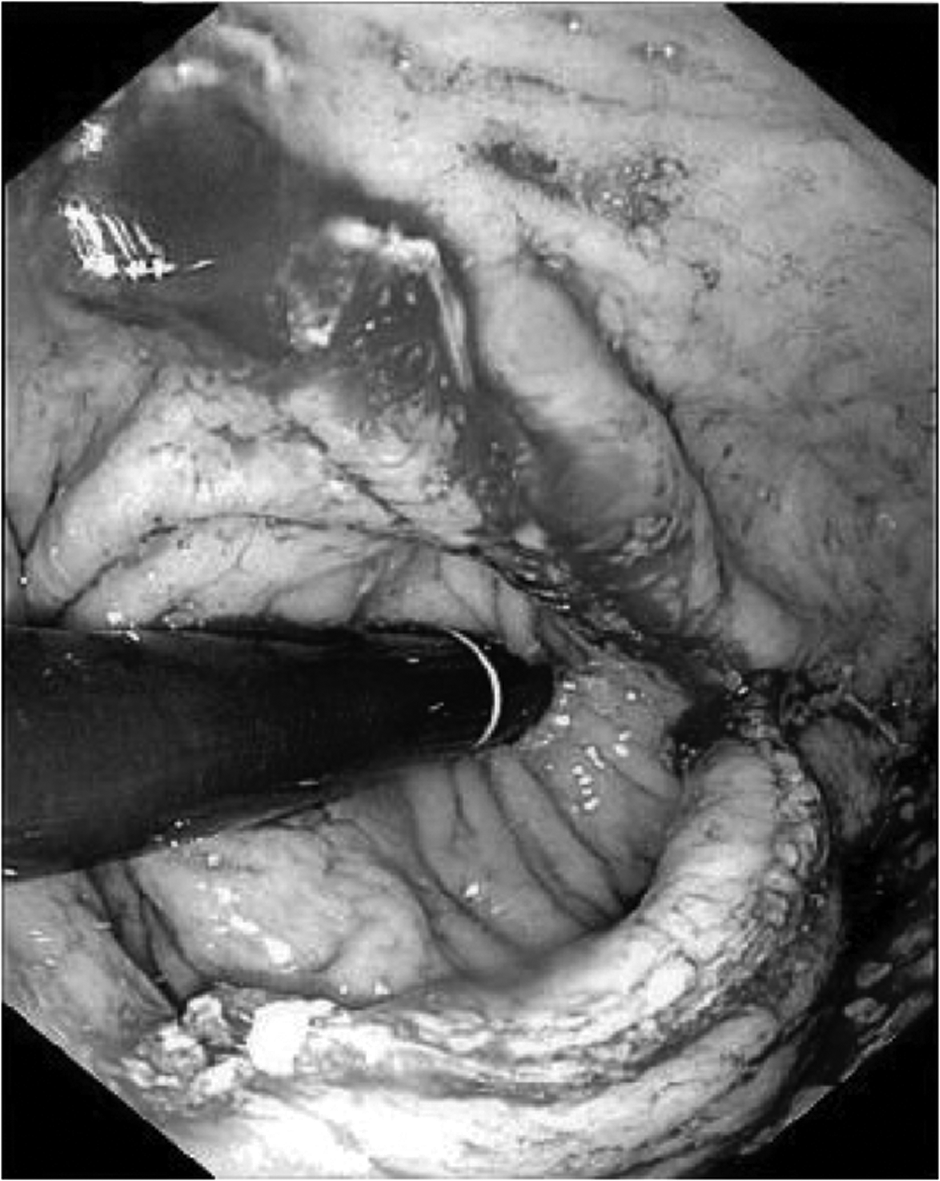
Once the endoscopic evaluation is complete, the anterior surface of the stomach is examined laparoscopically. The adhesions overlying the band are now taken down using the bipolar cautery device. This will allow full inspection of the band in relation to the gastric wall, as well as the anterior surface of the stomach (Fig. 5).
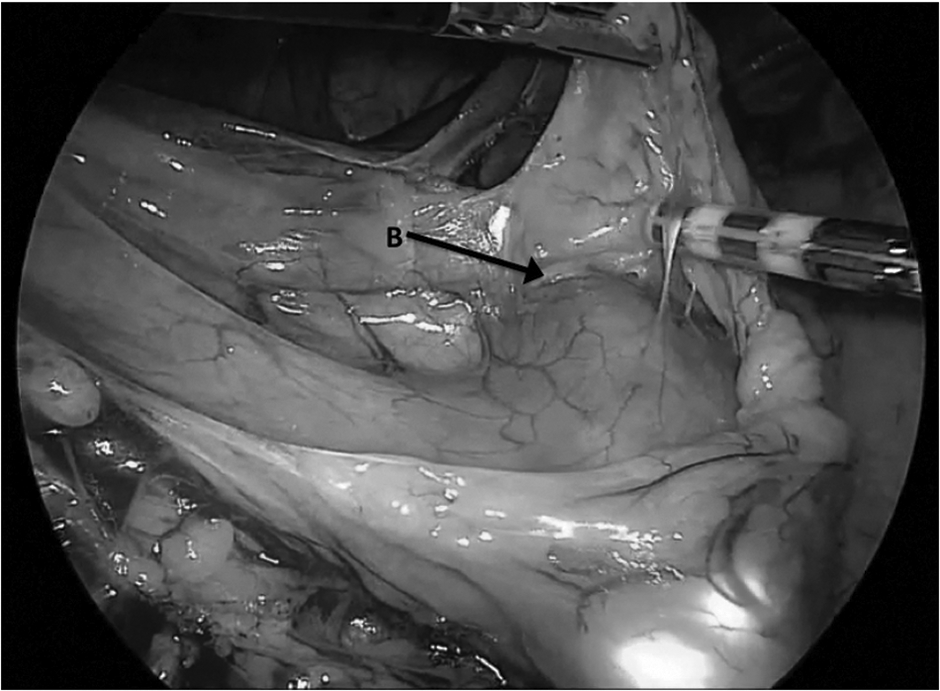
Lysis of adhesions on the anterior surface of the stomach. The endoscope is seen passing through the band (B).
With the guidance of the endoscope, an anterior gastrostomy is then created. This gastrostomy is placed on the body of the stomach along the greater curve, but anterior enough that it can be closed without significant effort (Fig. 6). If the gastrostomy is placed too distally, this may create a difficult angle for the proper positioning of the stapler intraluminally, as well as cause narrowing of the gastric outlet once the gastrostomy is closed. The stomach lumen is entered using a mixture of monopolar and bipolar energy. The gastrostomy is enlarged to allow seamless passage of the gastroscope and linear staplers as needed.
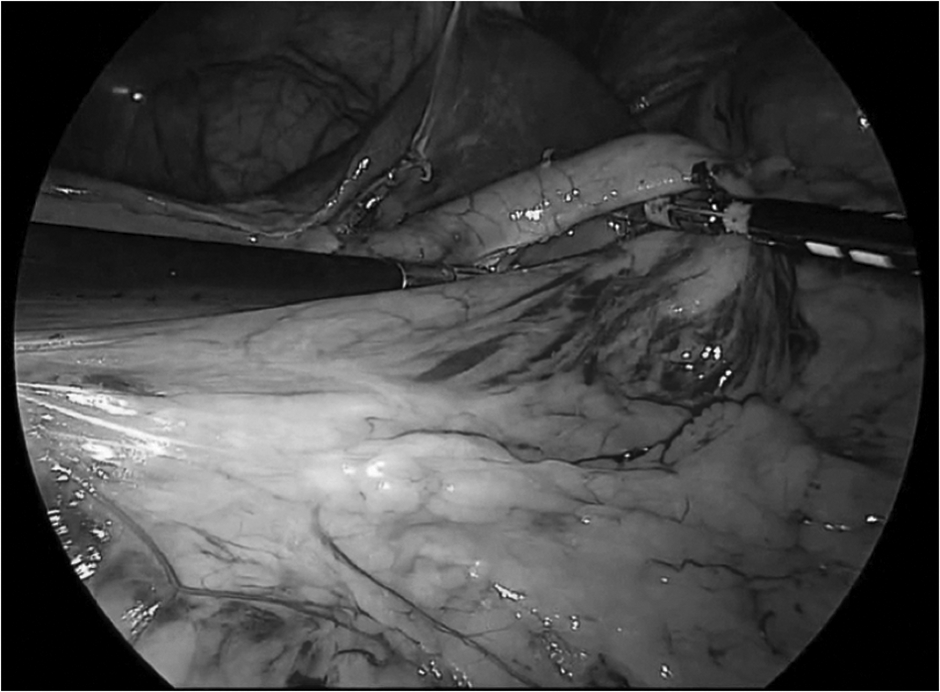
Creation of anterior gastrostomy along greater curve of the stomach.
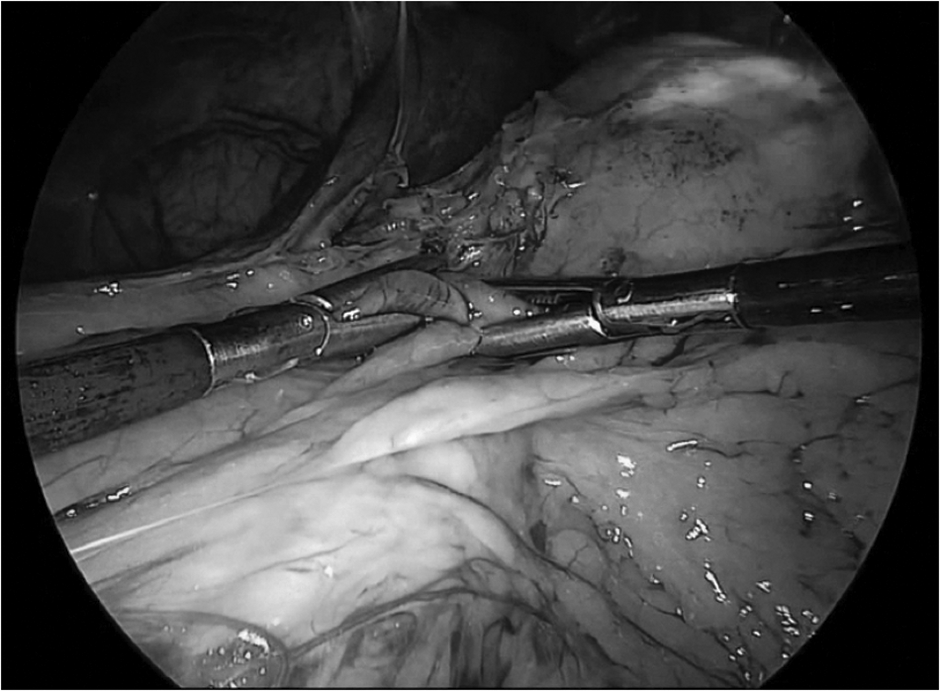
After the gastrostomy is adequately enlarged, the gastroscope is passed down the gastric lumen into the abdominal cavity so that it can be visualized laparoscopically. The linear stapling device is then introduced into the operative field through the left upper quadrant 12 mm trocar. With the guidance of the endoscope, the stapler is then passed through the gastrostomy into the gastric lumen. The stapler is guided into the proximal stomach by holding the tip of the gastroscope with the jaws of the stapler (Fig. 7). The gastroscope is retracted through the stenosis allowing accurate and proper positioning of the stapler. The blade of the stapler is then passed through the stenosis with endoscopic visualization (Fig. 8). Figure 9 illustrates the correct positioning of the stapler straddling the band. The stapler is then fired, dividing the band, and withdrawn through the gastrostomy.
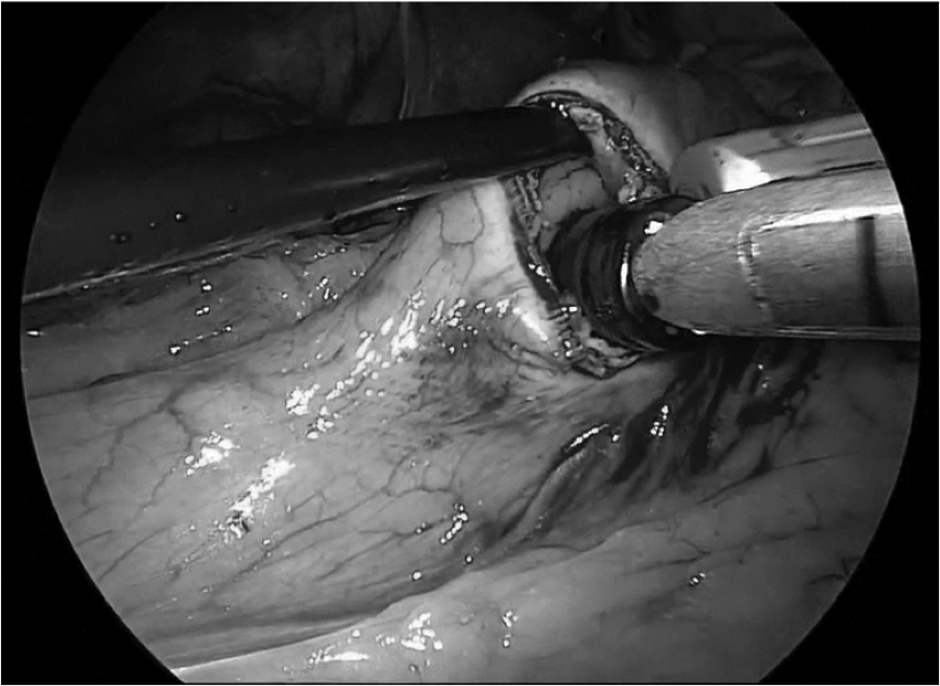
The endoscope passing through the gastrostomy. The stapler is guided into proper position by holding the tip of the endoscope with the jaws of the stapler.

Endoscopic view of the blade of the stapler passing through the stenosis.
Proper positioning of the stapler straddling the band.
The endoscope is passed through the gastrostomy again so that another staple load can be properly repositioned. Again, the blade of the stapler is passed into the gastric pouch, straddling the band and fired. This second fire serves to ensure band transection and enlarges the gastrogastrostomy between the gastric pouch and fundus to resolve the patient's dysphagia. The stapler is then removed and the gastrostomy is held closed by two graspers to allow endoscopic insufflation and full endoscopic evaluation of the gastric lumen (Fig. 10). The endoscope is then passed into the distal stomach and retroflexed to visualize the staple line. The endoscopic picture shows a retroflexed view demonstrating complete resolution of the stenosis (Fig. 11). If there appears to be continued narrowing or a large division between the pouch and fundus of the stomach, an additional staple load may be needed.
The gastrostomy is held closed to allow endoscopic insufflation after the band has been transected by the staplers.
Retroflexed endoscopic view showing staple line and resolution of the stenosis.
Once endoscopic evaluation is completed and staple line hemostasis is obtained, the gastrostomy is closed. Two to three full thickness 2-0 silk stay sutures are placed across the gastrostomy, and then a single staple load is used to close the opening (Fig. 12). The stomach is then endoscopically insufflated, and a leak test is performed. Saline is instilled into the upper abdomen, and the staple line is inspected for any air bubbling. If there is any question of a possible leak, the area is reinforced with interrupted vicryl sutures.

Closure of the gastrostomy using stay sutures and single staple load.
Next, the irrigation is suctioned out of the abdominal cavity, hemostasis is achieved, and final inspection of the operative field is performed. The trocars are removed, and the pneumoperitoneum is evacuated.
The patient is then admitted for observation overnight. A postoperative upper GI series is routinely performed the following morning to evaluate for leaks and improved passage of contrast into the distal stomach. The patient is started on a liquid diet the morning of postoperative day 1. If the diet is tolerated, pain is controlled with oral medications, and mobilization is sufficient, the patient is discharged home. The postoperative diet plan consists of 2 weeks of liquids followed by 2 weeks of a soft diet before progressing to regular consistency foods.
The patient is again extensively counseled on the importance of diet and exercise with regard to maintaining a healthy weight. Strict adherence to a portion-controlled diet and routine follow-up with a bariatric specialist or nutritionist will help manage the patient's weight postoperatively.
Conclusion
The technique described provides another option for revisional surgery for VBG in patients with adequate weight loss and intractable reflux symptoms or dysphagia. This method adequately relieves symptoms of reflux and regurgitation, and improves oral intake to allow nutritional requirements to be met without parental support. Though weight regain is a possible concern, this option allows improved quality of life and improvement in symptoms for patients who do not want or require further weight loss surgery.
Footnotes
Acknowledgments
The authors would like to acknowledge Edward Lin, DO, for his contribution to this operative technique. Nathaniel Lytle, MD, and Ankit Patel, MD, were supported in part by the Foundation for Surgical Fellowships.
Disclosure Statement
No competing financial interests exist.