
Abstract
Introduction:
This study aimed to review the mid-term results of laparoscopic sleeve gastrectomy (LSG) as a single one-stage operation for morbid obesity.
Methods:
We performed a retrospective analysis of prospectively collected data from November 2008 to August 2013. A total of 267 patients underwent LSG by a single surgeon at a single teaching institution. Data collected and analyzed included patient demographics, operative time, operative technique, length of stay, complications, learning curve, preoperative body mass index (BMI), and weight loss at 6 months, and 1, 2, 3, and 4 years.
Results:
The mean preoperative BMI was 47.6 kg/m2 and the mean age was 42.9 years. Mean operative time (100.3 minutes) significantly improved with increased experience. Patients with at least 6 months' follow-up were included to calculate weight loss (mean follow-up rate 46%). The mean BMI decreased to 36.2, 33.3, 33.3, 37.6, and 35.9 kg/m2 at 6 months, and 1, 2, 3, and 4 years respectively. Mean percentage excess weight loss (%EWL) was 54.3, 67.2, 58, 54.3, and 61 at 6 months, and 1, 2, 3, and 4 years respectively. We had three major complications (1.1%) and four minor complications (1.4%).
Conclusion:
LSG is a safe and effective procedure for achieving and maintaining acceptable weight loss for up to 4 years.
Introduction
L
Methods
Under Institutional Review Board approval, we performed a retrospective review of prospectively collected data from a cohort undergoing LSG at a teaching community hospital. All surgeries (267 operations) were performed by a single surgeon from November 2008 to August 2013, and were assisted by a senior surgical resident. Data collected and analyzed included patient demographics, operative time, coincidental hiatal hernia (HH) repair, surgical technique, length of hospital stay, complications, body mass index (BMI), and weight loss at 6 months, and 1, 2, 3, and 4 years. We compared the operative time and length of hospital stay between different subgroups, including LSG and LSG+HH repair. Operative time was also analyzed based on surgeon experience by dividing the groups into equal quarters. Patients who completed at least 6 months follow-up were analyzed for weight loss. Weight loss was expressed as change in BMI and mean percentage excess weight loss (%EWL). Using a BMI of 25, the ideal body weight was calculated based on the patient's height. Excess body weight was then calculated by subtracting the ideal body weight from the patient's initial weight. %EWL is then the percentage of the patient's weight loss divided by the excess body weight. Patients selected for LSG were based on the National Institutes of Health (NIH) consensus and included the following: age >18 years, BMI 35–40 with two comorbidities, BMI >40, and failure of medical and behavioral changes to achieve adequate weight loss. In our practice, we have no upper age or BMI limit set, as long as the patient would benefit from weight loss surgery and has an acceptable risk.
Descriptive statistics are presented as means and standard deviations for continuous data, and percentages for dichotomous and categorical data. Between-group comparisons for procedure groups were analyzed using a one-way analysis of variance (ANOVA) with Bonferroni adjusted post-hoc group comparisons for the three groups. Analysis was performed using SPSS v21 (IBM Corp., Armonk, NY) and statistical significance was determined at p≤0.05.
Surgical technique
After induction of anesthesia and endotracheal intubation, the patient is placed in supine position with a Foley catheter in place and a footboard at the bottom of the table. Surgery is performed in the supine position with three working trocars (two 5 mm and one 12 mm for the stapler) and another trocar for the camera. The 12 mm trocar is placed on the patient's right side to allow for insertion of the linear stapler. The liver is retracted cranially using a Nathanson retractor. The omental attachments are taken down starting approximately 5 cm from the pylorus along the greater curvature toward the left crus. We thoroughly evaluate for the presence of hiatal hernia (HH) and repair anteriorly the smaller asymptomatic ones (<2 cm) and posteriorly for larger ones (we typically place an absorbable mesh in these cases). Stapling is performed along a 34 fr bougie without being tight against the bougie, especially at the incisura and the angle of His. We use gradually decreasing cartridge thickness starting with the black cartridge, gradually decreasing the size to green load, then gold, then blue cartridges for the remaining staple line. The entirety of the staple line is reinforced using SEAMGUARD® (Gore Medical, Flagstaff, Arizona), which is placed prior to each staple fire. Upper endoscopy is performed routinely to assess for staple leak, bleeding, assess the lumen, and rule out any inadvertent remaining fundus. Specimens are extracted easily from the 12 mm trocar site without the need for a bag with minimal dilation of the fascia, which is typically repaired. All patients are admitted overnight with upper GI contrast study performed the following morning and planned for discharge on postoperative day 1 as per protocol.
Results
We performed 267 LSG from November 2008 to August 2013. Mean preoperative BMI was 47.6±8.0 kg/m2 and mean age was 42.9±10.3 years. All cases were successfully completed laparoscopically without any conversions. The mean operative time (skin incision to close time) for all LSG completed was 100.3±37.3 minutes. The mean operative times of the LSG alone and LSG+HH repair were 106.0±39.4 and 92±33.1 minutes respectively (Table 1). We found a statistically significant difference in the operative time between the LSG group and LSG+HH repair group (p=0.01).
LSG, laparoscopic sleeve gastrectomy; HH, hiatal hernia; LOS, length of stay.
The mean length of hospital stay for all patients was 1.6±0.7 days. There was no significant difference in the length of stay between the LSG+HH group and the traditional LSG (Table 1).
There was a significant improvement in the operative time when the cases were divided into four groups (Fig. 1). We showed with statistical significance (p<0.001) a decrease in the mean operative time with every quarter of our experience (130.2±39.6, 104.9±26.5, 87.9±30.8, and 78.1±28.4 minutes respectively).
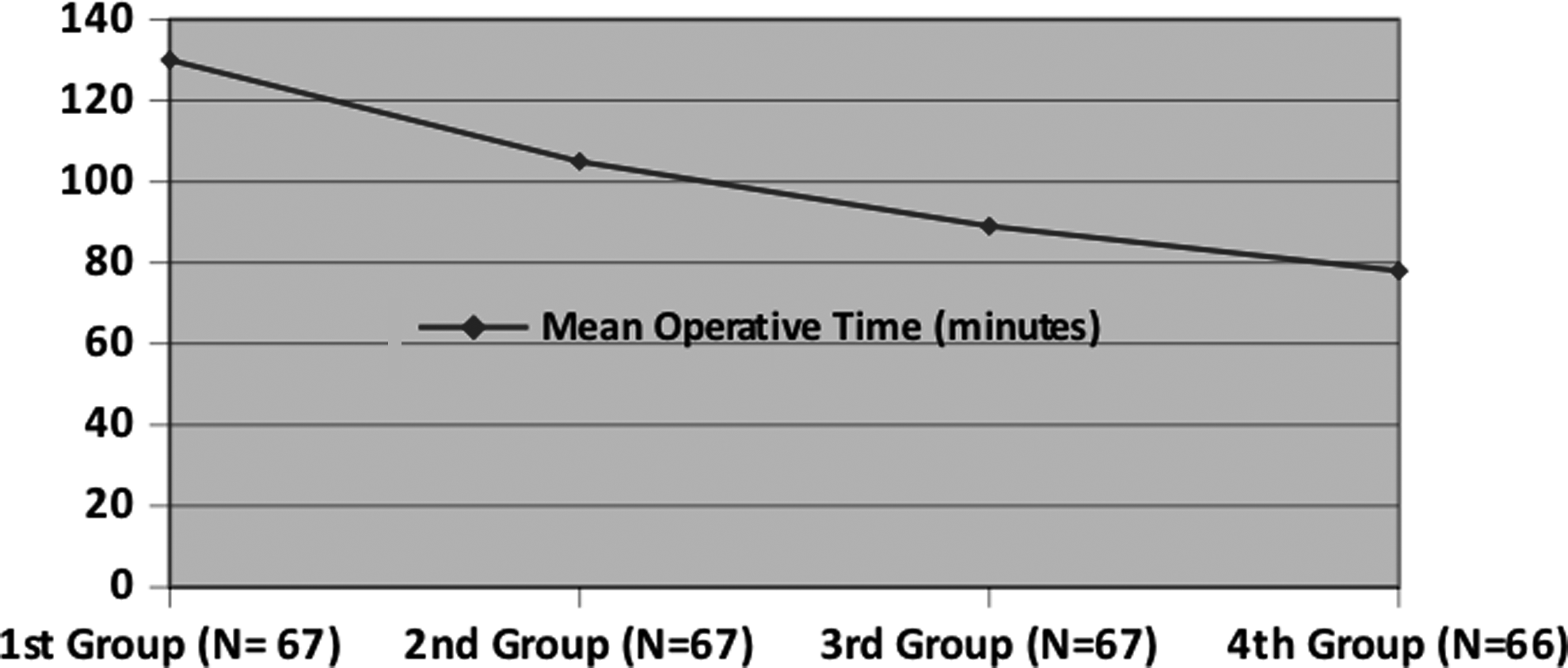
Mean operative time divided into quarters.
The mean preoperative BMI of all patients was 47.6±8.0 kg/m2. Patients with at least 6 months follow-up were included to calculate weight loss. The mean BMI was 36.2±6.8, 33.3±6.8, 35.1±7.8, 37.6±9.4, and 35.9±10.7 kg/m2 at 6 months, and 1, 2, 3, and 4 years respectively (Table 2). The %EWL was 54.3±16.6, 67.2±21.9, 58±0.3, 54.3±27.9, and 61±0.3% at 6 months, and 1, 2, 3, and 4 years respectively (Fig. 2).

Mean percentage excess weight loss (%EWL) over a 4-year period.
BMI, body mass index; %EWL, mean percentage excess weight loss; SD, standard deviation.
We had a total of seven complications (2%). One leak (0.4%) presented on postoperative day 5 and was managed with laparoscopic washout and drainage with suture repair of the leak (found with intra-op endoscopy at the angle of His). This patient was a smoker and did well without long-term complications. One patient had postoperative bleed evident from postoperative tachycardia and a drop in hemoglobin. Laparoscopic exploration was performed with the patient being hemodynamically stable and showed intra-abdominal hematoma without any active bleed. The site of bleeding was never confirmed but was thought to be from the omental cut edge. This patient left hospital the day after exploration (POD#2 from her sleeve). One patient had deep vein thrombosis (DVT; 0.4%). This patient had known history of previous PE and IVC filter who failed to comply with our postoperative anticoagulation protocol with Enoxaparin. Two patients (0.7%) had strictures: one at the GE junction and another 7 cm from the GE junction requiring EGD and balloon dilation. Both patients presented with poor PO tolerance after 2 weeks and 1 month. Both responded well to two sessions of dilation. One patient had wound infection of the specimen extraction wound (0.4%) requiring incision and drainage at bedside. One patient had trocar site (12 mm trocar) hernia (0.4%) requiring reoperation and repair due to incarceration of intestine. This occurred before we started to repair the specimen extraction site routinely. We did not have any mortality, and there was no conversion to open procedure.
Discussion
Sleeve gastrectomy was initially introduced as the first step of a staged procedure followed by duodenal switch 7 or a Roux-en-Y gastric bypass. 2 As with many bariatric procedures, it was quickly adopted laparoscopically with acceptable results and improved patient satisfaction. 8 The logic behind staging these operations was to decrease the high morbidity and mortality rates of the complex procedure that were often associated in the mega-obese patient population. LSG then was postulated as a standalone restrictive procedure due its good initial weight loss 9 with promising effective results in mid- and long-term follow-up periods. In a review of long-term weight loss results after LSG, Diamantis et al. found that the overall mean %EWL at 5 or more years was 59.3%. 10 In a follow-up after LSG at 8–9 years of 13 patients, Sarela et al. found that the median %EWL was 68%. 11 LSG offers technical advantages over traditional LRYGB and LGB, including lack of intestinal manipulation and anastomosis, pylorus preservation, lack of foreign object implantation, and no risk of internal hernias. Although conceptually safe and appears simple, it is an operation with many subtleties with the need for attention to detail for the best outcome. Many complications in this operation do exist, and some, such as leaks and severe strictures, could be very difficult to manage.
This study is a large single-surgeon initial series of LSG and includes the entire experience, thus limiting selection bias. In this study, %EWL at 6 months, and 1 and 2 years were 54.3%, 67.2%, and 58%, which are similar to other published short- and mid-term follow-up series. Lee et al. and Rosenthal et al. reported higher EWL at the 2-year follow-up of 83% and 67.9%.9,12 Our 2-year follow-up is unacceptably low, which is partly due to large cohort of patients being from out of state. We increased our ancillary staff later on in our practice to reach out and improve our follow-up, which is shown by our higher 3- and 4-year follow-up rates.
Himpens et al. published more than six years of results on weight loss in a cohort of 30 patients with a %EWL of 53.3%. 6 Bohdjalian reported similar results in 5-year follow-up of 55%. 13 Yet there have been reports of weight gain between the third and sixth years. This does not seem to be our experience, although our long-term follow-up is low to reach this conclusion. Late weight regain may be due to many factors, including technical difficulties with sleeve dilation or behavioral and dietary issues.
While many advocate for a second-stage operation, feeling that the sleeve is not an adequate standalone operation, Himpens et al. noted in their series that weight regain coincided with the interruption of the office visits after 3 years. 6 This confirms that poor follow-up rather than surgical issues are likely to play a major role in weight regain. As for the concern that the sleeved stomach might dilate over time, Himpens et al. did confirm the formation of “neo-fundus” on some late postoperative upper GI series. 6 It is still unclear as to how many of these “neo-fundus” are related to poor upper dissection and removal of the fundus at the time of the initial surgery.
In terms of surgical learning curve, our data suggest that the LSG is mastered early in the cohort. When the total cases were divided into four groups chronologically, there appeared to be a statistical improvement in mean operative time: 130.2, 104.9, 87.9, and 78.1 minutes. Also attributing to the mastery of the procedure, the two major complications, staple-line leak and hemorrhage, occurred among the initial patients. The staple-line leak occurred in patient number 7, and the hemorrhage occurred in patient number 14. Our practice evolved through experience. This evolution was responsible for our low complication rate as we addressed the adverse events.
We always felt that the logic sequence of cartridge type should follow the change of gastric wall thickness. We have always gone from stapling the antrum with a green load followed by yellow then blue load. When the black load became available about 100 cases into our practice, we changed to fire it first at the thickest part of the antrum. Although we initially used 34 fr bougie, we changed after our first leak (case #7) to leave a distance of a few millimeters from our stapler. This is especially at the incisura to prevent outflow resistance (indirect cause of a higher leak) and at the highest firing where we leave about 5–10 mm to prevent stapling esophageal tissue that does not heal as well. This, we believe, is in part the reason we have not had leaks since. In addition, we stopped performing this operation on smokers, as the leak occurred on a smoker. We believe that strictures occur mostly from twist of the staple line instead of having a smaller bougie. We prevent this by always checking the back wall before firing the stapler and apply equal lateral traction on both the anterior and posterior wall. Prevot et al. suggested that the LSG technique is mastered after 30 cases by concluding a statistical significance in the mean operating time between the first chronological 30 patients and the next 30 patients (139 vs. 93 minutes), while also showing a statistical significant improvement of %EWL at 5 years between the two groups (34% vs. 48%). 14
In this study, we found that, against expectations, the mean operative time of LSG+HH was significantly lower than in the LSG alone (106 vs. 92; p=0.01). These numbers, however, represent an improvement in our technique with faster operative time and more investigation of HH. In fact, the prevalence of HH increased with our experience. In the first half of the series, 21% of cases involved repair of a HH, whereas 57% of cases involved repair of a HH in the last half the series. The significantly shorter operative time in the LSG+HH group is likely a reflection of the learning curve and not a reflection of the additional repair. Increasing literature appears to describe the sleeve as a reflux-inducing operation. This led us gradually to be more aggressive in investigating for HH and in repairing any defect, even if very small (dimple of the hiatus). We do not know if this had any positive impact on postoperative reflux. In our experience, we did not see the sleeve leading to GERD, although this is based on symptoms only without any objective measurement of distal acid exposure. Most HH were small and were repaired anteriorly. Posterior repair was performed only for patients with hernias >3 cm or for smaller but very symptomatic ones. A total of 12 out of 118 hiatal hernia repairs (10%) were repaired posteriorly with placement of mesh. We do not have objective measurement of acid exposure, but we continue following these criteria for repair based on our positive results from a reflux standpoint.
There was no clinical difference in the length of stay between the two subgroups. This was not unexpected, as we found that what keeps patients past the first postoperative day (which is our routine discharge day) is mostly nausea and occasionally heartburn. We do now, however, see more success with POD1 discharges, which we believe is largely due to eliminating narcotic patient controlled analgesia (PCA), which almost eliminated severe postoperative nausea (the main reason for staying an extra night). We have now moved to a combination of intravenous (IV) acetaminophen (starting with a preoperative dose in the holding room) and IV Toradol. We believe we will see significant impact as more cases are done. Incisional pain has not been an issue with our patients and certainly has not delayed any discharge. Patient education and correct expectations play a major role in timely discharge. In this study, seven (2%) complications occurred. In other similar studies, the perioperative complication rates ranged from 3% to 15%.6,12–19 In our cohort, there was only one staple-line leak (0.4%). In comparison to other studies, the incidence of staple-line leak ranged from 0.7% to 5.5%. This low incidence is encouraging and likely to be multifactorial related to surgical technique and patient selection. The efficacy of using buttressing in decreasing staple-line leaks is still debatable, 20 but has shown in animal studies to increase pressure resistance at the level of the stapler line, along with hemostatic properties. 21 In our study, only one patient had a postoperative thrombotic event. The low rate of thrombotic event may be due to early ambulation and preoperative subcutaneous Enoxaparin use, extended in severely obese patients (BMI > 50) for 2 weeks postoperatively.
Conclusion
LSG is a safe procedure with a minimal rate of complications in experienced hands and with satisfactory short- and mid-term weight loss. Operative time and hospital stay are shorter than most bariatric operations, a factor that may encourage many fearful patients to come forward for surgery.
Footnotes
Author Disclosure Statement
Rami E. Lutfi is a consultant for Ethicon Incorporated, Gore Medical, and Olympus Corporation. Tareq Q. Kamal and Pey-Yi K. Lin have no conflicts of interest.