
Abstract
Background:
The size and shape of the stomach are variable among individuals and conditions, so an individual three-dimensional (3D) stomach model is important when planning bariatric procedures. If the stomach is aerated to a certain level by endoscopy and the internal space is measured, a 3D stomach model can be constructed precisely. In this study, we constructed a 3D model of the stomach using endoscopy and planned tailored bariatric procedures.
Methods:
Three patients underwent esophagogastroduodenoscopy. The stomach was aerated to the predetermined level, and internal dimensions were measured using regularly marked endoscopic guidewire. Three-dimensional stomach models were constructed using this information, and individual stomach volumes were calculated. We also planned a simulated sleeve operation or endoluminal bariatric gastroplasty for predetermined volume reduction.
Results:
The stomach volume of each patient was acquired and intertemporal variation was calculated. The resection line for sleeve operation and suture lines for endoluminal gastroplasty were planned. Expected volume and shape change after the procedure were obtained.
Conclusion:
A patient's stomach volume and shape are important information in surgical or endoscopic volume restrictive procedures. These data can be used for the prediction of treatment response, complications, and prognosis. In the absence of techniques for individualized 3D stomach modeling and volume estimation, this procedure would be an important basic step for future tailored bariatric procedures.
Introduction
B
If the stomach is aerated to a certain level and the internal dimensions are measured during routine esophagogastroduodenoscopy, a three-dimensional (3D) model of the stomach can be constructed precisely. In this study, first we constructed an individualized 3D stomach model using endoscopy. From this model, we were able to calculate each individual's stomach volume and plan individualized bariatric procedures using 3D simulation software.
Materials and Methods
Three patients underwent esophagogastroduodenoscopy for screening or diagnostic purposes. The stomach was aerated to the level where the gastric folds of greater curvature are distended sufficiently to check for entire mucosal lesions. Measurement of internal dimensions was performed using regularly marked endoscopic guidewire (Hydra Jagwire™ High Performance Guidewire; Boston Scientific, Natick, MA). The stomach was divided into four major compartments (fundus, body, pyloric antrum, and pyloric canal; Fig. 1), and internal dimensions critical for determining stomach volume were measured (Fig. 2 and Table 1). From these data, we made a 3D model of the stomach for each patient and calculated the stomach volume. Another gastroenterologist repeated the same procedure 1–2 months later to check the reproducibility of the volume estimation. With these 3D reconstructed stomach models, we could simulate sleeve gastrectomy or endoluminal bariatric gastroplasty for a predetermined volume reduction. Three-dimensional stomach model construction and a simulated bariatric procedure were performed by Cinema4D R12 (MAXON Computer, Friedrichsdorf, Germany).
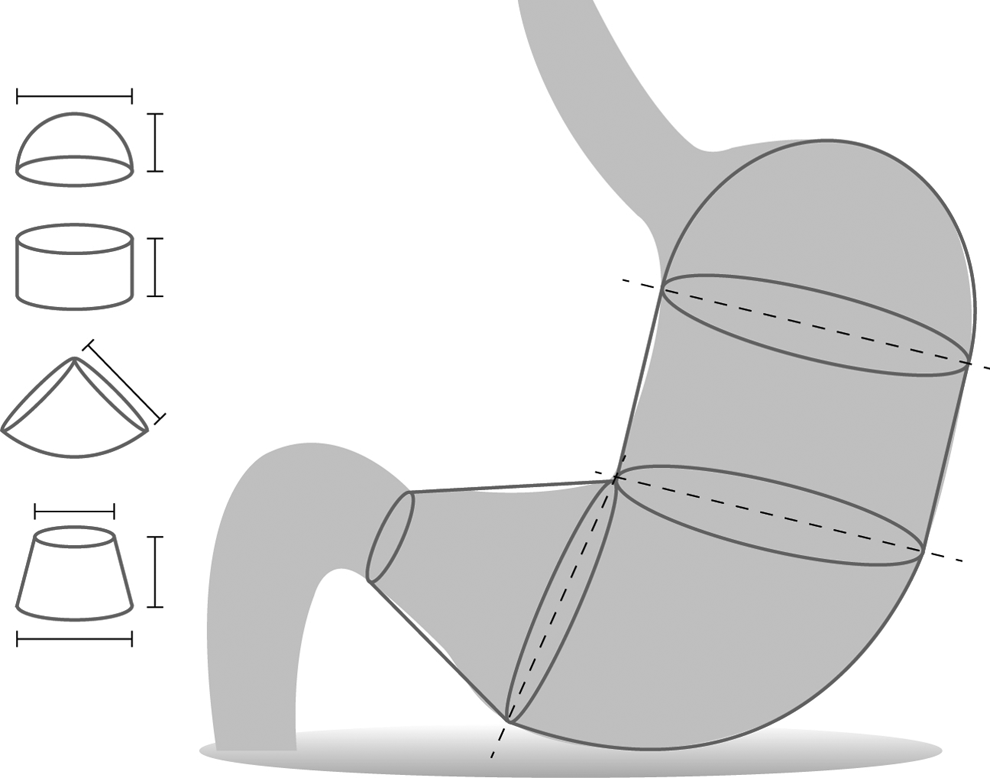
Schematic view of four stomach compartments used for three-dimensional (3D) construction and volume estimation. The stomach was divided into four compartments arbitrarily, and internal dimensions were measured by endoscopic guidewire.
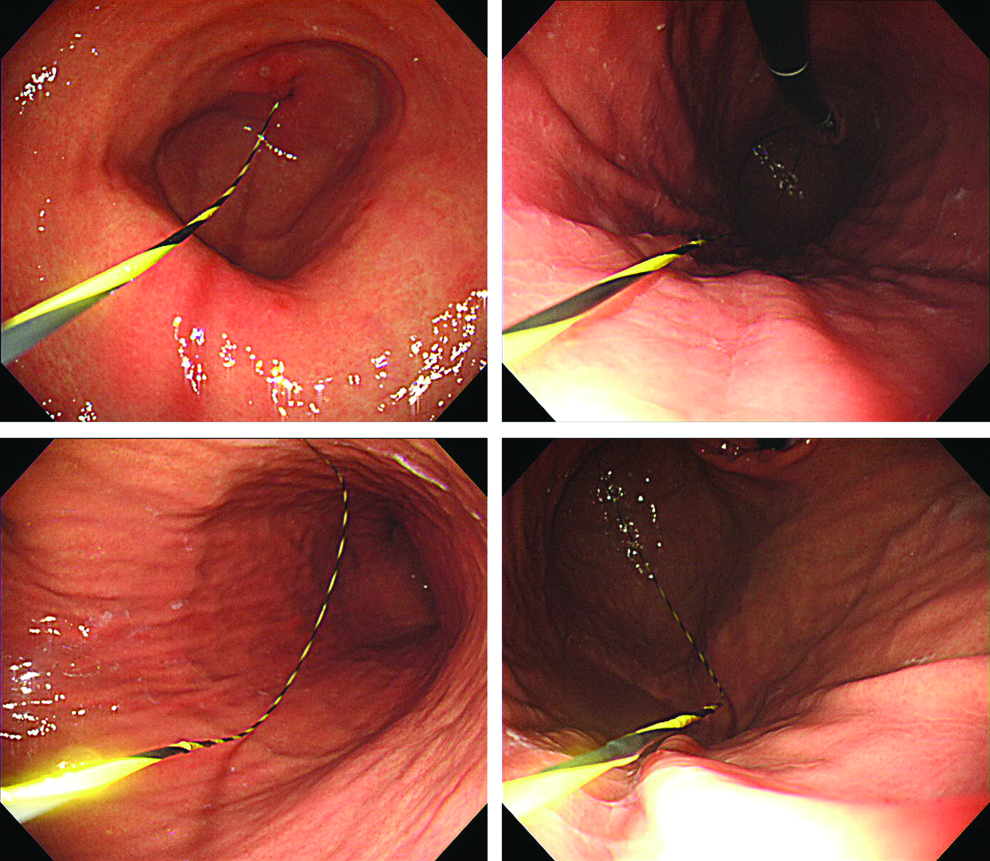
Measurement of stomach internal dimensions for constructing a 3D model and determining stomach volume. During endoscopic evaluation, guidewire was used for determining the length of the predetermined region. Color images available online at www.liebertpub.com/bari
Results
3D reconstructed stomach models
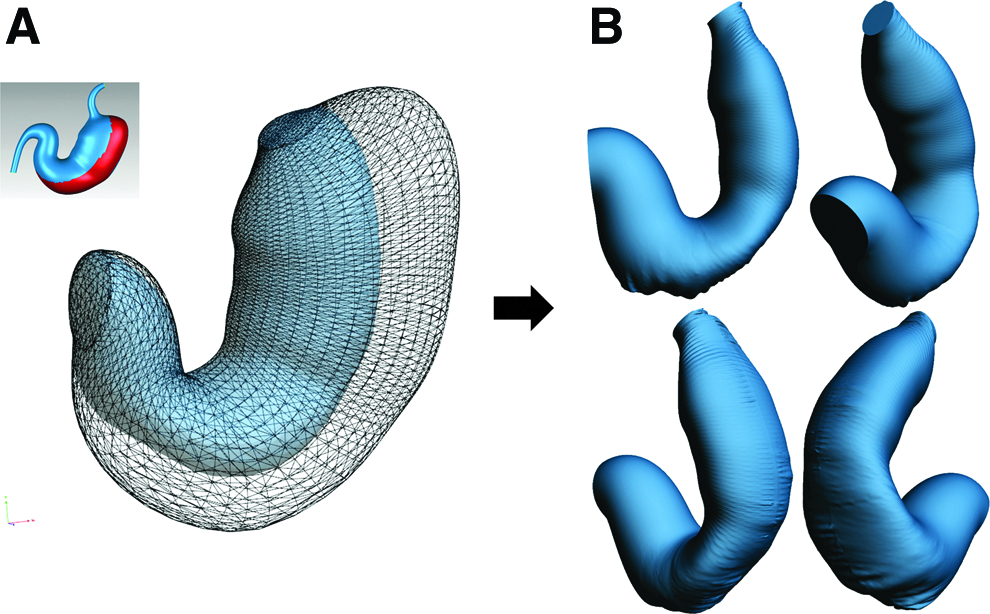
Three patients underwent esophagogastroduodenoscopy (Table 2). Three-dimensional stomach models were constructed using the measured size and shape information obtained during the endoscopy (Fig. 3). From these constructed 3D stomach models, we could calculate the stomach volume for each individual (Table 3). The same patients underwent esophagogastroduodenoscopy 1–2 months later, and 3D stomach models were constructed using information acquired during the second endoscopy. Intertemporal variations were calculated based on data previously acquired in the first endoscopy, which were around 10% of the original stomach volume (Table 3). From this result, we can assess the precision or reproducibility of this method for measuring individual stomach volume.

Three-dimensional constructed individual stomach model of three patients
GERD, gastroesophageal reflux disease.
Personalized virtual bariatric procedures using 3D stomach models
Sleeve gastrectomy is often performed for morbidly obese patients. This procedure removes the main part of the fundus and body with the goal of reducing remnant stomach volume to be 100–200 cc regardless of the patient's condition.21,22 We applied virtual sleeve gastrectomy to the reconstructed 3D stomach model to reduce stomach volume to the expected level. We designed a sleeve gastrectomy resection line aimed to reduce stomach volume to 40% of the original size (Fig. 4A). After performing virtual resection and stapling through the planned line, the calculated remnant stomach volume was 36% of the original stomach (Fig. 4B and Table 4). From this attempt, we could simulate sleeve gastrectomy and calculate the expected volume change after surgery, showing the possibilities of planned sleeve gastrectomy with the anticipated volume change.
Sleeve gastrectomy aimed for 60% of volume reduction.
We also simulated endoluminal bariatric gastroplasty for predetermined intraluminal volume reduction using a novel endoscopic suture device developed by our group. 23 The successive suture lines were planned for this procedure (Fig. 5 and Table 5). Three-dimensional stomach models after planned endoscopic suture were constructed, and volume changes were calculated (Fig. 6). About 15% volume reduction was achieved after four stitches (Table 6). When we applied similar successive four stitches one more time, 30% volume reduction could be achieved (Table 6).
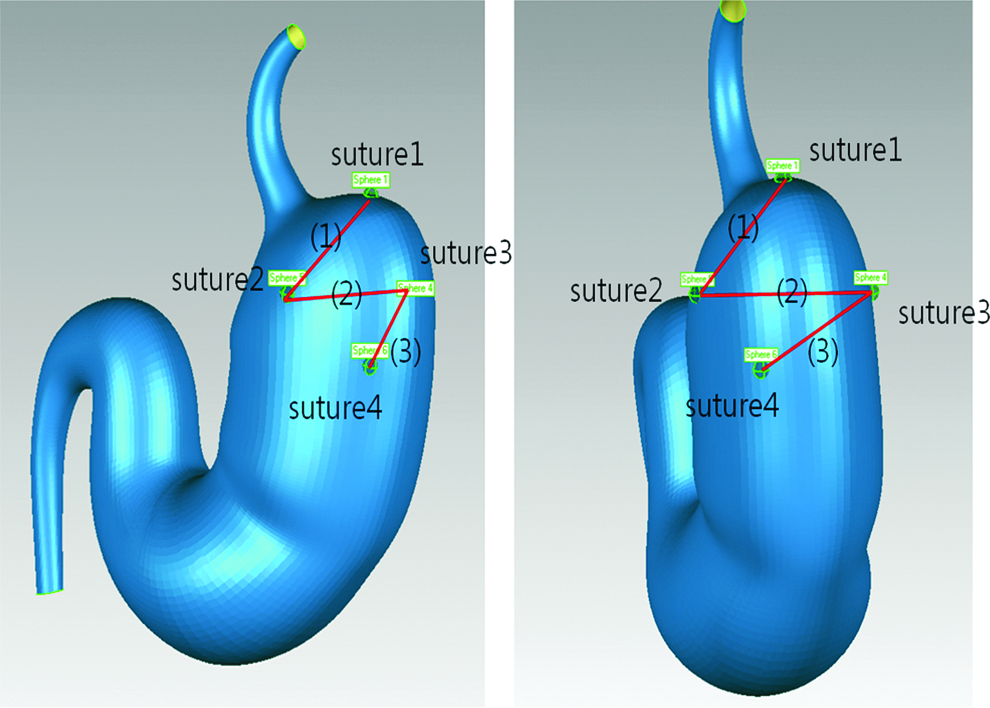
The planned suture lines for endoluminal bariatric gastroplasty using novel endoscopic successive suture device. Successive suture lines in the order (1), (2), and (3) were planned for bariatric gastroplasty. Color images available online at www.liebertpub.com/bari
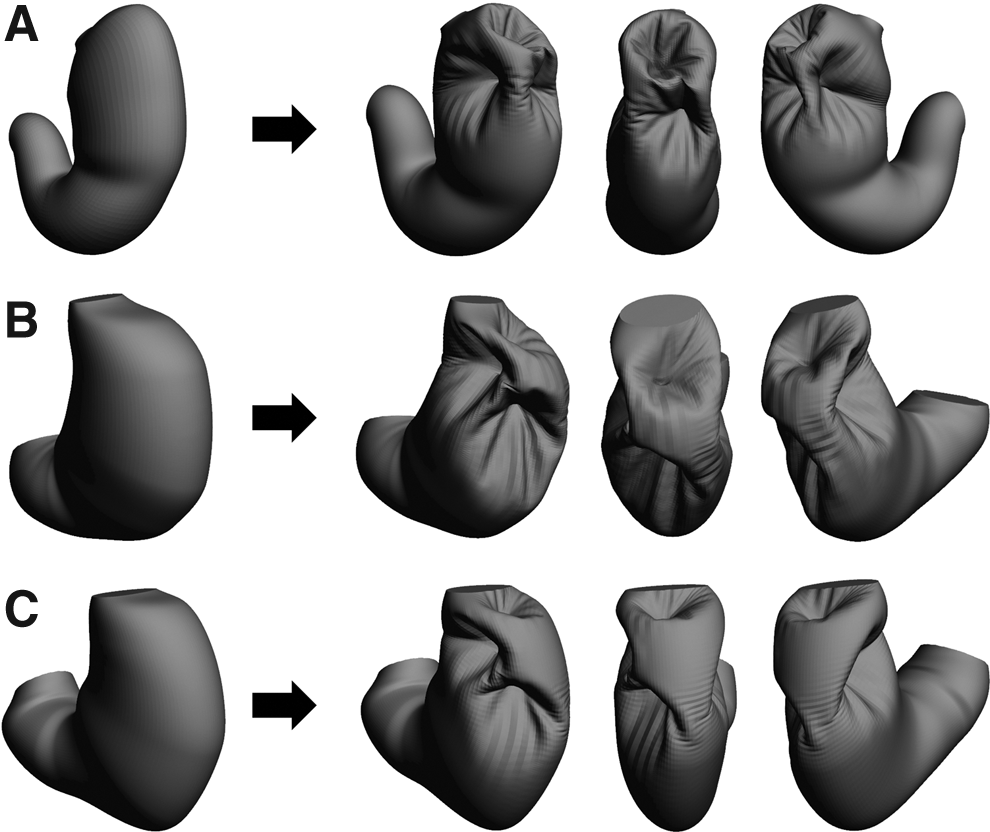
Endoluminal bariatric gastroplasty using an endoscopic suture device. The successive suture lines were planned as for Figure 5, and simulated stomach models after endoluminal bariatric gastroplasty were constructed using 3D simulation software for three patients (
Discussion
Obesity is increasing continuously, and bariatric surgical procedures are frequently performed. Recently, endoscopic bariatric procedures have emerged as a new treatment option for obesity as well as metabolic disease.14,24 In the stomach volume restrictive procedures, data about individual stomach volume, shape, and volume change after procedure are very important parameters for planning procedures and predicting treatment response. However, up to now, measuring personal stomach volume and shape has been difficult due to several limiting factors such as variations among individuals and various biological factors that can affect stomach geometry. This is the first study that has attempted to obtain information about individual stomach volume and shape reproducibly, and that has applied this information to make a plan of bariatric procedures for individually optimized treatment.
In this study, we could produce a 3D stomach model for each patient relatively precisely, even though 100% accuracy was not achieved. Constructed 3D stomach models were useful for planning and simulating bariatric procedures such as sleeve gastrectomy or endoluminal gastroplasty using an endoscopic suture device. We could also predict volume and shape change after procedures with this information. This kind of work may have a critical role in future tailored bariatric procedures.
Even so, our study has several limitations. Internal stomach dimensions were measured manually by an endoscopist, so interpersonal variations may affect the accuracy of these measurements. This issue can be addressed by incorporating new technologies to the endoscopy such as laser scanners or 3D surface reconstruction technology from image sequences.25,26 In addition, stomach aeration to allow sufficient distension of gastric folds in the body, greater curvature side is not an absolute objective condition, but we believe this is the best method for reproducible stomach modeling so far. Our method is based upon the assumption of a normal stomach configuration, so there are limitations in 3D stomach modelling for a deformed stomach such as that of postgastrectomy patients and severe peptic ulcer disease. This problem can be overcome by introducing the up-to-date 3D rendering methods mentioned above.
If we can accommodate 3D rendering technology with the current endoscopic equipment, accurate stomach shape and volume data can be applied not only to bariatric procedures but also many other disease entities. For example, the relationship between stomach volume or shape and functional gastrointestinal disorder, obesity, or gastroesophageal reflux diseases (GERD) will be interesting subjects for future research. Furthermore, we expect these data will help facilitate establishing a guideline on optimal bariatric procedures with maximal weight losing effect and minimal adverse effects.
Conclusions
In this study, construction of personal 3D stomach models was possible. These data were useful in planning optimal bariatric procedures, and individual stomach volume could also be calculated from these models. In the absence of techniques for individualized 3D stomach modeling and volume estimation, this procedure would be an important basic step for future tailored bariatric procedures.
Footnotes
Acknowledgments
A portion of the data in this manuscript was presented at the Digestive Disease Week 2014 meetings in Chicago, IL. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean Government (NRF-2014R1A2A2A01006131) and Grant of Korea University.
Author Disclosure Statement
No competing financial interests exist.