
Abstract

T
I will present evidence and explain why the band has declined in use and should no longer be considered as the procedure of choice for obesity. First, consider the U.S. Food and Drug Administration (FDA) study, 2 which had adverse events data. 3 When patients were at 6 years post-surgery, 28% of banding devices were explanted; weight loss was only 18% of initial body weight. See Figure 1 for body mass index (BMI) changes in post-band patients over time.
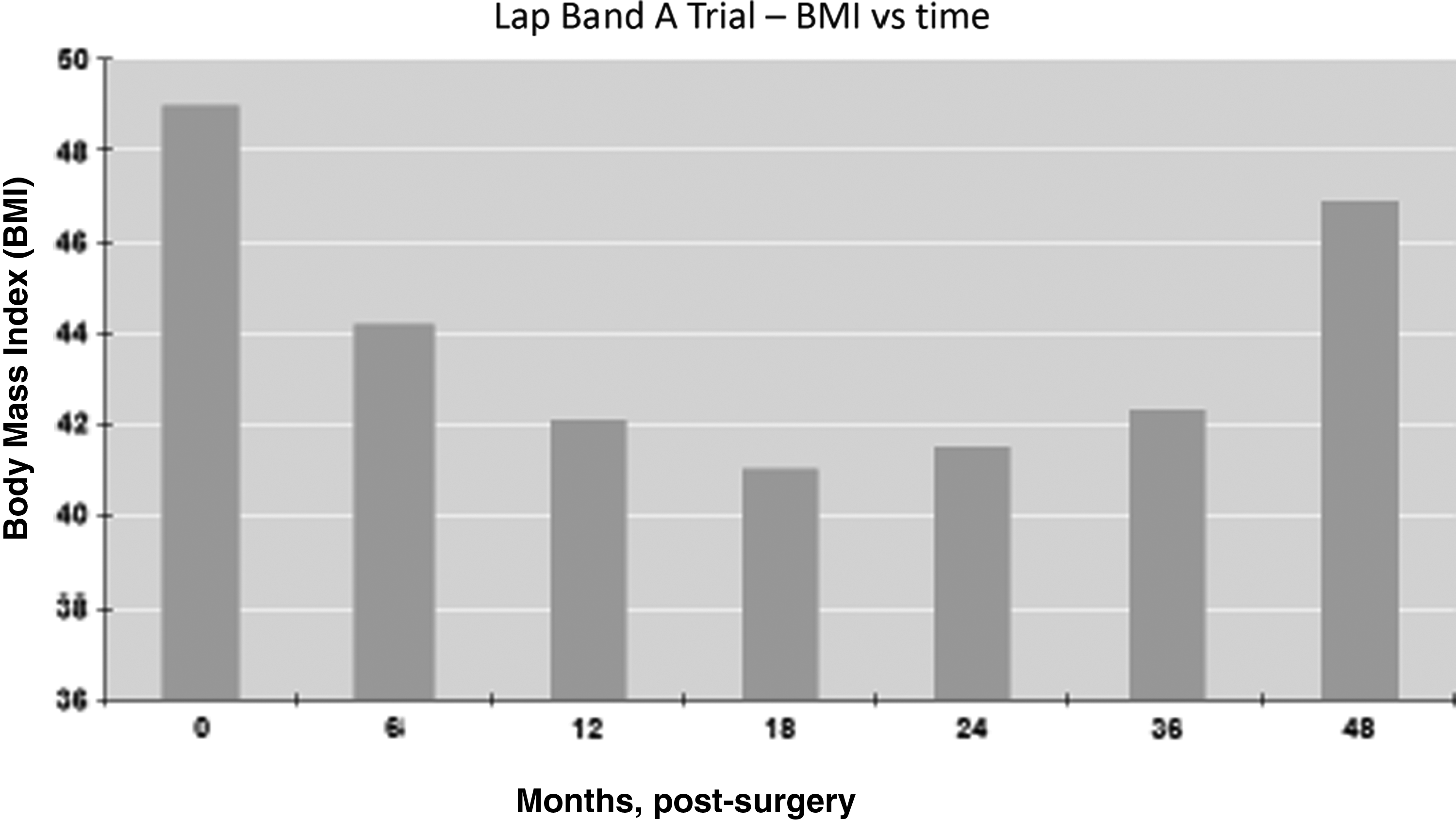
Mount Sinai patients from Food and Drug Administration (FDA) Lap-Band A trial. Courtesy of Dr. Gagner.
A problem with analyzing results from the A trial was that it took several years for patients to realize that they didn't like the Lap-Band. At first, the patients may have had issues, but they kept working at it, and then 4 or 5 years post-surgery, they would opt to have it removed. So when you present your data too early, the later problems are not reflected.
Another issue with the band is that the FDA advisory panel never initially recommended it. In the year 2000, by a 6-4 vote, the FDA advisory committee concluded there were insufficient data to determine whether the device, called Lap-Band, was safe and effective. 4 But, by some mystery, a few months later, the band was approved.
Looking beyond the United States, European countries are removing bands at a record rate. I'm told now that sleeve gastrectomy has come to be the most frequently performed procedure in France. In Belgium, Jacques Himpens provides a 10 year review, from 1998 to 2008 5 (Fig. 2), and the numbers clearly show a steep decline in band placements.
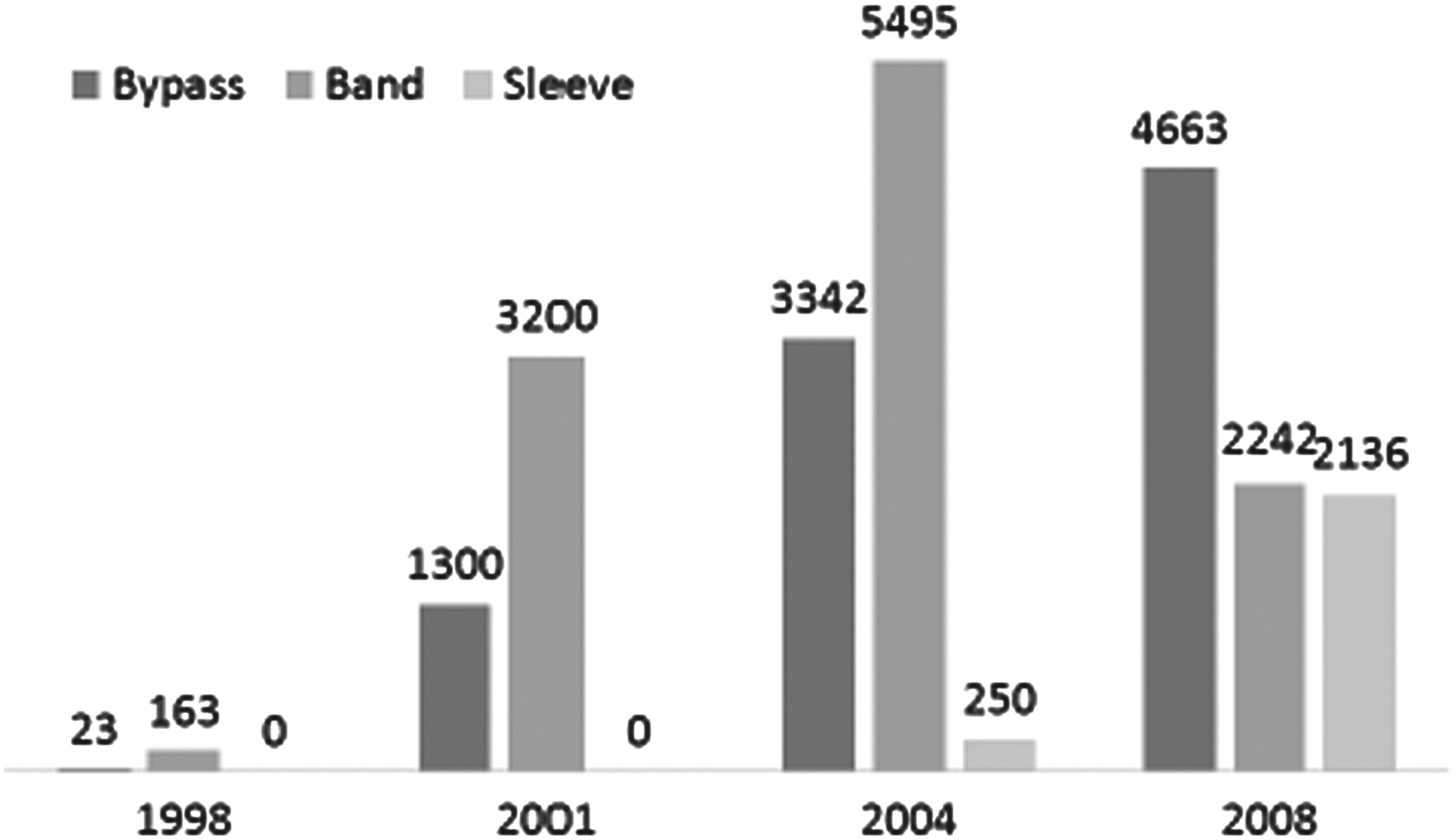
Bariatric surgery in Belgium. Courtesy of Dr. Jacques Himpens.
Dr. Suter in Switzerland has looked at the 10 year experience of laparoscopic gastric banding, including long-term complications and failure rate. 6 The failure rate of patients, defined by Dr. Suter's study as an excess weight loss (EWL) of <25% or major reoperation, was 36.9% at 7 years post-surgery, with each year after surgery adding 3–4% to the major complication rate.
There is another issue with the Lap-Band. Mortality and morbidity rates are often measured at 30 days post-surgery, but when you look at mortality beyond 30 days, there are more deaths for various reasons. I have data showing that two-thirds of mortality due to LAGB happen after 30 days, 7 and it's likely to be even more when you include reoperation, revisions, and conversions to other operations (Fig. 3).

Causes of all mortalities from laparoscopic adjustable gastric band (LAGB). GI, gastrointestinal, PE, pulmonary emboli. Courtesy of Dr. Gagner. Color images available online at www.liebertpub.com/bari
Ten years ago, we did a study comparing best medical practices of banding versus best medical practices of gastric bypass. Whatever the BMI range, the weight loss was dramatically better with bypass than banding. 8 A randomized study in the United States by Dr. Ninh Nguyen also showed that gastric bypass has better weight loss results than banding.
There was a randomized study by Dixon for treating diabetes by comparing the band with best medical treatment. 9 The interesting thing—and one I have never seen reproduced—was the 73% complete remission of diabetes for the band patients. I think that sometimes people interpret “complete remission” of diabetes differently. Not even Phil Schauer's study comparing gastric bypass or sleeve gastrectomy to best medical management had 73% diabetes remission. 10
In addition, conversions after banding are increasing and can be quite complicated. In our own experience, band removal occurred in 29% of cases and conversion in 43%. 11 There is a study that is about to be published dealing with conversion of banding to sleeve gastrectomy in 300 patients by Dr. Patrick Noel of France. The percentage of excess weight loss five years after the conversion is between 75% and 80% (pers. comm.).
With banding, making adjustments is perpetual. The fluid volume undergoes spontaneous diffusion through the membranes all the time, so you have to replenish the fluid for a lifetime.
In terms of economics, Dr. Ninh Nguyen looked at the cost of gastric bypass versus adjustable banding and found that gastric bypass was only $1,500 more than banding. 12 From these perspectives I have highlighted, banding should be abandoned.
Now, that's partly true. I'd like to discuss this in a bit more detail before I get into whether we should expect the bypass or sleeve to take over.
I will rely on data that Henry Buchwald has provided to us. He has done an excellent job with three studies, giving us the data from 2003, 2008, and 2011. The world data that he published recently in Obesity Surgery does show a slight decrease in bypass operations. 13 It shows a fairly sharp increase in sleeve gastrectomy, and quite dramatic decrease in the band.
However, if we look at the total number of bariatric surgeries, there are decreases across all types of procedures. If we look at just the United States, where there is better quality data by and large, we see that in the 1990s not much was happening, and then there was very rapid growth (Fig. 4).
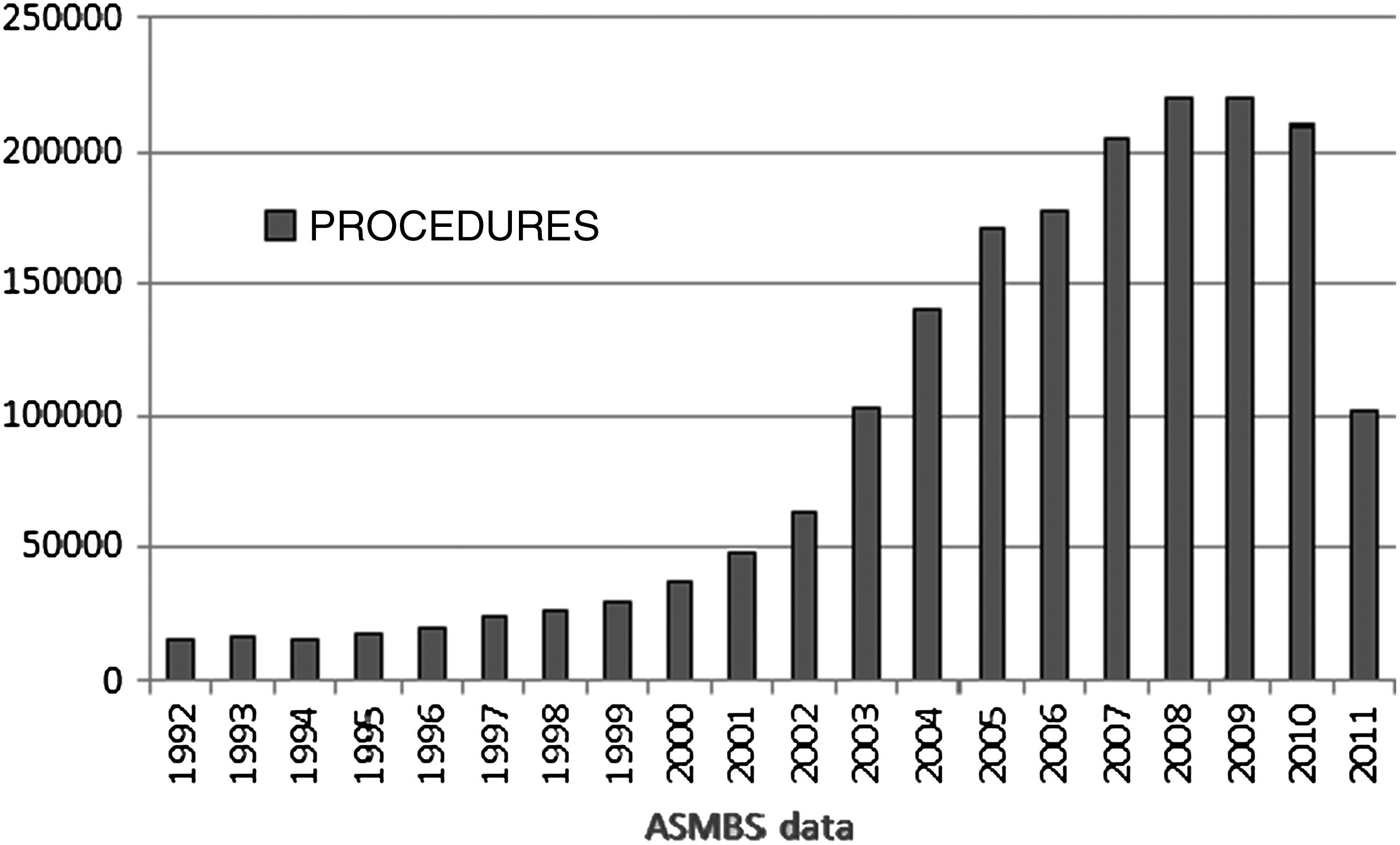
Total bariatric procedures in the United States 1992–2011. ASMBS, American Society for Metabolic and Bariatric Surgery. Courtesy of Dr. O'Brien.
The highest growth rate was in 2003, and it reached a peak in 2008 of around 224,000 cases per year. But since 2008, the numbers have been declining. In fact, Henry Buchwald's data at 2011 show a very sharp decrease in total procedures.
These numbers are a bit worrisome. In 2008, there were 217,800 cases in total in the United States, of which 112,200 were bypass and 96,800 were laparoscopic adjustable gastric band (LAGB). If we look at the changes that occurred, there was a decrease of 64,409 bypass procedures in the United States between 2008 and 2011, according to Henry Buchwald's data. However, the band decreased by 69,170, only a little bit more than the gastric bypass.
Then the sleeve gastrectomy—and I quote Michel saying it has seen “exponential growth”—has actually gone from a mere 8,800 cases up to 19,486. This is fewer than 11,000 new cases. We're not replacing the 123,000 cases we've lost. So we're looking at something that is a tiny fraction of what we need to handle the world's problem with obesity.
We have 500 million people around the world who are obese. We have approximately 80 million people in the United States who are obese, and we're only treating this tiny little sliver (Fig. 5).

The impact of bariatric surgery on the global problem of obesity, 2011. Courtesy of Dr. O'Brien.
I don't think any of us should be all that comfortable at this stage about how bariatric surgery is trending.
Now let us examine what's happening to the band. Think about what you want, what your patient wants, and what the community wants from bariatric surgery. The patient is going to want something that's very safe, minimally invasive, with no or minimal anatomic changes, modest discomfort, and that is affordable.
The clinician wants substantial weight loss that's sustained and wants to see many secondary benefits in health, quality of life, and survival. They want data, not from anecdotes, and not from some observational study that was done 12 or 15 years ago. They want data from good, quality, randomized controlled trials. Administrators and healthcare providers want to have good healthcare at reasonable cost, and they want to have something that they can handle, that is feasible, and that they have the resources to do.
I just want to show a couple of examples of some of those data. We conducted a major randomized controlled trial in 2000. We were asking the question of whether surgery is better than medicine. It had never been asked, but we could ask that question with the band, whereas we could not logistically do it back then with a bypass.
Eighty patients were randomized to a medical program or the band with a 2 year follow-up, and we followed their health and their weight. The paper that we published in Annals of Internal Medicine in 2006 showed the percent of excess weight loss was 87% in the surgical group and 21% in the control group 14 (Fig. 6).

Medical treatment versus LAGB surgery. EWL, excess weight loss; RCT, randomized controlled trial. Courtesy of O'Brien et al., Ann Int Med, 2006. Color images available online at www.liebertpub.com/bari
These figures are from the early part of this decade. We now have 10 year follow-up on those patients. We have just completed that, and in fact we have published it in the current edition of Obesity Surgery. 15
You can see in Figure 7 that from the peak of 80% excess weight loss, it's fallen away somewhat, possibly reflecting the fact that all of these patients entered into our normal follow-up program once the trial was complete, which might not have been as intense. But they still maintained 62% of their excess weight loss after 11 years.

Medical treatment versus LAGB surgery, long-term outcomes. C.I., confidence interval; EWL, excess weight loss. Courtesy of O'Brien et al., Obesity Surgery, Sept, 2013.
Earlier this year in the Annals of Surgery, we published the outcome on 3,200 patients we had treated throughout the whole period that the band was available. 16 A total of more than 8,000 patients have been followed up in our dedicated band clinic and Wendy Brownb and I have taken care of this particular group of 3,200 patients. There have been no deaths associated with any primary procedure or revisional procedure. And some of these patients are very sick people.
There is no question that the band is a safe procedure, and any of us who have used it know this to be so. Figure 8 shows the weight loss that occurred in those patients over the 15 years.

Weight loss up to 15 years after LAGB surgery. Courtesy of Dr. O'Brien.
Patients reach a peak of just over 50% of excess weight loss in about 2 to 3 years post-surgery, and from then on it is relatively stable. They end up averaging 47% of excess weight loss.
For long-term outcomes, we did a systematic review of the literature. 16 We found seven papers addressing band outcomes that had 10 or more years of follow-up, with at least 10 patients at the time of follow-up, and had presented the data in terms of percent of excess weight loss. At the same time, we found eight similar papers addressing the Roux-en-Y gastric bypass. We have had Roux-en-Y for 45 years now, and there are only eight papers with long-term follow-up. This was up until November 2011 when we stopped the literature review. The weight loss from the two sets of papers comes out about equal: 54% of excess weight loss in the band group and 54% in the bypass group!
However, Roux-en-Y also had a reoperation rate between 8% and 38%. It is clear that the reoperation rate of the Roux-en-Y patients is not much different from the reoperation rate of the band patients.
There are many high-quality randomized trials demonstrating that weight loss after the band is associated with better health, longer life, physical improvements, better psychosocial circumstances, and money savings.
There have now been four high-quality studies done for diabetes and bariatric surgery: our study in Melbourne, 17 Phil Schauer's study in Cleveland, 18 the Rome study, 19 and a recent wonderful study by Sayeed Ikramuddin. 20
There were differences between the studies, which could matter, but our endpoints are very clear. Surgery is an effective means of treating diabetes. In Phil Schauer's study, there was 44% diabetes remission rate for bypass patients and 37% remission for sleeve patients, which is three times the control group's remission rate. That's a very good result. There was a 73% diabetes remission rate in our band study, 75% diabetes remission for bypass in the Rome study, and 95% diabetes remission for BPD. Ikramuddin's study showed 44% diabetes remission rate, which was exactly the same as the Schauer study.
So the band does work. But why is it that people are moving away from the band? We know it works if it's done correctly. Is it because it requires too much aftercare? Aftercare is not funded and that's important.
The band is very safe. It's truly an outpatient surgery. It's minimally invasive, with no anatomic changes and requires simple analgesics for postoperative pain. In our clinic in Melbourne or our clinic in Texas, you can do it for <$10,000.
The long-term studies that Dr. O'Brien quotes on LAGB included colleagues, Dr. Miller and Dr. Himpens. Are they currently doing Lap-Band procedures? Dr. Himpens is going to tell us that he's not putting in a single band, and Dr. Miller has already shown us the dramatic decrease in band placements.
The problem with the studies that Dr. O'Brien quotes on gastric bypass and DS in his 10 year study is that the average BMI of those patients is not 40. It's in the 50s. The percentage of excess weight loss at a BMI of 50 is at least 10% lower than when you have a LAGB for a BMI of 40.
And there is a conflict of interest. Most of their center is sponsored and paid for by Allergan, so that gets into the equation. In June 2003, Allergan shares plunged, and recently their shares went down once again. The Lap-Band entity of Allergan has now been spun off into its own company again. Why is that?
The conclusion of their study was that gastric banding is safe and effective, and it supports the existing data that it's safer than Roux-en-Y gastric bypass. However, there is no data that specifically address the differences in long-term weight loss outcomes and need for revision between the two procedures. In fact, there is an editorial from the New England Journal of Medicine that underscores the passionate debate over the preferred procedure that is not based on actual data. 21 Some strongly prefer LAGB over gastric bypass because of the former's safety advantage and the belief that long-term outcomes of the two procedures are similar. Others argue for gastric bypass because they believe long-term outcomes fall short in patients who undergo LAGB and that there is an unacceptably high need for removal of the band or a conversion to a bypass procedure or sleeve gastrectomy.
There is no long-term randomized study between the banding procedure and the other procedures, and that's what we need. In this case, we need to compare oranges to apples.
One good comparison is to think about osteoarthritis of the knee and total knee replacement. Osteoarthritis is a chronic disease for which there is a surgical cure. Total knee replacement started about the same time as bariatric surgery started to grow. For the United States in 2013, there was about 650,000 total knees replaced.c The slope of growth is steep, and it's projected to go to 3.5 million total knees by the year 2030. Who is making those decisions? Who is making the decision that prevents access to bariatric surgery?
We have had gastric stapling now since the 1960s. I believe there are a huge number of people who are just not opting to undergo stapling procedures. Those are the people who are going to make the decision at the end of the day. It's not going to be Michel Gagner or Jacques Himpens or me. They're going to come to us, and they're going to ask us for help.
Are they going to ask for a stapling procedure? I don't think so. I think they've made that decision. I'm happy to acknowledge that all of these procedures work. All I'm saying is that the band, if it's used correctly, can work just as well as anything else.
But to appeal to the physicians, to appeal to the healthcare administrators, and to appeal to the people who have the problem of obesity, we're going to have to change the tone of how we're approaching it. There should not be fighting over this little sliver, but rather striving to meet the needs of our patients.
To address the point about Allergan: I have never received funding from Allergan. My research center, from which I have retired as director, certainly has had funding. Allergan is now in the process of selling the band company, and the band is such a trivial item within a very big company that it would hardly even show up on their balance sheet. So whatever happened to the stock market is totally unrelated, but I appreciate Michel bringing it up.
So think about the future. I think we're going to see things turn around. The safety of the band, the softness of it, the gentleness, and the fact that it is really an outpatient procedure. You can't go and have a colonoscopy as simply as you could with a band these days. And we can get good results if we know how to do it correctly.
I know how to do it correctly. I can do it in Melbourne. I can do it in Texas where I cover a group there. We can achieve good results, and our group in Texas is growing. Our group in Melbourne this year has seen 92% more patients than we saw for the same period last year. So if you do it properly, you're on a winner. It's a good procedure.
Footnotes
Disclosure Statements
Dr. Gagner has received honorarium for educational activities from Covidien, Ethicon, W.L. Gore, MID, Transenterix, and Boehringer Laboratories.
Dr. Paul O'Brien is the Emeritus Director of the Centre for Obesity Research and Education (CORE) at Monash University which receives a grant from Allergan for research support. The grant is not tied to any specified research projects and Allergan has no control of the protocol, analysis and reporting of any studies. CORE also receives a grant from Applied Medical towards educational programs.
Dr. O'Brien has written a patient information book entitled “The Lap-Band Solution: A Partnership for Weight Loss” which is given to patients without charge, but some are sold to surgeons and others for which he receives royalty.
Dr. O'Brien is also employed as the National Medical Director for the American Institute of Gastric Banding, a multicenter facility, based in Dallas, Texas, that treats obesity predominantly by gastric banding.
Dr. Ponce is a consultant for Apollo Endosurgery, speaker and consultant for W.L. Gore, consultant and clinical trial investigator for Reshape Medical, and clinical trial investigator for USGI Medical. Dr. Ponce is also a former adjustable gastric band proctor for Allergan and Ethicon.