
Abstract
Agranulocytosis is a serious, potentially life-threatening disorder that frequently occurs as an adverse reaction to drugs. Carbamazepine is a known culprit and a very common drug used as an anti-epileptic. The case is reported of a 49-year-old epileptic woman on long-term carbamazepine treatment who developed agranulocytosis following bariatric surgery (sleeve gastrectomy), likely due to carbamazepine-altered oral exposure resulting in high plasma levels. A reduction in the drug dose resulted in normalization of carbamazepine levels and improvement of the neutrophil count without the use of granulocyte colony-stimulating factor (GCSF). This observation could explain a dose-dependent drug-induced cytopenia rather than an idiosyncratic effect. This is the first case of drug-induced agranulocytosis following bariatric surgery, which illustrates the need for careful postoperative monitoring of specific drugs. A literature search of the use of GCSF in agranulocytosis and the status of drug absorption following bariatric surgery was also performed.
Case History
A 49-
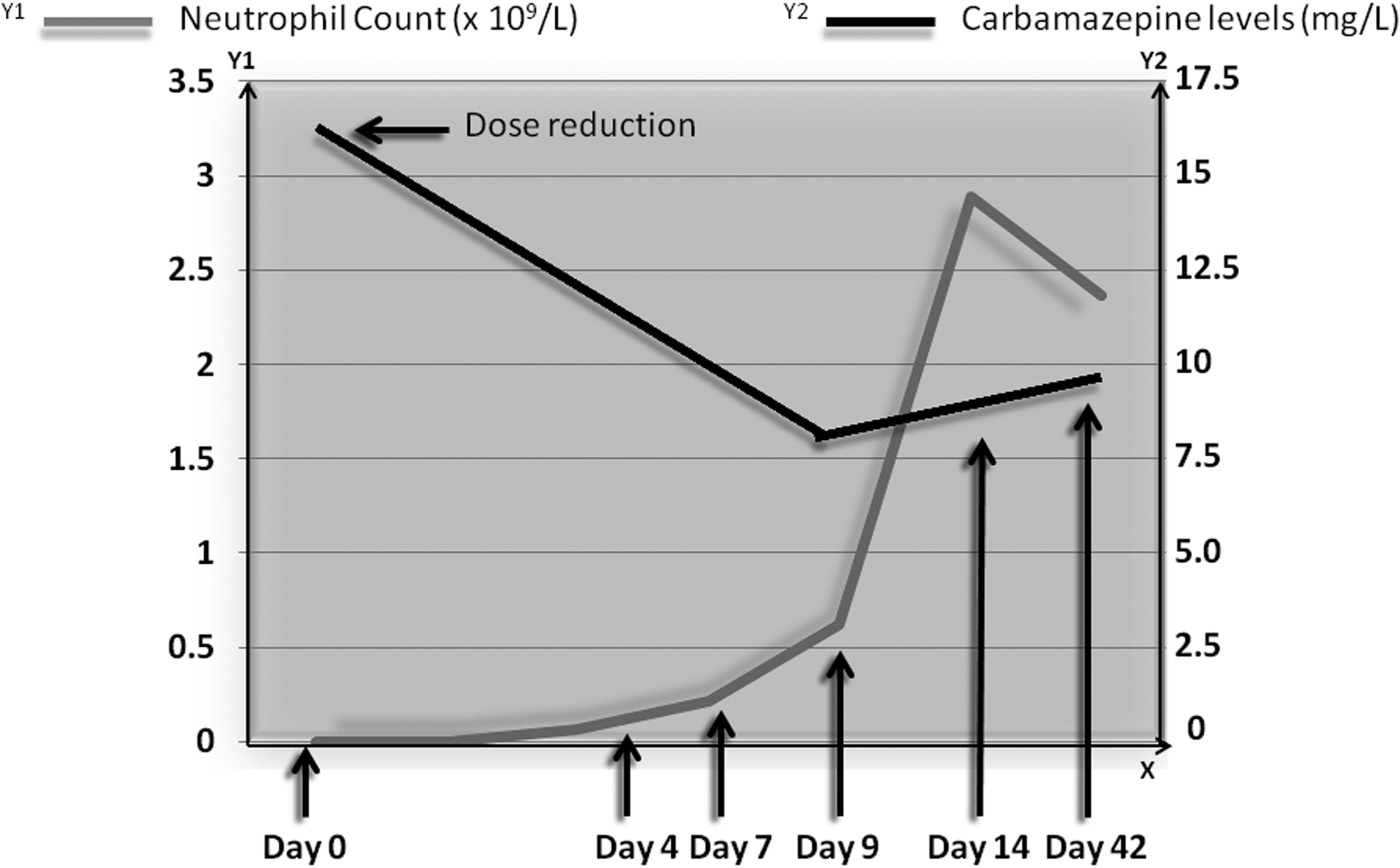
High levels of carbamazepine (15.9 mg/L) were recorded on admission (day 0). Dose was gradually reduced from 800 mg BD to 400 mg BD. Levels normalized, and on day 9, neutrophil count had been over the safe level of 0.5 × 109/L.
Definition
Agranulocytosis is marked by a profound decrease in the number of, or an absolute lack of, granulocytes in circulating blood, classically resulting in a neutrophil count <0.5 × 109/L.1,2 In the majority of patients, the neutrophil count is <0.1 × 109/L. Under Council for International Organizations of Medical Sciences auspices, the Roussel Uclaf pharmaceutical company organized an international meeting in 1991 concerning drug-induced blood cytopenias, and set the criteria for idiosyncratic drug-induced agranulocytosis (Table 1).3,4
Discussion
Agranulocytosis associated with the use of carbamazepine is well-known. The collective incidence of thrombocytopenia, agranulocytosis, and aplastic anemia ranges from 1% to 2%. 5 A decrease in white blood cells (WBC) is thought to occur with carbamazepine due to the inhibition of colony-stimulating factor in the bone marrow. The co-administration of lithium, which stimulates colony-stimulating factor, can sometimes reverse the effects of carbamazepine. 5 Leukopenia occurs transiently in about 10% and persistently in about 2% of carbamazepine-treated patients, and typically develops within the first 3 months of treatment. 6 Interestingly, women are at a higher risk developing leukopenia than men when exposed to anticonvulsants, with no clear explanation for this finding. Usually recovery of the WBC count occurs within about 6 days following discontinuation of carbamazepine. 7 Although mild or moderate neutropenia is a more common side effect of carbamazepine therapy, agranulocytosis is a very rare event, with only a few cases described in the literature. Most of these cases report an idiosyncratic phenomenon, in that toxicity can occur after different periods of exposure, is unpredictable, and not clearly related to the total dose consumed.8–10 However, the present case demonstrates that agranulocytosis developed only when carbamazepine plasma levels were high and was resolved with reduction of the dose, without needing to stop the drug.
Common drugs most often associated with agranulocytosis are listed in Table 2. Drugs commonly used in clinical practice for which the risk appears to be higher are highlighted.
Higher risk.
The main concerns in such cases are severe sepsis and deep-seated infections that without appropriate treatment could be fatal. More than 20 years ago, the mortality rate for idiosyncratic drug-induced agranulocytosis was 10–16%, as reported in European studies.1,11,12 This rate has dropped to 5–10% in the last decade, and keeps improving with the early recognition, management, and prompt use of broad-spectrum antibiotics. 1 The incidence of agranulocytosis increases with age, as only 10% of cases are reported in children and young adults, and more than half of the cases occur in people older than 60 years of age. 13 Old age (>65 years), septicemia or shock, metabolic disorders such as renal failure, and a neutrophil count <0.1 × 109/L are poor prognostic factors, and are associated with a longer time to neutrophil recovery. 4 However, in all cases of neutropenia, other causes should be excluded, especially if there is no improvement after discontinuation of the relevant drug (Table 3). Local guidelines suggest the following baseline investigations for neutropenia before a bone-marrow biopsy: B12/folate; autoimmune screen; virology, including hepatitis B and C, human immunodeficiency virus, occasionally Epstein–Barr virus, and cytomegolvirus; and a blood film.
Drug absorption and bariatric surgery
Bariatric surgery has been used increasingly to tackle obesity, especially for patients with other comorbidities such as type 2 diabetes and hypertension. Current strategies aim to alter the anatomy of the gastrointestinal tract and produce weight reduction. Two mechanisms are responsible: limiting the volume of food intake while diminishing the stomach's capacity, or inducing malabsorption by surgically bypassing regions of the small intestine and diverting biliopancreatic secretions, which limit nutrient absorption. 14 Commonly used procedures are gastric banding, sleeve gastrectomy, Roux-en-Y gastric bypass (RYGB), and biliopancreatic diversion with duodenal switch (BPD-DS). As a consequence, the absorption of nutrients and vitamins is affected. The British Obesity and Metabolic Surgery Society recommends annual monitoring and supplementation of B12, folate, calcium, and vitamin D (Table 4). 15
May be variation between centers as to whether routine supplementation with vitamin B12 following the sleeve gastrectomy or duodenal switch.
The alteration in the anatomy and physiology of the gastrointestinal tract could potentially affect drug absorption. Unfortunately, there are only a few studies or case reports in this field. Padwal et al. conducted a systematic review of 26 studies. Evidence for diminished drug absorption was found in 15/22 studies involving jejunoileal bypass, 1/3 studies of gastric bypass/gastroplasty, and 0/1 studies examining biliopancreatic diversion. The effect of bariatric surgery on drug absorption appears to be drug specific. The most consistent evidence for diminished absorption was found for cyclosporine, thyroxine, phenytoin, and rifampin. 16
However, there is some evidence for unchanged or enhanced drug absorption after gastric bypass surgery. Studies have shown that interindividual variability of enzymatic expression and, consequently, differences in first-pass metabolism have a potential effect in drug bioavailability. 14 Skottheim et al. evaluated the effect of bariatric surgery (RYGB and BPD-DS) on the bioavailability of atorvastatin. Pharmacokinetic measurements were obtained, as well as genotypic profiling for cytochrome P450 3A5 (CYP3A5) and ATP-binding cassette subfamily B member 1 (ABCB1). Those patients with the lowest systemic exposure (high enzymatic expression) prior to surgery showed a median 1.2-fold increase in area under the curve (AUC) of the drug and a twofold increase after BPD-DS. 17 Since CYP enzymatic content is greater in the proximal portions of the small intestine, bypass of this segment should cause an important reduction in intestinal metabolic activity. Therefore, this may increase the bioavailability of certain drugs, as in this case of atorvastatin. However, the same group, in a follow-up of these patients, demonstrated that the initial increase in atorvastatin systemic exposure observed in the majority of patients 3–8 weeks after surgery. This effect was reversed approximately 2 years after surgery. 18 Other studies show diversity of long-term findings on systemic exposure of different drug categories.19–21 With the lack of clinical trials for other potentially toxic drugs, it would seem reasonable serum concentrations to be measured separately for each patient postoperatively.
With sleeve gastrectomy, drugs will not bypass any part of the small intestine and therefore do not alter intestinal first-pass metabolism. The smaller volume of the stomach with restrictive procedures may prevent adequate tablet or capsule disintegration due to reduced gastric mixing. 16 22 Solubility of a drug is dependent on pH. Drugs that are more soluble at a lower pH are absorbed in the stomach, while those that are soluble in more basic environments are absorbed in the small intestine. Changes in the stomach volume after bariatric surgery result in a decrease in gastric acid production and a higher pH compared with the stomach as a whole. The change in pH may cause a decrease in the absorption of medications that rely on an acidic pH for solubility or absorption. A reduction in the surface area of the stomach may further decrease drug bioavailability. These changes may be especially important for drugs that are slowly absorbed, such as sustained-release formulations.
However, in the present case, it is important to consider the effect of obesity on pharmacokinetics independent of the bypass procedure because it leads to a dramatic drop in body mass over a relatively short period of time. This may be associated with reversals in the influence of obesity on drug disposition to characteristics more in line with leaner patients. Drugs will differ in their pharmacokinetic response to surgery, limiting any general conclusions regarding the impact of the surgery on drug disposition. 23 Other potential mechanisms in sleeve gastrectomy and augmented oral drug exposure could include a possible acute change in CYP3A due to interleukin-6 (IL-6) induction and altered drug metabolism 24 or induced hepatic metabolic activity due to weight loss.
Role of granulocyte colony-stimulating factor in agranulocytosis
Granulocyte colony-stimulating factor (GCSF) is a glycoprotein that stimulates proliferation and differentiation of myeloid progenitor cells of the granulocyte lineage with minimal in vitro or in vivo effect on other lineage, and enhances mature neutrophil function by improving chemotaxis and increasing phagocytosis and oxidative burst.25,26 Currently, GCSF is not yet licensed for use in this specific condition, and sometimes it is still debatable whether it improves outcomes. Andrès et al. conducted an analysis of seven other systematic reviews and case studies between 1994 and 2008 on hematopoetic growth factors and drug-induced agranulocytosis. 27 In some of these studies, the evidence put forward was questionable, but overall, six out of seven studies appear to support the use of GCSF. The benefits included reduction in the duration of agranulocytosis (2–5 days), and reduced antibiotic use and length of hospital stay with minimal or absent side effects. The authors concluded that their preference would be to use GCSF, especially in the group of patients with poor prognostic factors as described above (neutrophil count <0.1 × 109/L, age >65 years, severe infection, or comorbidity).
Conclusion
As many of the guidelines for bariatric surgery focus on postoperative biochemical monitoring and micronutrient replacement, there is no clear guidance for specific drug monitoring. The present case demonstrates that bariatric surgery (sleeve gastrectomy) could potentially enhance oral drug exposure of carbamazepine with the relevant complications. The rare side effect of agranulocytosis seemed to develop in a dose-dependent manner. In cases of agranulocytosis, early management of infections with broad-spectrum antibiotics, consideration of GCSF use, and consultation with a hematologist is necessary. Considering the potential impact of sleeve gastrectomy on oral drug exposure and long-term adaptation, it would be reasonable to monitor therapeutic drug levels, when possible, with complete blood count, kidney, and liver function until anastomoses are healed and the risk of immediate complications is minimal. Once or twice weekly blood samples for the first 2 months and monthly thereafter for the following 3 months are recommended. Long-term monitoring, every 3–6 months, might be necessary until a more stable weight is obtained or at any time point when drug toxicity is apparent. Therefore, it is imperative to identify certain drug categories where the risk of bone-marrow suppression is higher, and more studies are needed in order to set guidelines for post bariatric surgery drug monitoring.
Footnotes
Acknowledgments
We wish to thank Gráinne Smyth (Clinical Pharmacist), who helped with the case.
Author Disclosure Statement
No competing financial interests exist.