
Abstract
Obstructive sleep apnea (OSA) is a common comorbidity in the patient population undergoing bariatric surgery. Up to 70% of patients undergoing weight loss surgery suffer from the disease and its physiologic sequelae. Subjecting these patients to surgery, an anesthetic, opioid therapy, and other sedating medications may place them at increased risk for an adverse event in the perioperative period. There is extensive medical literature outlining post-surgical complications in patients with OSA and growing evidence that both preoperative and postoperative considerations should be made in caring for these patients. There is an increasing number of perioperative care recommendations from national societies and patient safety organizations outlining management strategies for OSA patients. However, there is not yet a faultless predictive model determining which patients with OSA are at highest risk after surgery. This article serves specifically to address OSA in the bariatric population, apply sleep apnea literature in real practice, and demonstrate a large hospital-system algorithm used to assess, risk-stratify, and care for this population.
Introduction
A
OSA has been estimated to affect 5–9% of women and 17–24% of men aged 30–60 years in the United States. 10 It has been estimated that up to 90% of individuals with moderate to severe OSA have not been formally diagnosed.11,12 Surgical patients may have a higher incidence of OSA than the general population; the disease has been estimated to affect one in four surgical patients 13 and is higher in certain subsets of patients, including those undergoing bariatric surgery. Lopez et al. preoperatively evaluated patients presenting for bariatric surgery with a formal sleep study, and found that 78% of study subjects were diagnosed with at least mild OSA. 13 Additionally, patients with OSA may have numerous comorbidities such as diabetes, hypertension, stroke, heart failure, and atrial fibrillation, increasing patient complexity for physicians managing these patients in the perioperative period. With approximately 163,000 patients undergoing weight loss surgery in the United States in 2013, 14 surgeons and anesthesiologists need to create focused plans to manage and care for patients with sleep apnea.
OSA patients have been shown to have a significantly increased risk of postoperative complications.15–17 Mokhlesi et al. retrospectively analyzed a database of 91,028 patients undergoing bariatric surgery from 2004 to 2008 to determine if OSA (determined by ICD-9 code) was an independent predictor for mortality, increased length of stay (LOS), and cardiac or respiratory complications. 18 In this study, diagnosed OSA was not associated with an increase in mortality or LOS. It was however, associated with a significantly increased odds ratio for emergent postoperative endotracheal intubation and mechanical ventilation (OR 4.35 [95% confidence interval (CI) 3.97–4.77], p < 0.001) and atrial fibrillation (OR 1.25 [95% CI 1.11–1.41], p < 0.001). A more recent study of bariatric patients compared 693 bariatric patients undergoing Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy. 19 The patients were divided into three groups: (1) patients with OSA using positive airway pressure (PAP) therapy; (2) patients who screened as high risk for OSA (STOP-Bang score >3) or had diagnosed OSA but were not on PAP therapy; and (3) patients who had a STOP-Bang screening score ≤2, and were considered as low risk for OSA. Analysis of the results revealed that group 2 had a longer LOS (4.1 vs. 3.2 vs. 2.5 days, p = 0.0001 and p < 0.0001), increased incidence of pneumonia (2 vs. 17 vs. 4, p = 0.040 and p < 0.0001), and more reintubations (0 vs. 7 vs. 0, p = 0.1442 and p = 0.0098). There were two deaths in the study, both in group 2 (0 vs. 2 vs. 0, p = 0.5142 and p = 0.3807). An autopsy was performed for both patients and revealed cause of death was sudden cardiac arrest due to asphyxia.
Preoperative Screening
Given the increased risk of adverse cardiac and pulmonary events in patients with OSA undergoing surgery, implementing a screening system for sleep apnea should be a part of the preoperative evaluation. This is particularly true for patients undergoing bariatric surgery, given the increased incidence of disease. Both the American Society of Anesthesiology and the Joint Commission recommend screening all surgical patients for OSA. In 2012, the Society for Ambulatory Anesthesia (SAMBA) published a consensus statement recommending the use of the STOP-Bang screening questionnaire (Fig. 1) as the preoperative screening tool. 20 Although there are numerous screening tools available, the STOP-Bang is easy to administer, has been validated in all surgical populations, and is highly sensitive. It is not, however, diagnostic for sleep apnea, and should ideally be administered during an initial surgical consult to allow time for a sleep study referral for those who screen as high risk.

STOP-Bang Questionnaire. Adapted from the STOP Questionnaire, A Tool to Screen Patients for Obstructive Sleep Apnea, Frances Chung, Balaji Yegneswaran, Pu Liao, Sharon A. Chung, Santhira Vairavanathan, Sazzadul Islam, Ali Khajehdehi, Colin M. Shapiro. Anesthesiology 2008;108:812–821.
The STOP Questionnaire was developed by Dr. Francis Chung et al. at the University of Toronto and was published in the medical literature in 2008. A score of three out of four “yes” answers to the screening questions predicted, with high sensitivity, those with moderate and severe sleep apnea. Including the Bang parameters further improved the sensitivity of the screening tool. Using a score of three, the STOP-Bang is >90% sensitive for patients with moderate to severe sleep apnea. 21 The specificity was, however, much lower: 56%, 43%, and 37% for mild, moderate, and severe sleep apnea, respectively. Given the cost of sending a large number of patients for sleep study when many of them may not have the disease, the screening has been reevaluated to determine if a higher screening score may be more reasonable. Increased scores are more likely associated with the presence of OSA. 22 An evaluation of 746 patients who visited preoperative clinics for a variety of inpatient surgeries were screened by STOP-Bang score and underwent polysomnography (PSG) with complete data available for review. For STOP-Bang scores of 5 or 6, OSA was confirmed to be present in 68% of patients. For a score of 5, the odds ratio of moderate and severe OSA was 4.8 and 10.4, respectively. In a study specifically looking at obese (BMI ≥ 30 kg/m2) and morbidly obese (BMI ≥ 35 kg/m2) patients, 310 presurgical candidates were screened by STOP-Bang score and underwent PSG. Of those, 253 (81.6%) were diagnosed with OSA (apnea–hypopnea index [AHI] >5). 23 In this patient population, a STOP-Bang score of 4 had a sensitivity of 87% and specificity of 41%, whereas a score of 5 demonstrated a balance between sensitivity and specificity with scores of 68 and 69%, respectively.
The STOP-Bang screening model is highly sensitive at lower screening scores but lacks specificity at these same cutoff points. Given the sacrifice made for sensitivity, consideration can be given to combine the STOP-Bang score with a review of the patient's serum bicarbonate level (HCO3−). In a study of 384 elective surgery patients, a STOP-Bang screening score was obtained, a preoperative PSG was completed, and a serum HCO3− level was measured prior to surgery. 24 The authors chose to use a cutoff point of HCO3− ≥ 28 mmol/L because it represented the 75th percentile of the cohort. For those with an AHI of 16–30 (moderate OSA), the serum HCO3− was ≥28 mmol/L in 39.5% of the sample. Forty-three percent of patients with severe sleep apnea (AHI > 30) had a serum HCO3− level of ≥28 mmol/L. Patients with a STOP-Bang score ≥3 and a HCO3− ≥ 28 mmol/L had a twofold increase in the probability of having OSA; this was equivalent to using a STOP-Bang ≥6. The specificity based on STOP-Bang ≥3 alone is 37% for OSA. It is slightly lower at 30.4% for moderate/severe OSA and 27.7% for severe OSA. Using serum HCO3− ≥ 28 mmol/L, in addition to a STOP-Bang ≥3, improved specificity of the screening to 85.2%, 81.7%, and 79.7%, respectively.
Making a decision with regard to a screening cutoff that prompts preoperative testing can be difficult and may be one of the limitations preventing hospitals from routinely using a questionnaire to evaluate patients. The data have not yet defined an optimal number to send patients for sleep study to prevent adverse events in the perioperative period. Given that information, and in consideration of limited resources and a patient's ability to obtain a sleep study prior to surgery, the authors' hospital system chose to use a cutoff point of 5 to balance sensitivity and specificity. Patients with a score ≥5, with sufficient time prior to surgery, are referred for a sleep study for both diagnosis and implementation of PAP therapy if needed. If a program were to screen only bariatric patients, it would be reasonable to use a lower number (4) to refer for PSG or home sleep apnea test (HSAT) given the prevalence of OSA in this population. The preoperative serum HCO3− level is currently used to risk stratify patients postoperatively, but, as studied, it could additionally be used preoperatively in combination with STOP-Bang ≥3 to determine patients who could benefit from a sleep test referral.
The value of screening, even if the patient is unable to obtain a sleep study or initiate PAP therapy, is an important first step for all hospitals taking care of patients with both untreated and undiagnosed sleep apnea. Anesthetics, sedatives, and narcotics worsen upper airway collapsibility, affect sleep architecture and REM patterns, and diminish the arousal response to hypercarbia and hypoxia. A risk score can aid in planning an anesthetic, choosing preoperative and postoperative medication, and determining the level of monitoring required for patients postoperatively.
Preoperative Testing and Initiation of Therapy
There is an absence of large randomized, controlled, prospective trials that demonstrate that preoperative testing and initiation of PAP therapy improves patient outcomes. Sending all patients for sleep testing may be prohibitive from a cost and resource standpoint; testing and titration of treatment may also delay the patient's surgical date. Stierer and Collop 25 wisely point out that the “phenotype of the patient who will suffer adverse perioperative outcomes due to OSA has not been elucidated.” Hospital systems, surgeons, and anesthesiologists should realize that an exact model for determining who best benefits from preoperative screening and testing has yet to be determined. If the need for surgery limits time available for testing, there is not clear evidence to suggest that diagnosis by sleep study improves outcomes over treating suspected OSA patients as having the disease.
The benefits of PAP therapy for treatment of OSA have been demonstrated in the medical literature; definitive physiologic changes occur in patients treated with continuous positive airway pressure (CPAP). Those same changes are thought to be beneficial in both the operating room and postoperative period. CPAP therapy in patients with OSA has been shown to improve systolic function in those with congestive heart failure (CHF), 26 to decrease blood pressure in drug-resistant hypertension, 27 and to reduce arterial stiffness 28 (an indicator of cardiovascular risk). Untreated OSA doubles the 12 month risk of recurrent atrial fibrillation compared with those with OSA using CPAP therapy. 29
Thus, patients at high risk for OSA (STOP-Bang ≥5 OR STOP-Bang ≥3 + HCO3− ≥ 28 mmoL/L) with poorly controlled medical comorbidities merit testing and treatment if time before surgery allows. Conditions that present concern in a patient with known (but untreated) OSA or suspected OSA, particularly in the surgical environment, include untreated or drug-resistant hypertension, uncontrolled atrial fibrillation, CHF with an ejection fraction ≤40%, pulmonary hypertension, and COPD on home oxygen therapy.
CPAP therapy has not been yet proven to be a panacea for OSA in the perioperative setting. However, there are data to suggest that preoperative CPAP may benefit patients in the postoperative period. Liao et al. recently demonstrated in a randomized trial that autotitrated continuous airway pressure (APAP) started 2 days prior to surgery and continued 5 days postoperatively, decreased the AHI and improved oxygenation in orthopedic patients with OSA. 30 Mutter et al. compared postoperative outcomes in undiagnosed OSA patients with outcomes when the same patients were subsequently diagnosed with OSA and provided CPAP treatment with a matched cohort control. 31 The risk of respiratory complications in both undiagnosed and diagnosed OSA patients compared with controls was significantly higher for developing adult respiratory distress syndrome (p < 0.001) and respiratory failure (p < 0.04). The undiagnosed OSA patients not receiving treatment also had an OR of 2.40 [CI 1.22–4.72] for experiencing cardiac arrest and shock (p = 0.01) compared with controls. In contrast, when diagnosed and treated with CPAP, they did not have an increased risk for cardiac arrest (OR 0.82 [CI 0.38–1.78], p = 0.61), demonstrating that preoperative CPAP decreased the risk of cardiac morbidity in OSA patients.
More recently, however, a systematic review and meta-analysis of >900 patients with known or suspected OSA using CPAP (pre- and/or postoperatively) versus those not using CPAP revealed no difference in postoperative adverse events. 32 Patients with pre- or postoperative CPAP use compared with no CPAP had risk ratio of an adverse event of 0.88 [CI 0.73–1.06]. Decreased LOS trended toward the CPAP group versus no-CPAP group but was not statistically significant (p = 0.05). Thus, although CPAP use for OSA may decrease LOS, the efficacy of CPAP in preventing perioperative morbidity was not clearly established in this study.
Ambulatory Center versus Inpatient Hospital Setting?
More complete analyses of this topic are available in the literature. However, a brief review is provided here to assist programs in developing an algorithm for scheduling surgery in the most appropriate care environment. The authors' hospital has developed a straightforward algorithm to designate patients that do and do not qualify for care at an ambulatory center.
In 2012, SAMBA published a consensus statement “Preoperative Selection of Adult Patients with Obstructive Sleep Apnea Scheduled for Ambulatory Surgery.” In determining their position statement, SAMBA members performed a meta-analysis of seven articles evaluating patients undergoing surgery at an ambulatory center, including those having laparoscopic bariatric surgery. The incidence of postoperative hypoxemia and need for supplemental oxygen in this review was higher in the OSA population. However, this did not correlate with reintubation, longer time to discharge, hospital admissions, or death. Based on these results, SAMBA published guidelines that were not aligned with the 2006 American Society of Anesthesiologists (ASA) recommendations on OSA. The SAMBA algorithm for determining appropriateness for ambulatory surgery does not exclude patients with known or suspected OSA, but instead suggests that these patients must be medically optimized and willing and able to use postoperative CPAP. SAMBA additionally recommends that pain management in this setting be predominantly provided with nonopioid medications.
The authors' hospital algorithm determining which patients undergoing general anesthesia qualify for same-day versus inpatient surgery is based on the SAMBA guidelines but with defined criteria for medical conditions that preclude ambulatory surgery (Fig. 2). Due to the hypoxemia and hypercarbia that can occur in OSA, patients with concomitant CHF, atrial fibrillation, severe COPD, and pulmonary hypertension may be at higher risk in the postoperative setting. Additionally, due to the risk of respiratory failure in patients with neuromuscular disease and the likeliness that patients on chronic opioid therapy will need higher doses of opioids in the perioperative setting, there is also risk for these patients if sent home following their surgery. It is recommended that these patients have surgery at an inpatient facility with consideration for a monitored bed as needed. Of note, it is important to recognize that patients who have undergone a uvulopalatopharyngoplasty and no longer use CPAP should be treated as having OSA unless a repeat sleep study demonstrates resolution of disease; they should follow selection criteria to determine if they are an appropriate candidate for an ambulatory surgery center.
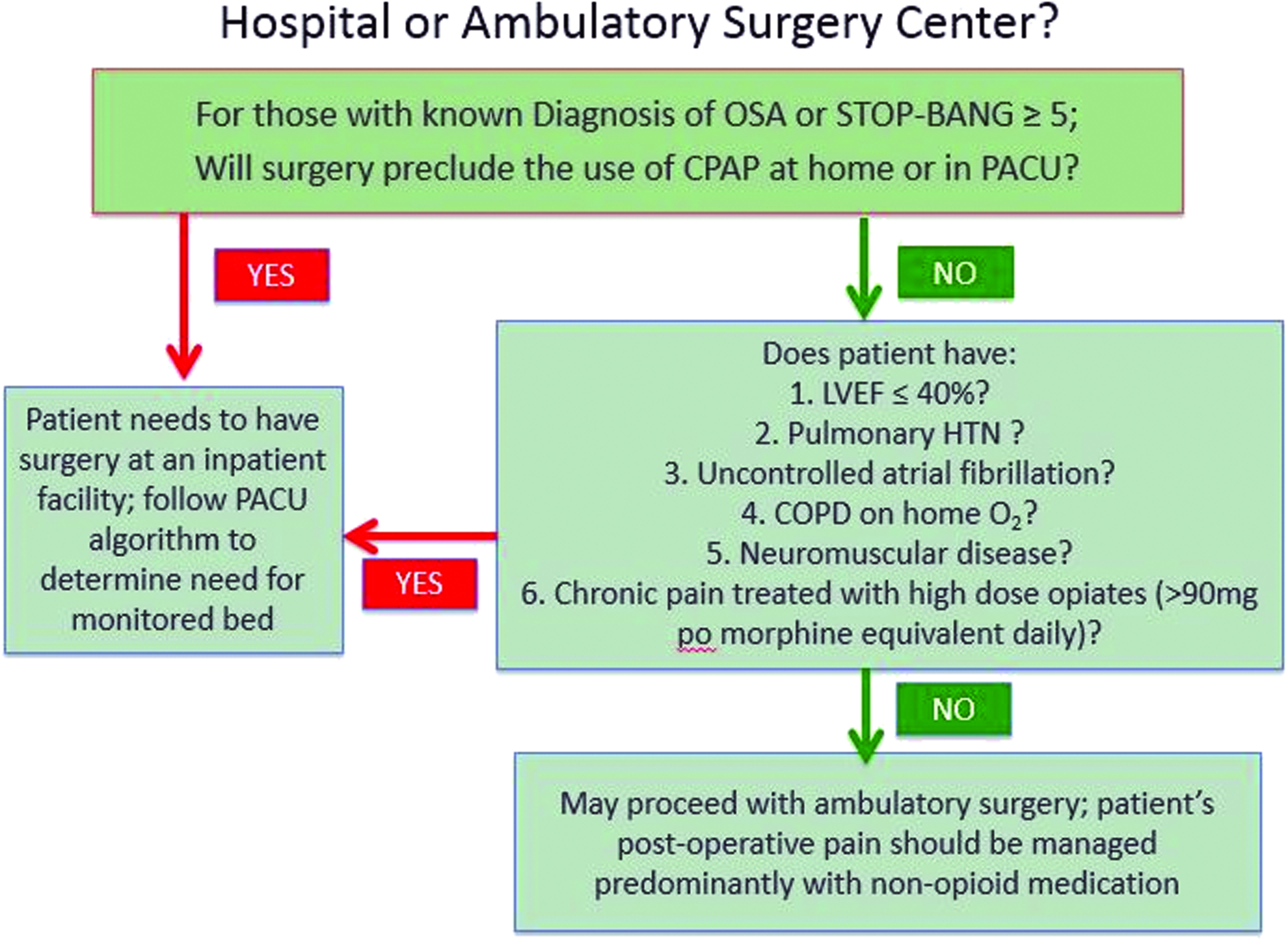
Inpatient versus ambulatory surgery setting. Color images available online at www.liebertpub.com/bari
Ambulatory surgery centers caring for patients with known and suspected OSA need to be familiar with CPAP devices and settings to be able to assist patients with set-up. Furthermore, patients with undiagnosed but suspected OSA may require CPAP postoperatively to provide the necessary airway pressures to prevent obstruction resulting in hypopnea, hypercarbia, and hypoxia. If the ambulatory surgical center does not have access to a PAP device or the trained staff to place the machine and choose appropriate settings, consideration needs to be given to scheduling surgery at a facility with necessary resources.
All patients, regardless of surgical facility, should be screened in the post-anesthesia care unit (PACU) to determine the most appropriate level of monitoring following PACU care. Although most patients do well in an ambulatory surgery environment and may proceed home, there are times that a hospital admission will need to be facilitated in this environment due to high-risk behaviors demonstrated in the PACU. Thus, qualifying to have surgery in an ambulatory environment does not guarantee that a patient will be able to be discharged to home.
Postoperative Screening
Preoperative screening for OSA and suspected OSA is only valuable if the information impacts patient care decisions. Obtaining a STOP-Bang score for patients prior to surgery is an important first step, but screening alone does not provide sufficient care for these patients.
Patients with a known diagnosis of OSA who are on CPAP therapy should have their CPAP device placed very shortly after arrival in the PACU. The sedating effects of an anesthetic, opioids, benzodiazepines, and antihistamines place the airway at increased risk of obstruction due to the decreased activity of the upper airway musculature and a blunted arousal response.
Those patients with known OSA, who are not currently on CPAP, or those with a STOP-Bang score ≥5, should be carefully observed in the PACU for behaviors that indicate respiratory compromise. The use of continuous pulse oximetry is an American Society of PeriAnesthesia Nursing (ASPAN) standard for PACU care, and should be used in all patients with known or suspected sleep apnea. However, it should not be the only means to evaluate the adequacy of ventilation. Even in the setting of normal oxygenation, ventilation may be substantially impaired, and hypoxemia may be a late event. To date, there is not an accepted standard monitor in all postoperative care environments that will assess ventilation. If capnometry is available, using this technology provides additional information when assessing the quality of ventilation. The absence of an end-tidal CO2 tracing, >5 second pauses between breaths, or poor waveform tracing should cause prompt evaluation of a patient in the PACU. In addition to the use of pulse oximetry and end tidal capnometry, PACU nurses must be trained as vigilant monitors of a patient's ventilatory status specifically observing the following behaviors:
33
1. Bradypnea—a respiratory rate of more than eight breaths per minute; 2. Apneic episodes >10 s; 3. Pulse oximeter reading (SaO2) < 90% (on supplemental O2, CPAP, or room air).
In 2007, Gali et al. 34 used a preoperative sleep apnea clinical score (SACS) in combination with the above-listed PACU events to develop a practice management plan for surgeons and anesthesiologists to identify patients at high risk for oxygen desaturation after PACU discharge. Although the SACS is not the same as a STOP-Bang score, it does share similar variables (neck circumference, presence of hypertension, frequency of snoring, observed gasping/choking during sleep) and is used as clinical prediction score. Patients in this study with a high SACS, who demonstrated the above postoperative behaviors at repeated intervals, did have more desaturation events following PACU discharge. A second study by the same group looked at 693 patients to determine if a SACS score, or SACS plus recurrent PACU events, was associated with postoperative respiratory events. 35 Those patients with a high SACS had an odds ratio of 3.5 (p < 0.001) compared with those with low SACS. Notably, those with high SACS in addition to recurrent PACU events had an OR of 21 (p < 0.001) of having a postoperative respiratory event (admission to an ICU for a respiratory indication: respiratory failure, need for respiratory therapy intervention not including bronchodilators, need for noninvasive ventilation, or development of postoperative pneumonia) compared with a low SACS. As this study demonstrates, a two-step screening process may confer benefit to patients. A pre- and postoperative assessment cannot definitely prevent unexpected or undesired outcomes in this population but certainly has been shown to be an advisable strategy in caring for sleep apnea patients.
Hypopnea may not as easily be detected in the PACU as other listed behaviors, but it does present concern to the patient care team. Anesthesiologists and perioperative nurses with a trained eye can often detect insufficient ventilation in spontaneously breathing patients in the recovery room. Sampling of arterial blood to confirm elevation of the PaCO2 can aid in the diagnosis of hypoventilation. If hypopnea is suspected, this can be included as an at-risk behavior when determining therapy and bed placement.
Screening for PACU events should be documented at 30 min intervals for 90 min. Importantly, to be able to document sleep apnea risk, the patient must be observed resting undisturbed for at least 30 min of this period. Frequently, a postoperative patient will have a normal respiratory rate and no suspected hypoventilation but will be unable to maintain normal oxygen saturation levels (>90%) on room air. If a baseline serum HCO3− is unavailable, the patient should be observed resting for an additional 90 minutes. If able to maintain normal arterial saturation, they may be discharged to an unmonitored bed. If not, CPAP should be initiated and the patient transferred to a monitored bed (Fig. 3).
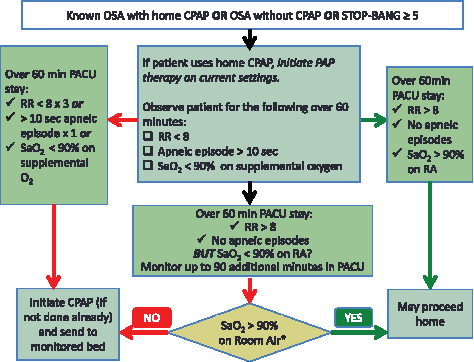
Post-anesthesia care unit obstructive sleep apnea (OSA) screening algorithm. *Observation made while resting undisturbed. Color images available online at www.liebertpub.com/bari
If baseline serum HCO3− is available, it can be used to decide on appropriate therapy and bed assignment. If the serum HCO3− is <28 mmol/L, the patient may be observed in the PACU for an additional 90 min with continued trials on room air. If oxygen saturation can be maintained for 60 min on room air, the patient may proceed to a floor bed. If not, the patient should be evaluated for PAP therapy and sent to a monitored bed. Likewise, for patients whose room air SaO2 < 90% and serum HCO3− is ≥28 mmol/L, PAP therapy should be considered and an admission arranged for a monitored care environment (Fig. 4).
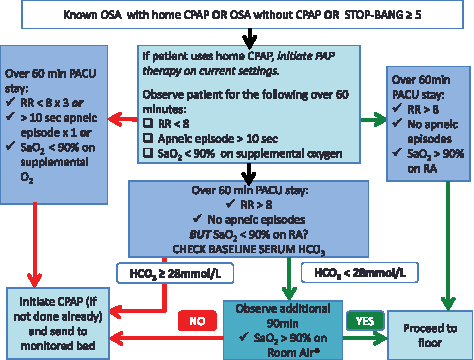
Post-anesthesia care unit OSA screening algorithm using baseline serum bicarbonate. *Observation made while resting undisturbed. Color images available online at www.liebertpub.com/bari
The 2006 ASA guidelines recommend that patients with OSA remain monitored in a PACU 7 h past their last hour of obstructive behavior. It would be unlikely that a patient would experience significant respiratory events following a 60 min PACU stay without respiratory events. However, caution must be exercised in prescribing increased opioids or other sedatives. If concerns exist in transitioning a patient to floor medication orders, an extended PACU stay can be considered for initiation of these orders in a monitored environment.
Patients exhibiting behaviors in the PACU that require admission to a monitored bed and CPAP therapy need a sleep study referral upon hospital discharge (Fig. 5). Educational material needs to be provided to the patient, ideally his/her primary care physician, and if possible should include contact phone numbers/addresses to local sleep centers to assist with appointment scheduling.
Sample referral letter for patients with suspected OSA.
PAP Therapy versus Supplemental Oxygen
Prior to initiating an OSA algorithm at the authors' hospital, most known OSA or suspected OSA patients were not provided PAP therapy. Instead, supplemental oxygen was started in the PACU and continued on the floor. Oxygen therapy may reduce the number of desaturation events associated with the disease, but CPAP has been established as the treatment choice for OSA. 36
In 2013, a meta-analysis evaluated oxygen versus CPAP therapy in patients with OSA defined by an AHI >5 events per hour on polysomnogram. 37 The review evaluated prospective studies with patients using CPAP, oxygen, or placebo as the intervention. CPAP versus nocturnal oxygen does not demonstrate an improvement in oxygenation; it does, however, decrease the apnea hypopnea index (SMD −3.37). Oxygen therapy may in fact extend apneic times in patients with OSA, 38 placing them at risk for hypercarbia and ultimately respiratory failure. A particular focus of medical teams caring for the patient population undergoing bariatric surgery should include education about the altered pulmonary mechanics of obese patients (obstructive lung disease, decreased functional residual capacity, and increased closing capacity). These physiologic changes are further worsened by general anesthesia (increased atelectasis, decreased lung volumes, altered respiratory timing), opioids, and sedatives. Undetected hypoventilation due to normal oxygen saturation levels in the setting of oxygen therapy may exacerbate apneas and place patients at increased risk. CPAP therapy, instead of oxygen, should be considered in bariatric patients as a first-line treatment for hypopnea and obstructive airway behavior.
Recently, the New England Journal of Medicine published a randomized, controlled trial of 318 patients with OSA assigned to sleep hygiene with healthy lifestyle information alone (exercise and diet instruction), or healthy lifestyle education in addition to nocturnal oxygen therapy or CPAP. 39 All patients had known coronary artery disease or multiple cardiac risk factors, including hypertension, diabetes mellitus, or smoking. The groups receiving oxygen therapy and CPAP both had reductions in nocturnal hypoxemia, each having at least a 2.6% drop in the time in which oxygen saturation was <90%. Cardiovascular risk was assessed at 12 weeks; the CPAP group's mean arterial pressure was significantly lower than the education plus oxygen group (p = 0.02). Thus, despite the fact that sustained hypoxemia is associated with blood pressure elevation, the reduction in desaturation events in the oxygen therapy group did not result in decreased blood pressure. In the absence of oxygen therapy showing advantage over CPAP for the treatment of upper airway obstruction, and with evidence to suggest CPAP decreases cardiovascular risk, PAP should be considered the first-line treatment for PACU respiratory events when OSA is suspected.
Monitored Beds and PAP Therapy
If events occur at two or more 30 min intervals in the PACU (the same event or varied events), the patient should be considered at risk for continued respiratory compromise after PACU discharge. A monitored bed (step-down or ICU based on hospital resources) needs to transmit vital sign data to a central station, a telemetry room, or to a nurse alarm system. Bedside monitors without an alert capability to obtain a member of the medical team immediately may not prevent respiratory compromise or postoperative opioid-induced respiratory depression. 40 Patients scheduled to have same-day surgery exhibiting apneas, bradypneas, and/or desaturation events in the PACU (on CPAP, face mask, nasal cannula, or room air) will need to be admitted and monitored for at least one night postoperatively. Alternatively, patients may remain in the PACU or a clinical decision unit with monitored beds as a 23 h observation (vs. hospital admission).
PAP therapy may provide benefit to patients not already using it routinely, and should be initiated in the PACU for continuation and titration in a monitored care environment. Involving respiratory therapy as needed to help set up a device for patient comfort and titrate positive pressure to a patient's need is recommended.
For patients using a home CPAP device, respiratory therapy can be consulted to evaluate the machine and patient. If there is suspicion that the device is not functioning, a hospital CPAP machine should be used at the patient's home setting. If a seal cannot be created with the face mask/nasal mask or nasal pillows (e.g., presence of an NG tube), an alternative device may need to be tried. If the hospital device CPAP settings are increased (as compared with home machine settings) as means to keep the patient's airway patent, or supplemental oxygen needs to be added to the home/hospital CPAP device, the patient should be placed in a monitored bed.
Floor/Home CPAP
For patients with known OSA using home CPAP, it is imperative that the patient continue to use their device postoperatively. PAP therapy needs to be used at all times while a patient is sleeping. Floor orders from the anesthesiologist/surgeon need to involve nursing/respiratory therapy staff in assisting the patient in placing the device both at night and while napping during the day. This information should be provided to the patient and the patient's family preoperatively to prepare them for CPAP use in the hospital. Discharge instructions should also be provided outlining CPAP use in the postoperative period, particularly for the timeframe in which the patient is to remain on opioid therapy for pain control (Fig. 6).
Sample patient instructions for postoperative CPAP use.
Conclusion
Patients with OSA deserve special consideration in the surgical setting. General anesthesia as well as several commonly used medications such as opioids, benzodiazepines, antihistamines, and anti-emetics have the potential to exacerbate apneic and hypopneic episodes. A preoperative screening algorithm enables surgeons and anesthesiologists to refer appropriate patients for sleep study, determine the most suitable surgical environment, and plan for intraoperative care needs. The postoperative screening tool should be used to risk stratify patients further to determine their monitoring and treatment needs. To date, no perioperative OSA algorithm has been proven to prevent complications in patients undergoing surgery; future trials and outcome studies will continue to modify the current care approach. A designated care strategy, for both those diagnosed with OSA and those with suspected disease, serves to raise awareness of perioperative risk and increases vigilance when these patients are most vulnerable.
Footnotes
Author Disclosure Statement
No competing financial interests exist.