
Abstract
Background:
Anastomotic strictures at the gastrojejunal anastomosis (GJA) are relatively common after a laparoscopic Roux-en-Y gastric bypass (LRYGB). There are three different ways to perform a GJA: circular stapled (CS), linear stapled (LS), and hand-sewn (HS). The CS technique provides the most standard diameter, and the LS and HS techniques can be standardized by using a bougie to calibrate the diameter of the anastomosis. However, they can all become strictured. This study examines the stricture rate of a hand-sewn GJA over a 4-year period.
Methods:
A prospectively maintained database was used to retrospectively evaluate patient outcomes at our bariatric center. This database was evaluated for strictures. The gastric bypasses were performed over a 4-year period by a single surgeon. The technique remained standard over the study period. This was a two-layered HS anastomosis with four different sutures of an absorbable suture (2.0 VICRYL®). Inclusion criteria were primary laparoscopic gastric bypasses. Exclusion criteria were revisions and conversions to open procedures and combined procedures.
Results:
From 2010 to 2013, there were 454 primary LRYGB. The overall stricture rate was 3.1% with 14 patients. This varied by year from a low of 0% in 2013 to 4.2% in 2012. The average time to stricture was 57.5 days with a standard deviation of 29 days. One patient had a recurrent stricture, and all patients responded to pneumatic dilation.
Conclusions:
A two-layered HS anastomosis has an acceptable rate of stricture. These strictures are early and respond well to pneumatic dilation.
Introduction
T
Materials and Methods
A prospectively maintained database was used to retrospectively evaluate patient outcomes at our bariatric center. The database was maintained according to Health Insurance Portability and Accountability Act guidelines, and the patients also signed an informed consent allowing use of their deidentified data for study purposes. The study was also adherent to the Declaration of Helsinki guidelines. This database included data on complications. The gastric bypasses were performed over a 4-year period (2010–2013) by a single surgeon. The technique remained standard over the study period. This was a two-layered HS anastomosis with four different sutures of 2.0 VICRYL®. The inclusion criteria were all consecutive patients undergoing primary laparoscopic bypasses, age >18, and patients that had no early reoperations. Exclusion criteria were revisions and conversions to open procedures and combined procedures. This database was evaluated for patients that developed a stricture at the GJA. The technique for the creation of the GJA remained standard over the study period. This was an antecolic two-layered HS anastomosis with absorbable sutures over a 34 Fr bougie. The patient's chart was then examined for radiographic studies, endoscopies, treatments, and outcomes. The patients that presented with stricture underwent pneumatic endoscopic balloon dilation. All patients responded well to the dilation.
Surgical technique
The technique of performing the HS anastomosis in this series was as follows: the gastric pouch was created by multiple firings of an endoscopic LS to the size of approximately 20 cc. Staple line reinforcement with absorbable material was used for creation of the gastric pouch, except for the first firing of the stapler, in the portion of the gastric pouch where the small bowel was attached to create the GJA. The small bowel was then divided 40 cm distal to the ligament of Treitz, and a 100 cm Roux limb was measured. A posterior outer layer of 2.0 VICRYL is used to connect the Roux limb to the gastric pouch. A gastrotomy and also an enterotomy were created with electrocautery. A two-layer hand-sewn anastomosis using absorbable suture was then performed over a 34 Fr bougie. This used four different sutures. Dyed 2.0 sutures are used for the outer layers and undyed suture for the inner layer. An intraoperative air leak test with an endoscope was performed in all cases (Figs. 1–4).

Outer posterior layer of gastrojejunal anastomosis (GJA).
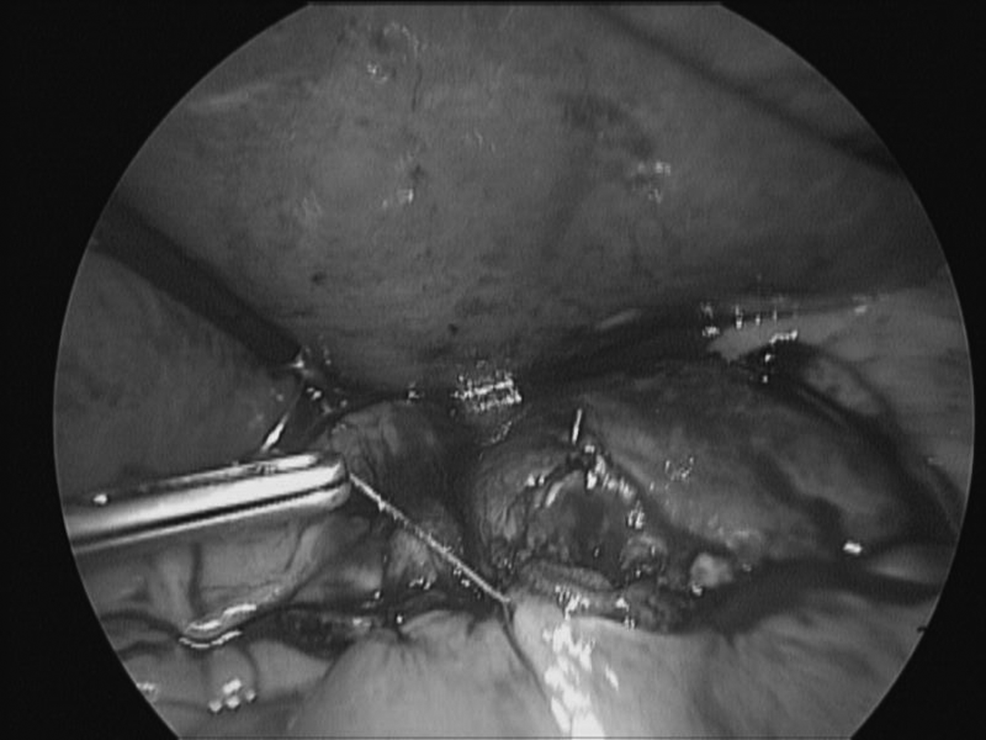
Inner posterior layer of GJA.

Anterior inner layer of GJA

Anterior outer layer of GJA.
Results
Between 2010 and 2013, 454 patients underwent primary laparoscopic Roux-en-Y gastric bypass (LRYGB) surgery. Fourteen patients presented with stricture in the study period. There were five males and nine females that presented with stricture. With 14 documented cases of stricture at the GJA, the overall stricture rate was 3.1%. The rate varied by year with no strictures in 2013 to a high of 4.2% in 2012 (Table 1). The average time to stricture was 57.5 days with a standard deviation of 29 days. There was a wide variation in average time to stricture by year. In 2011, the average time to stricture was 38 days, but in 2010, the time to stricture was 81 days. The time to stricture in 2012 was 52 days so the learning curve of accumulated case volume does not seem to matter. Only one patient had a recurrent stricture, and all patients responded well to pneumatic endoscopic dilation. Ulceration of the anastomosis occurred with the stricture in 3 of the 14 patients.
GJA, gastrojejunal anastomosis; HS, hand-sewn; LRYGB, laparoscopic Roux-en-Y gastric bypass.
Discussion
This series is comparable to other published series in regard to the stricture rate of a HS GJA. The published literature is full of articles that report a single surgeon or a single-center experience (Table 2). The rates of stricture of the GJA vary widely, even within the confines of the same technique. There are likely many factors that play into the development of a postoperative stricture. These include surgeon-specific factors, such as method of creation of the GJA, type of suture used, diameter of the anastomosis, surgeon experience, size of the CS and bougie, and tension of the GJA, just to name a few. Patient-specific factors are probably just as important, but more variable. These include factors such as BMI, smoking status, NSAID use, other medications, sex, age, and possibly even geographic location and H. pylori infection.
CS, circular stapler; CS21mm, circular stapler 21 mm; CS25mm, circular stapler 25 mm; GJS, gastrojejunostomy; LS, linear stapler.
In this series, we observed stricture rates in a LRYGB surgery using a HS GJA. Patient demographics did not vary significantly, and our technique was consistent. In fact, we had already performed over 400 gastric bypasses using this technique, and the time period studied was chosen to prevent any bias that could be attributed to the learning curve.
Hand-sewn
There is wide variation in the literature regarding stricture rates in the hand-sewn technique. Higa et al. reported using the HS GJA technique in 1040 LRYGBs. 1 They demonstrated a 4.9% stricture rate. They also used a two-layer technique with absorbable suture. Swartz et al. had a stricture rate of 15.2% in 1344 cases. 2 They used an inner layer of absorbable sutures with an outer layer of permanent sutures over a 34-Fr tube. Qureshi et al. presented one of the lowest rates found in the literature of 2.8% in 177 cases using HS. 3 This was with a two-layer absorbable suture technique over a 34-Fr tube. Also using the HS technique, Gonzalez had a 3.5% stricture rate with only 87 cases. 4 The stricture rates can also range higher, as reported by Bendewald et al., who had a rate of 7.7%, and 36.6% by Abdel-Galil and Sabry.5,6
Circular stapler
Using the 25 mm CS for the GJA provides the most consistent and standard technique. The diameter of the stapler is standard and not dependent on the technical ability of the individual surgeon. Qureshi et al. showed a 1.18% rate of stricture with a 25 mm CS. 3 Gould et al. showed a considerably higher rate of stricture of 15.9% with a 21 mm CS, but when they switched to a 25 mm CS, their rate dropped to 6.2%. 7 Nguyen et al. had a similar experience with a stricture rate of 26.8% with a 21 mm CS, but saw it drop to 8.8% using a 25 mm CS. 8 The stricture rate for the 21 mm CS is widely regarded as too high, the smaller CS has fallen out of use, and the 25 mm stapler seems to have replaced it.
Linear stapler
Our review of the literature showed very little significant difference in stricture rates of the LS groups. Abdel-Galil and Bendewald had a similar rate at 6.6% and 6.0%, respectively. Qureshi reported a low rate of 4.42%, while Gonzalez had no strictures with the LS technique.
Madan et al. reported that from 215 bariatric surgeons performing a GJA, 43% use CS, 41% use LS, and 21% a HS technique. 9 Surgeons that performed all three types of GJA showed variance in the stricture rate between different techniques.
The rate of stricture in our study compares favorably to the published literature. There are many factors that can contribute to the formation of strictures when performing a HS GJA, both surgeon and patient specific. At 3.1%, our rate of stenosis is acceptable and the strictures respond well to pneumatic dilation. Revisions were not included in this series, but the hand-sewn technique seems ideally suited for revisions. This technique can overcome the differences in tissue thickness and other anatomic changes that are seen with previous surgery. There are pitfalls to any technique, but the sutured anastomosis is more forgiving than a stapled anastomosis. For example, a broken suture is relatively easy to fix, especially compared to a misfired stapler. In the early postoperative period, suture can be seen intraluminally on endoscopy and may be associated with ulcer formation, but an absorbable suture should be gone within 4–6 weeks. Although the hand-sewn technique is more challenging to master, the outcomes are as good as stapled techniques and the skill set that comes along with it can help surgeons deal with difficult intraoperative situations.
Conclusion
A two-layered hand-sewn anastomosis has an acceptable rate of stricture. These strictures occur early and respond well to pneumatic endoscopic dilation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.