
Abstract
Introduction:
The intragastric balloon (IB) can be indicated for patients with overweight and obesity refractory to behavioral and medical treatment. In unusual situations, fungal colonization of the IB is observed, sometimes on their content, asymptomatic in most cases. The rare incidence of colonization is presented as the result of a multifactorial involvement, which predisposes to opportunistic infections.
Case Report:
Thirty-seven year old obese female, 87.5 kg, and body mass index 35 kg/m2. An adjustable intragastric balloon was indicated for treating obesity. At the end of the second month of treatment, she started presenting epigastric pain, postprandial fullness, and vomiting. The computed tomography showed abnormal balloon inflation, with air inside. The management adopted was to carry out total evacuation of the adjustable balloon, followed by new insufflation with nystatin solution added to methylene blue solution.
Discussion:
The contamination of the IB and its content raises the possibility of gas production inside the balloon by fungal fermentation, resulting in increased balloon volume leading to obstructive symptoms. In these situations, typically the balloon is removed and pharmacologic treatment is not necessary. In this case, it was shown well succeeded by no recurrence of hyperinflation with gas.
Introduction
T
IB is inserted endoscopically and then filled with 400–700 mL of saline and methylene blue solution under direct vision.1,2 In an Italian study with 2515 patients, Genco et al. showed an overall complication rate of 70/2515 (2.8%). Gastric perforation occurred in 5 patients (0.19%), gastric obstruction in 19 (0.76%), balloon rupture in 0.36%, esophagitis at 1.27%, and gastric ulcer in 0.2%. 3
In unusual situations, fungal colonization of the IB is observed, sometimes on their content, asymptomatic in most cases (Table 1).4–6 The rare incidence of colonization is presented as the result of a multifactorial involvement, which predisposes to opportunistic infections such as gastric stasis, smoking, and use of antacid drugs. Colonization is generally asymptomatic and in the outside area of the IB. In most cases, it is discovered at the time of removal, sometimes altering the physical characteristics of IB, making it more brittle and hardened, which can make removal more difficult. When symptoms are present, they are nonspecific as epigastric pain, vomiting and, in severe cases, dysphagia because of esophageal colonization.
Case Report
A 37-year-old obese female, 87.5 kg in weight, and body mass index (BMI) 35 kg/m2, with many unsuccessful attempts at weight loss with dietary restriction and medications for more than 2 years. After evaluation with the multidisciplinary team, the use of an adjustable intragastric balloon (AIB) for a year was indicated for treating obesity.
After the initial period of adaptation, the patient showed a satisfactory evolution with loss of 12.6 kg (BMI 30 kg/m2) until the end of the second month of treatment when she then started presenting epigastric pain, postprandial fullness, and vomiting. The computed tomography (Fig. 1) showed abnormal balloon inflation, with air inside. The patient was submitted to an endoscopic evaluation that showed a visually hyperinflated balloon with marked fluid level with about 50% of the balloon with air (Fig. 2).
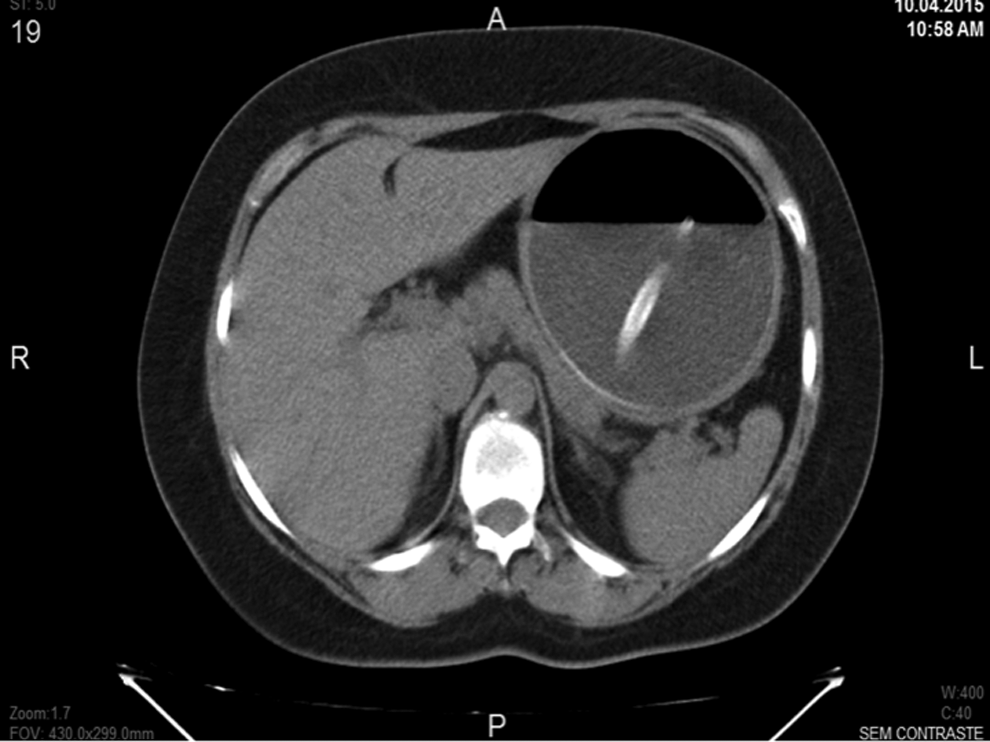
Abnormal balloon inflation with air inside. A computed tomography image.
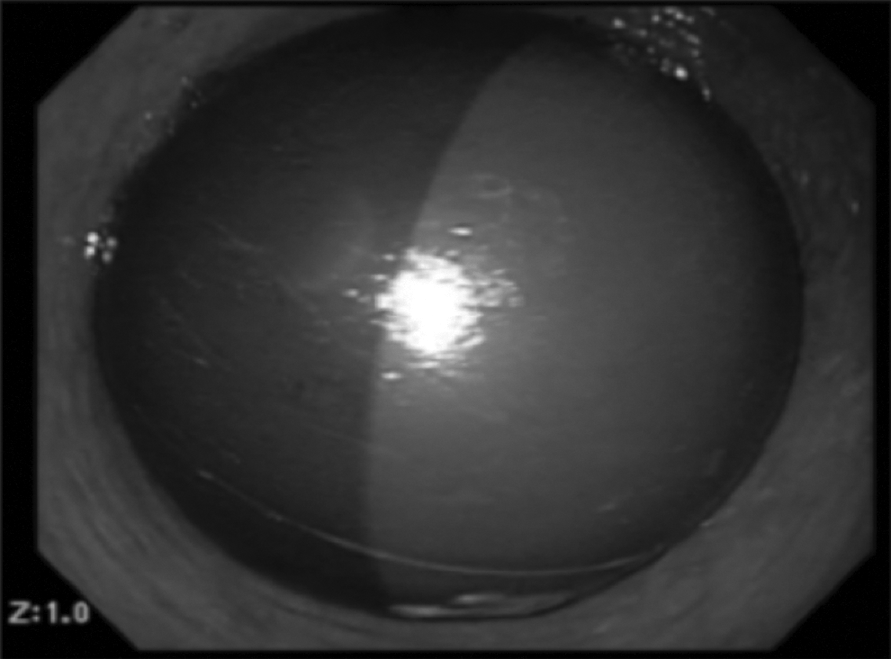
Intragastric balloon with gas hyperinflated.
The management adopted was to carry out total evacuation of the AIB, with the first 50 mL designated for culture (which identified the presence of Candida sp.), followed by new insufflation with 10 mL of nystatin solution (1,000,000 units) added to 600 mL of methylene blue solution (Fig. 3).

After insufflation with 600 mL methylene blue +10 mL nystatin solution.
The follow-up was taken with nutrition and endoscopy staff. A new tomography showed a correctly located balloon in gastric fundus and with no gas. There was no need of other interventions. After 6 months, the patient remained asymptomatic with current weight of 68 kg, weight loss so far of 19.5 kg, and BMI of 27.24 kg/m2 (22.28% of initial weight). Removal was planned for 12 months.
Discussion/Conclusion
The IB has a structure of silicone elastomer, and the in vitro study shows that the silicone coating materials are susceptible to adhesion of Candida. 7 The candidiasis of the gastrointestinal system mainly affects the esophagus, and the infection is seen as white mucosa plaque-like lesions. 8 Although a typical fungal infection is not usually detected in the esophagus of the patient, such contamination cannot be excluded and can occur during endoscopic intervention, that is, the passage of the balloon through the oral cavity or during application.
Nystatin is a polyene antifungal antibiotic obtained from Streptomyces noursei and its molecular formula is C47H75NO17. Nystatin is both fungistatic and fungicidal in vitro against a wide variety of yeasts and yeast-like fungi. Candida albicans demonstrates no significant resistance to nystatin in vitro on repeated subculture in increasing levels of nystatin; other Candida species become quite resistant. Generally, resistance does not develop in vivo. Nystatin acts by binding to sterols in the cell membrane of susceptible Candida species with a resultant change in membrane permeability allowing leakage of intracellular components. Nystatin exhibits no appreciable activity against bacteria protozoa or viruses. Gastrointestinal absorption of nystatin is insignificant. Most orally administered nystatin is passed unchanged in the stool.
The contamination of the IB and its content raises the possibility of gas production inside the balloon by fungal fermentation, resulting in increased diameter and balloon volume leading to obstructive symptoms (nausea, vomiting, ulcers, ischemia, and punctures). In these situations, typically the balloon is removed and pharmacologic treatment is not necessary.
The choice for treating fungal contaminated IB by emptying and filling it up with nystatin in addition to methylene blue solution is an innovative approach based on rational control of local infection (Fig. 4). In this case, it was shown well succeeded by no recurrence of hyperinflation with gas. Despite the success of the approach in the present case, it still requires prospective randomized studies to confirm the effectiveness of the use of nystatin prophylaxis/treatment for fungal contamination in balloons that allow adjustment.
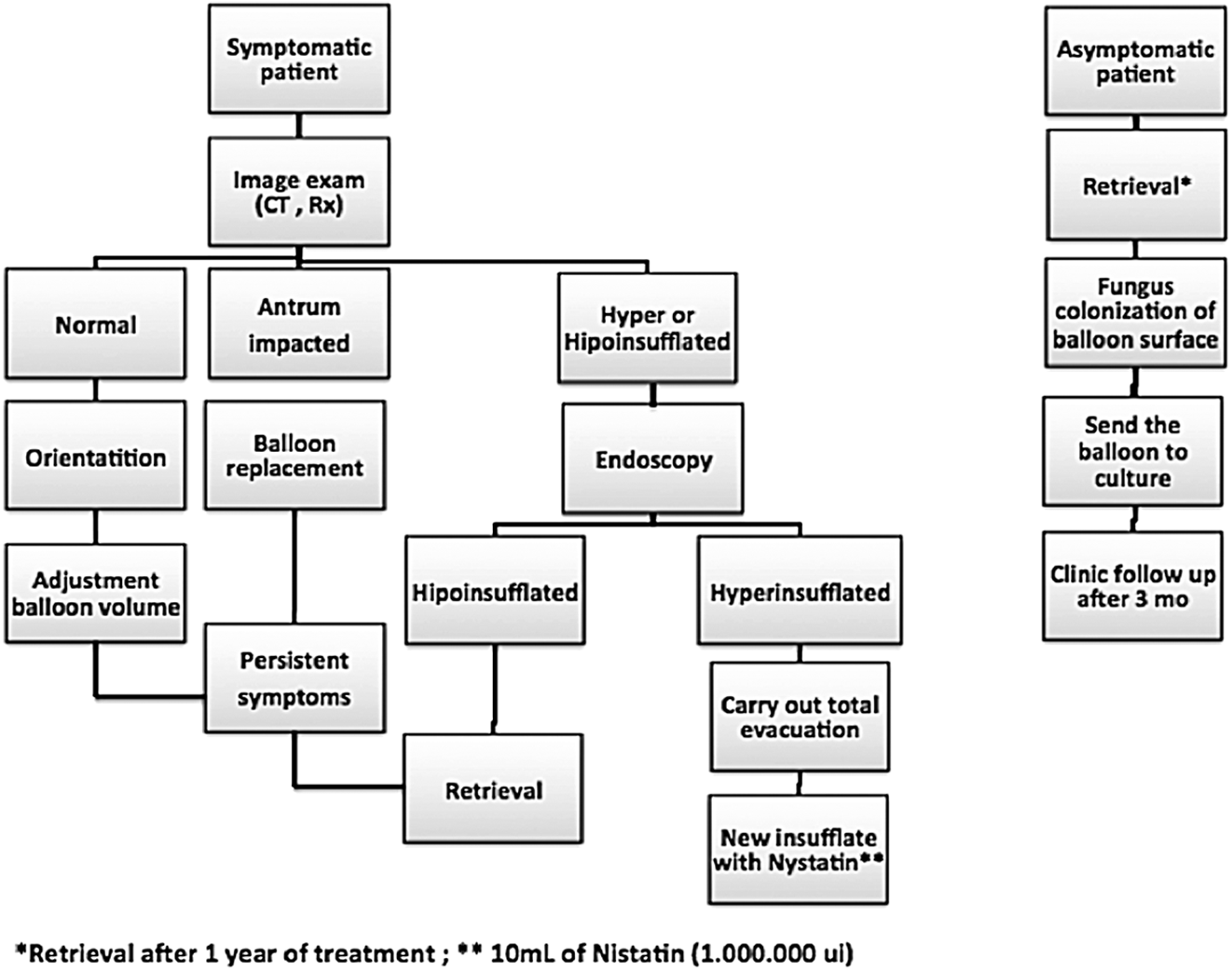
Algorithm for managing a symptomatic and asymptomatic patient during the treatment with an adjustable intragastric balloon for a year.
Footnotes
Author Disclosure Statement
No competing financial interests exist.