
Abstract
Background:
In obese subjects with type 2 diabetes mellitus (T2DM), the effect of laparoscopic greater curvature plication (LGCP) on the clinical improvement of T2DM is unknown. This study aims to investigate the effect of LGCP in improving the clinical profile of patients with T2DM.
Materials and Methods:
This is a retrospective study of obese subjects with T2DM who underwent LGCP between March 2011 and March 2013. Patients were followed up at different time periods. The efficacy of the procedure was investigated by using chi and t tests. Univariate and multivariate analyses were performed to investigate the predictors of excess weight loss (EWL).
Results:
Forty-three obese subjects (25 females, 18 males) with T2DM were enrolled. Mean age was 41.6 years. Preoperative mean ± SEM body–mass index (BMI) was 44.4 ± 0.8 kg/m2. Mean BMI decreased significantly at 1, 3, 6, and 12 months (p = 0.0002, p < 0.001, p < 0.001, and p < 0.001). Mean EWL was 20%, 32%, 42%, and 48% at 1, 3, 6, and 12 months of follow-up. At 1-year follow-up, a statistically significant decrease in mean serum fasting blood glucose (p = 0.001), HbA1c levels (p = 0.002), and Homeostasis Model Assessment (HOMA) index (p < 0.0001) was observed. Female sex (p = 0.013) and HOMA index (p = 0.009) were found to be independent predictors of EWL.
Conclusion:
LGCP is a safe and effective bariatric procedure for the management of obesity. Our findings show that in addition to significant weight loss, LGCP may contribute to the clinical improvement of T2DM in obese subjects.
Introduction
S
Over the past decade, laparoscopic greater curvature plication (LGCP) has emerged as an effective bariatric procedure for the treatment of obesity. 6 Findings from early studies have shown that LGCP is associated with significant long-term weight loss in obese patients, a significant reduction in perioperative morbidity, and early convalescence.7–9 The excess weight loss (EWL) in patients who undergo LGCP has been associated with preoperative body–mass index (BMI) and the reported risks and benefits vary for different grades of obesity. 9 Compared with other bariatric procedures, LGCP is less invasive and more conservative with a reversible potency with less risk of problems such as a leak. 8
Although previous investigators have demonstrated that different bariatric procedures may lead to clinical improvement of diabetes mellitus, little is known about the effect of LGCP on the clinical parameters of patients with diabetes mellitus. Furthermore, its impact on antidiabetic medication usage after the procedure has not been investigated yet. In this study, we sought to investigate the effect of LGCP on the clinical improvement in Turkish obese subjects with diabetes mellitus over a 12-month follow-up duration. We hypothesized that in addition to weight loss there may be a significant improvement in the clinical profile of type 2 diabetes mellitus (T2DM) patients who undergo LGCP.
Materials and Methods
This study is a local ethics committee-approved study conducted on subjects who underwent gastric plication at the Department of General Surgery, Bagcilar Training and Research Hospital, between March 2011 and March 2013. Subjects were selected for surgery based on the American Society of Bariatric Surgery guidelines. 10
Among all subjects (n = 258) who underwent laparoscopic gastric (greater curvature) plication within the study period, those with a previous diagnosis of type 2 diabetes mellitus (T2DM) (n = 43) were enrolled.
Data on subjects' demographics and anthropological parameters, including (height, weight, BMI), pre- and 1-month, 3-month, and 1-year postoperative laboratory results (metabolic profile; serum fasting blood glucose, HbA1c, triglyceride [TG], low-density lipoproteins, high-density lipoprotein [HDL]), serum insulin, and insulin resistance (HOMA-IR), were recorded into a prospectively maintained database. Information on previous drug history, including conservative weight loss measures adopted by subjects, were also noted and recorded. In addition, data on previous surgical history were recorded.
The effect of gastric plication on glucose and lipid metabolism was investigated by comparing preoperative and postoperative laboratory values at the different postoperative time points. Postoperative EWL was calculated in all subjects and its relationship with technique success was investigated. Statistical analyses were performed by JMP 10.0 (SAS Institute, Cary, NC) using Student's t and chi-square tests. Univariate and multivariate analyses were performed to determine the predictors of EWL in study subjects.
Operative technique
Preoperative preparations included prophylactic heparin, lower limb bandage, and antibiotic therapy. All patients were given proton pump inhibitors (PPIs) for a few days (less than a week) postoperatively. All operations were performed with the patient under general anesthesia.
A five-trocar technique was used. One 12-mm optical trocar was placed 5 cm above the umbilicus, one 12-mm trocar placed under the xiphoid for liver retraction, one 12-mm trocar placed at the left upper quadrant, one 5-mm trocar placed at the right upper quadrant, and one 5-mm trocar placed below the costal margin of the mid-clavicular line. Both procedures began with the dissection of the greater gastric curvature 4–6 cm from the pylorus up to the angle of His. Then, gastric plication was achieved by imbricating the greater curvature over a 34F bougie and by applying a first row of extramucosal interrupted stitch sutures. This was the template for a second row of extramucosal running suture line. At the end of the procedure, the shape of the stomach resembled that of a gastric sleeve. No drains were left in place. Upper gastrointestinal (GI) series with water-soluble contrast medium were performed on the first day after surgery to investigate the final shape for both procedures. Patients were discharged as soon as they accepted a soft diet without vomiting and received a prescription of PPI (single dose) and low-molecular-weight heparin, daily for 30 days. Ondansetron, cortisone, antiemetic, and the antispasmodic hyoscine were prescribed for 4 days only to alleviate mucosal edema resulting from venous stasis. The postoperative diet consisted of a soft diet for 4 weeks, followed by a progressive return to solid foods. Follow-up was scheduled at 3 and 6 months in the postoperative period. Gastric shape was reassessed on upper GI series performed on LGCP patients at 6 months for a better assessment of this investigational surgical treatment.
Results
Between March 2011 and March 2013, 258 patients underwent gastric plication surgery as a treatment for obesity at the Bagcilar Training and Teaching Hospital. Forty-three of these patients who had T2DM were enrolled.
Demographics and clinical characteristics of the study population are illustrated in Table 1. The study cohort had a mean ± SEM age of 41.6 ± 1.4 years and consisted of 25 females and 18 males. Preoperative mean BMI was found to be 44.4 kg/m2. Surgical-related comorbidities were recorded in 32.6% (n = 14) patients and five patients had a previous history of obesity-related intervention. Mean operative time was 85 min. All the procedures were performed uneventfully. The average duration of hospital stay was 3 days. During the follow-up period, four complications occurred and these included two subdiaphragmatic abscesses, one peripheral neuropathy, and one portal venous thrombosis. The subdiaphragmatic abscess was managed through percutaneous drainage and the other complications were managed medically.
Continuous variables are expressed as mean ± SEM. Categorical variables are given as percentages.
F, female; M, male.
During the follow-up period (12 months), the patients' BMIs were recorded at different time points (1, 3, 6, and 12 months). A dramatic decrease in mean BMI (44.4–40.4 kg/m2; p = 0.0002) was observed at 1-month postoperative follow-up. The decrease in BMI was also statistically significant at 3 and 6 months after surgery and most evident at 12 months after surgery (Fig. 1).
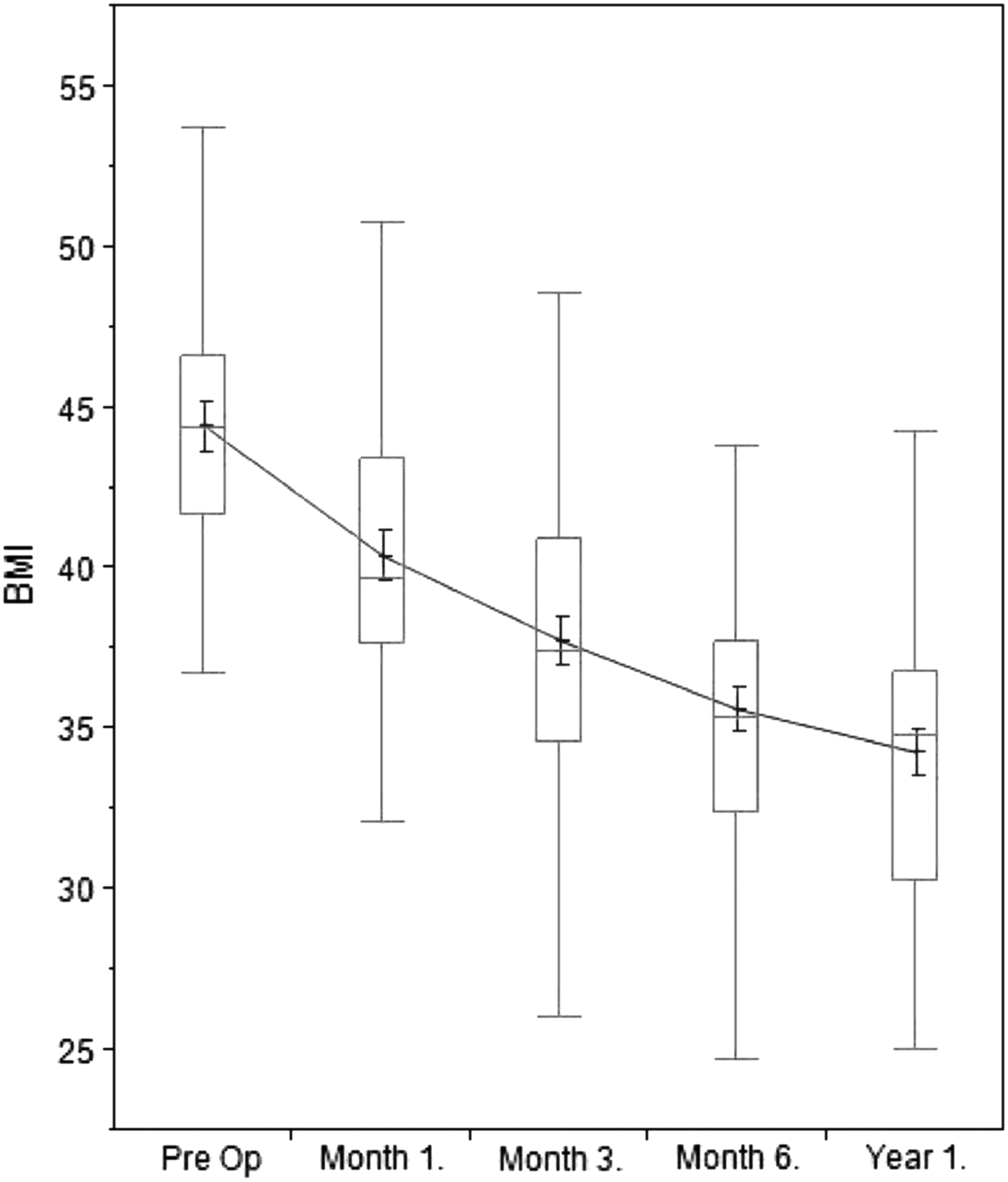
Body–mass index (BMI) change during 12 months.
EWL, which is defined as the percentage of excess weight that was lost during the follow-up period, was calculated and recorded for all patients during follow-up. Weight loss findings were in accord with the decrease in BMI over the 12-month follow-up period. Mean weight loss was 20% in the first month, 32% at 3 months, 42% at 6 months, and 48% at 12 months of follow-up (Fig. 2).
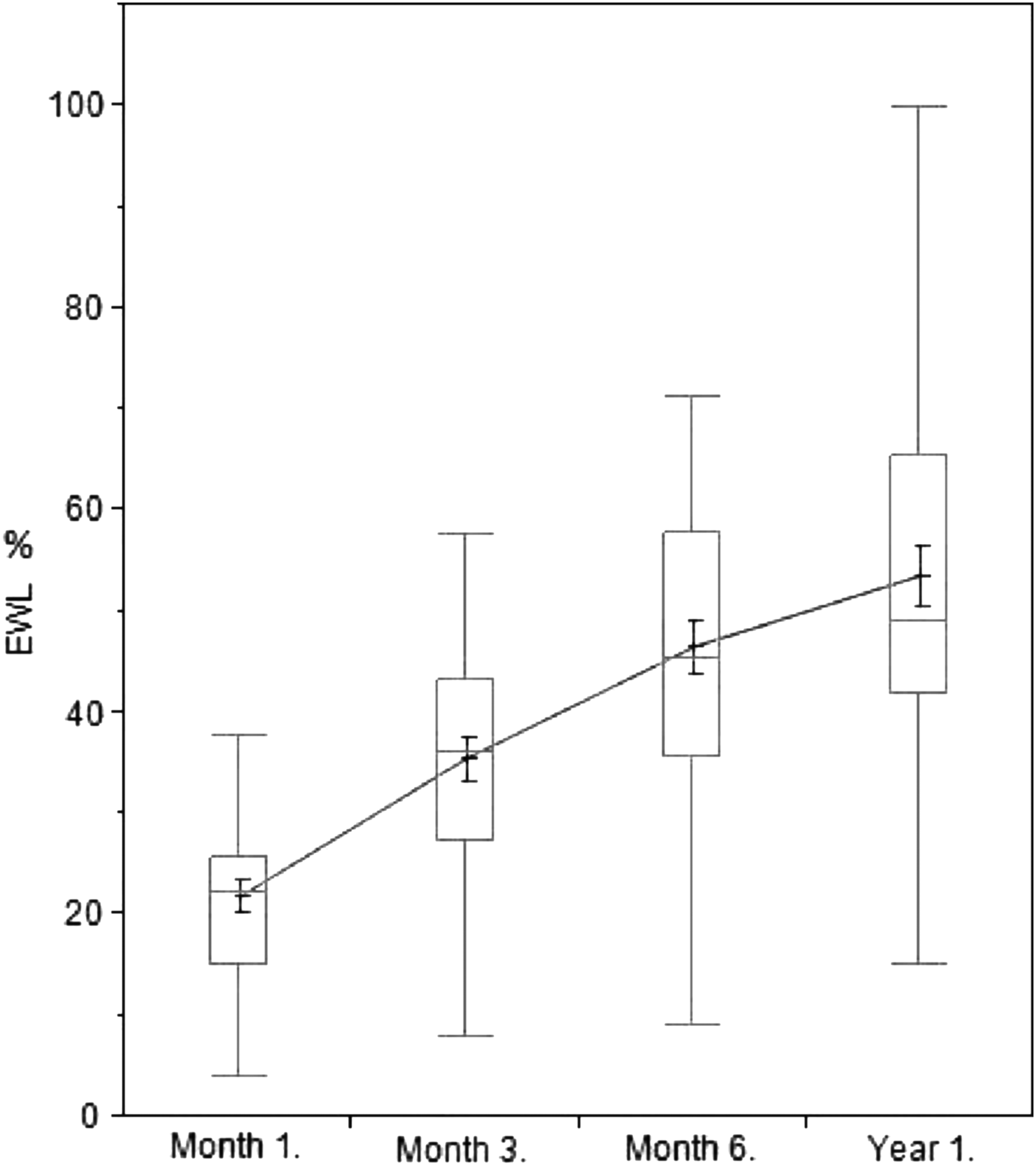
Excess weight loss (EWL) change during 12 months.
Table 2 shows the effect of the procedure on the metabolic parameters of patients before and 12 months after surgery. A statistically significant decrease in serum fasting blood glucose, HbA1c, insulin, TG, cholesterol, and Homeostasis Model Assessment (HOMA) indices was noted. Mean serum HDL levels also increased from 50 to 55 mg/dL (p = 0.054). This positive effect was also evident in the mean BMI of the patients, which decreased from 44.4 to 34.3 kg/m2 after 12 months of follow-up (p < 0.0001).
HDL, high-density lipoprotein; LDL, low-density lipoproteins.
The diabetic management protocol among patients was also investigated. Preoperative diabetic management consisted of insulin only (n = 4), metformin only (n = 28), insulin+metformin (n = 6), and diet (n = 5). At 12-month follow-up, only 1 patient remained on insulin, 16 on metformin, and 5 on (insulin+metformin). Overall, at least 76% of the patients were switched to diet only after 12 months of follow-up (p < 0.0001) (Table 3).
On univariate analysis, factors found to predict EWL were female sex (p = 0.0008), height (p = 0.054), and HOMA index (p < 0.0001). Female gender and HOMA index were independent predictors of EWL (p = 0.013, p = 0.009, respectively).
Discussion
In the current retrospective study, we present our experience with the laparoscopic gastric plication technique in 43 obese subjects with T2DM. To the best of our knowledge, this study is the first to investigate the effect of this technique on glucose and lipid metabolic parameters in T2DM obese subjects after a follow-up duration of 12 months. After a 12-month follow-up, serum levels of most metabolic parameters studied (glucose, HbAIc, insulin, TG, cholesterol, and HOMA index) decreased significantly. The success of the technique was also evident by the statistically significant decrease in EWL in all patients at1, 3, 6, and 12-month follow-up time periods.
Excess fat in the abdominal region as seen in obese subjects has been linked with metabolic abnormalities such as insulin resistance, hyperinsulinemia, glucose intolerance, dyslipoproteinemia, and comorbidities such as hypertension and diabetes mellitus.11,12 Previously reported studies have also documented an increase in T2DM risk by 3–10 times in subjects with high BMIs. 13 This risk is known to decrease by 50–75% after appropriate and successful weight loss management. 14
The benefits of bariatric surgery, which include appreciable weight loss and correction of existing comorbidities, have led to its incorporation into the management algorithm of obesity over the past two decades. Current surgical options include laparoscopic sleeve gastrectomy and gastric plication. The latter is a recently developed technique, which limits the gastric volume by invaginating the greater curvature of the stomach rather than gastric resection. 9 The laparoscopic bariatric surgery program at our institution was started in 2011 and since then over 750 procedures have been performed in about 700 patients.
The first series on LGCP was published by Talebpour and Amoli in 2007. The authors reported on 100 LGCP procedures in 76 female and 24 male obese subjects. Preoperative mean BMI was 47 kg/m2 and the procedures lasted in a mean time of 98 min (range 70–152 min). Mean hospital stay was 3 days (range 1–4 days). The patients were followed up for a mean duration of 18 months. The authors described the procedure as efficacious as EWL% at 1-, 6-, 12-, 24-, and 36-month follow-up time points was found to be 21.4%, 54%, 61%, 60%, and 57%, respectively. The safety of the procedure was also confirmed with a postoperative morbidity rate of 6%. 8 In this series, 13 patients who had T2DM had this condition resolved 6 months after surgery. Although smaller in size (n = 43), our findings are similar to that of Talebpour and Amoli. We observed a significant mean EWL% of 21.9%, 35.6%, 46.6%, and 53.7% at 1, 3, 6, and 12 months, respectively. In addition, about 76% of the subjects were switched to diet only after a follow-up duration of 1 year. Uniquely, the present study critically analyzed a larger cohort of obese subjects with T2DM, a number that was three times higher than what was reported by Talebpour and Amoli.
In the 2011 study by Skrekas et al., 6 the authors described their experience with 135 subjects who underwent LGCP in a mean operative time of 58 min (45–85 min). The mean follow-up period of the patients was 22.59 months (range 8–31 months). The morbidity rate reported in this cohort was similar (8.8%) to that reported by Talebpour and Amoli. In this study, a subgroup analysis based on BMI values showed that EWL% was significantly higher for patients with BMI less than 45 kg/m2 compared with patients with BMI greater than 45 kg/m2 (69.86 vs. 55.49, respectively, p = 0.006). Uniformly, inadequate weight loss was significantly higher (p < 0.001) in the group with BMI greater than 45 kg/m2. The incidence of complications did not make any difference with respect to BMI.
The effect of bariatric surgery on glucose and lipid metabolism in diabetic patients has been widely studied by previous investigators. Pories et al. 5 were the first to report the antidiabetic effect of gastric bypass surgery in 608 morbidly obese patients who were followed up for a mean duration of 7.6 years. What was striking about their report was that 121 of 146 patients (82.9%) who presented with noninsulin-dependent diabetes mellitus maintained normal values of blood glucose and glycosylated hemoglobin. Almost a decade later, a similar study that was conducted by Schauer et al. 3 documented normal fasting blood glucose and HBA1c levels in 83% (n = 199) and a significant improvement in 17% (n = 40) of 240 patients who underwent laparoscopic Roux-en-Y gastric bypass. In the present study, fasting blood glucose and HBA1c levels returned to normal in 12 patients and improved in 27 patients. This was evident in the management protocol of these patients as at least 76% of the entire study group was switched to diet only.
In a recent meta-analysis by Buchwald et al., the impact of bariatric surgery on type 2 diabetes in association with weight reduction was extensively studied. 4 The meta-analysis, which included 621 studies with 888 treatment arms and 135,246 patients, described complete resolution of the disease in 78.1% of diabetic patients and an improvement or resolution in 86.6% of patients. By procedure, weight loss and diabetes resolution were more evident in patients who underwent biliopancreatic diversion/duodenal switch, followed by gastric bypass, and least for banding procedures. Insulin levels declined significantly postoperatively as did HbA1c and fasting glucose values.
Although the present study is the first in the literature to investigate the effect of this technique on diabetes mellitus, it is limited by its smaller sample size and a shorter follow-up duration. In addition, it is difficult to conclude that the technique itself had a direct effect on the clinical improvement in T2DM status in all subjects. This remains a subject of controversy since several factors, such as compliance to treatment, genetic, or hormonal, can be held accountable for the clinical improvement observed. These factors kept the authors in the confines of drawing a more comprehensive conclusion.
Conclusion
In this study, we present our experience with laparoscopic gastric plication in a group of obese subjects with a history of diabetes mellitus. Our findings demonstrate the safety and efficacy of the procedure in terms weight loss and control of glucose and lipid metabolism in these patients. Although our short-term follow-up findings describe an appreciable improvement in metabolic parameters, the long-term benefits of this procedure are yet to be ascertained.
Footnotes
Author Disclosure Statement
No competing financial interests exist.