
Abstract
Background:
The failure of the conservative treatment of obesity and its close association with cardiovascular events have lead to a consensus deeming the surgical approach to obesity as a must. The aim of this study is to determine the efficacy and safety of Roux-en-Y Gastric Bypass (RYGB) in obesity and cardiovascular risk (CVR).
Methods:
A comparative observational retrospective cohort study based on clinical records of patients having undergone RYGB between January 1st, 2011 and January 1st, 2014. Data related to obesity are analyzed at four stages: the consultation during which the patient opts for surgical intervention, immediately before surgery, and at 3 and 9 months following surgery. Furthermore, the risk of cardiovascular event is estimated before RYGB and during the final ninth-month assessment.
Results:
Rates for immediate complications and quietus complied with safety criteria, being lower in proportion than those reported in recent publications. Effects on body mass index and excess body weight were significant with a reduction in both parameters, regardless of age and gender. CVR displayed an identical tendency whereby all subjects were classified as low risk during the final assessment.
Conclusion:
RYGB has proven to be a safe and efficacious alternative therapy overcoming limitations inherent in individuals.
Introduction
T
Therapeutic failure in the treatment of morbid obesity (MO) and its consequences in terms of quality of life and life expectancy have lead to a consensus suggesting treatment of this pathology be surgical, 5 an approach not free of risks. Thereby, a set of safety criteria have been established for this approach such as; mortality lower than 1%, morbidity lower than 10%, and a rate of less than 2% for repeat surgery. 6 Although several surgical alternatives exist, the scientific community is unanimous in ratifying that among all of them, Roux-en-Y Gastric Bypass (RYGB) is the treatment of choice in the greater majority of cases. 7 Furthermore, numerous research articles have reported that following this type of surgery, comorbid metabolic conditions associated with obesity undergo improvement or even remission,7,8 which suggests that RYGB may produce a decrease in cardiovascular risk (CVR). 9
The prevalence of MO in Spain has tripled over the last 15 years. 10 More specifically in the Region of Murcia, recent research in an urban population revealed that 43% of subjects presented obesity and of these, 6.4% were diagnosed with MO. 11
The aim of this study is to determine the efficacy and safety of bariatric surgery (BS) performed using the RYGB technique as a treatment for obesity and CVR, while also examining possible relationships with the sociodemographic characteristics of the study population.
Materials and Methods
Design and subjects
This retrospective observational study involved 146 patients subject to RYGB at the Virgen de la Arrixaca Clinical University Hospital (HCUVA), situated in Murcia, Spain. The inclusion criteria required the existence of clinical bariatric follow-up records as compiled by the Endocrinology and Nutrition unit of the HCUVA between January 1st, 2011 and January 1st, 2014 (Fig. 1). The selection of medical records was made from the data base of persons registered in Area 1 of the public health system of the region of Murcia, Spain.
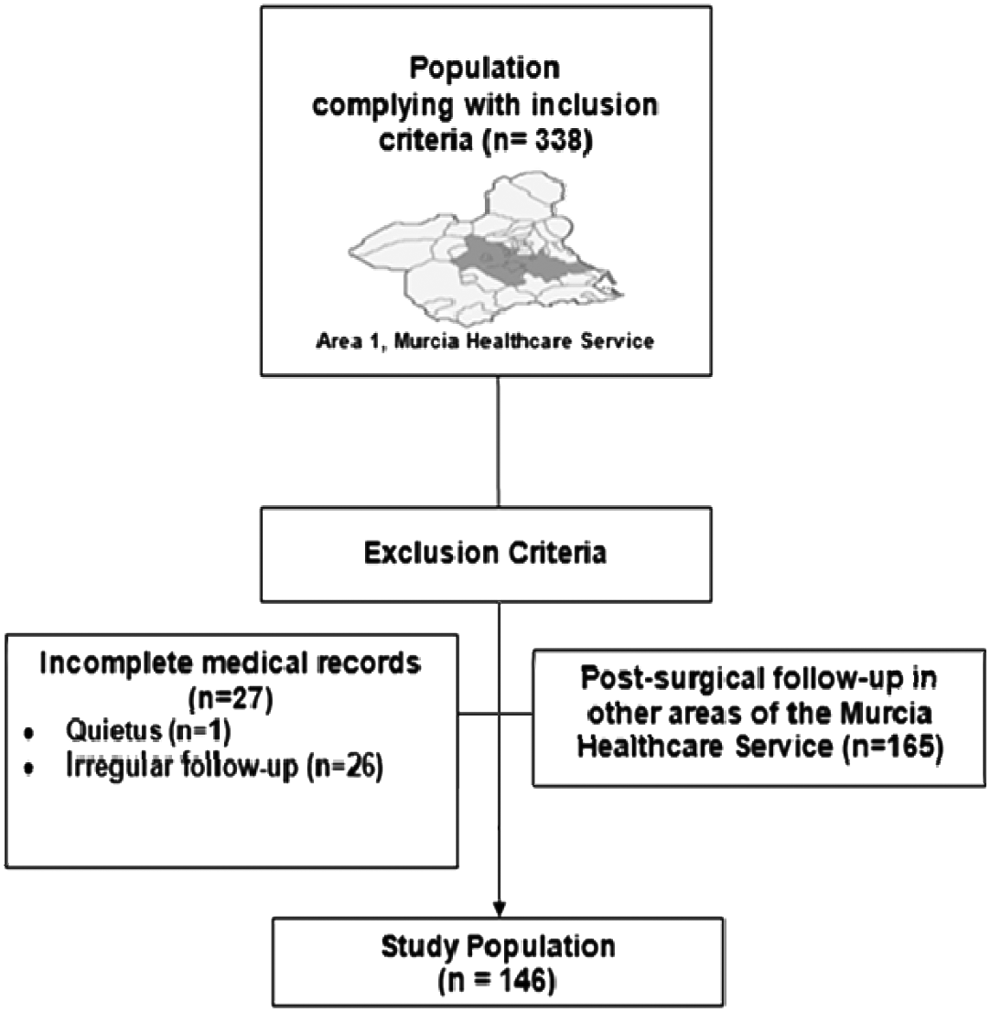
Selection criteria diagram.
Over the research period, data regarding obesity and comorbidity were collected, together with other related variables at three stages in time: before surgery, at 3, and at 9 months following RYGB. Data were also obtained for obesity-related variables during the consultation in which the patient opted for this surgical procedure.
Procedure
This research was approved by the HCUVA ethics committee on May 22nd 2014 and registered with the Department of Records and Codification. Thereby, complete anonymity and confidentiality are assured for all patients whose data and information were subject to analysis, in accordance with Spanish law: Ley Orgánica 15 as on 13th of December 1999 on the Protection of Personal Data. Following receipt of permission, the data were retrieved from medical records (in both electronic and physical format) and protected by password.
The data obtained from the medical records were arranged according to sociodemographic variables (gender, psychiatric, and cardiovascular background), substance abuse (alcohol, tobacco, and/or cannabis consumption), current RYGB surgery variables (age at which surgery was performed, type of anastomosis: 100/150, 100/200, and 100/250, and postsurgical complications over the first 30 days), and anthropometric data (height and weight), as well as clinical and analytical variables (systolic blood pressure [SBP], diastolic blood pressure [DBP], total cholesterol [TC], and high-density lipoprotein cholesterol [HDL-C]).
Measurement
This study was performed according to the guidelines of the Spanish Society for Study into Obesity (SEEDO) (Table 1), using the body mass index (BMI); weight in kilograms divided by height in meters squared. Furthermore, excess weight (kg) for any given patient was calculated by first obtaining the recommended upper weight limit corresponding to a BMI of 25 kg/m2. Once this figure was obtained, excess weight was calculated as the difference between the ideal weight limit and the real weight of the patient.
BMI, body mass index.
To estimate the risk of CVD at 10 years, the Framingham cohort methodology was utilized. Risk factors included in the Framingham equation were as follows: age, gender, TC, HDL-C, SBP (treated and nontreated), diabetes mellitus, and tobacco smoking (smoker or nonsmoker). 13 According to the scores obtained for each risk factor, the subjects were classified into three categories for absolute risk at 10 years: low (<10%), intermediate (10–19%), and high risk (≥20%).
Data analyses
Statistical analyses were performed using the SPSS software version 22.0, with statistical significance set at p < 0.05. Variables were analyzed by basic descriptive statistical calculations, frequencies, arithmetical average, and standard deviation, all with a confidence interval of 95%.
Regarding hypothesis contrast testing, Student's t-test was used for the bivariate analysis of independent samples. The chi-squared test was utilized for qualitative variables. McNemar's nonparametric test was applied for the analysis of two-paired proportions, while Cochran's Q test was used for more than two correlated proportions.
A partially repeated measures analysis of variance was performed as a multivariate analysis to study the efficacy of RYGB surgery taking gender into account. This test was also used to contrast anthropometric and CVR values regarding the different Roux-limb lengths.
Results
Sample characteristics
The mean age at which patients underwent RYGB was 42.24 ± 11.94 years (confidence interval [CI] 95% 37.06–44.23), with ages ranging from 18 to 68 years of age. The male gender represented a minority group within the study population (30.8%). With regard to cardiovascular background, 6.8% had experienced at least one cardiovascular event before BS and 18.5% had been diagnosed with mixed anxiety-depressive disorder and were undergoing pharmacological treatment. The low incidence in substance abuse is worthy of note (27%) (Fig. 2).

Substance abuse. Subjects answering NO did not use tobacco, alcohol, or cannabis. Subjects answering YES admitted using tobacco, alcohol, and cannabis.
Overall, 16.5% had experienced failure of previous BS of some form; 23 subjects (15.8%) with Adjustable Gastric Band; and only one with Intragastric Balloon (0.7%). The most common type of RYGB derivation, at 67.8% of all interventions, was that initiated at 100 cm from the angle of Treitz with a jejuno-jejunal anastomosis at 150 cm, the 100/200 and 100/250 derivations represented 31.5% and 0.7%, respectively.
No complications were described over the initial 30 days postsurgery for 141 (96.6%) patients. The remaining five patients (3.4%) presented some form of incidence; one patient (0.7%) developed gastrojejunal stricture and four (2.7%) presented infection of the surgical wound. Furthermore, the rate of mortality was 0.7%.
Patient progress in terms of obesity
Before surgery, the mean weight and BMI was 118.77 ± 20 kg and 47.3 ± 7 kg/m2, respectively. At 9 months following surgery, the mean weight was significantly lower at 85.21 ± 16 kg as was the BMI at 31.4 ± 5 kg/m2 (p < 0.001) (Fig. 3); with an overall mean reduction of 33.56 kg, which represents 28.26% of the initial weight. The percentage of excess weight lost was 68.8%, with a greater loss among female patients at both 3 months (41.39 ± 15.75) and 9 months (28.94 ± 13.63) compared to males (40.27 ± 14.33 kg at 3 months and 25.13 ± 16.35 kg at 9 months).
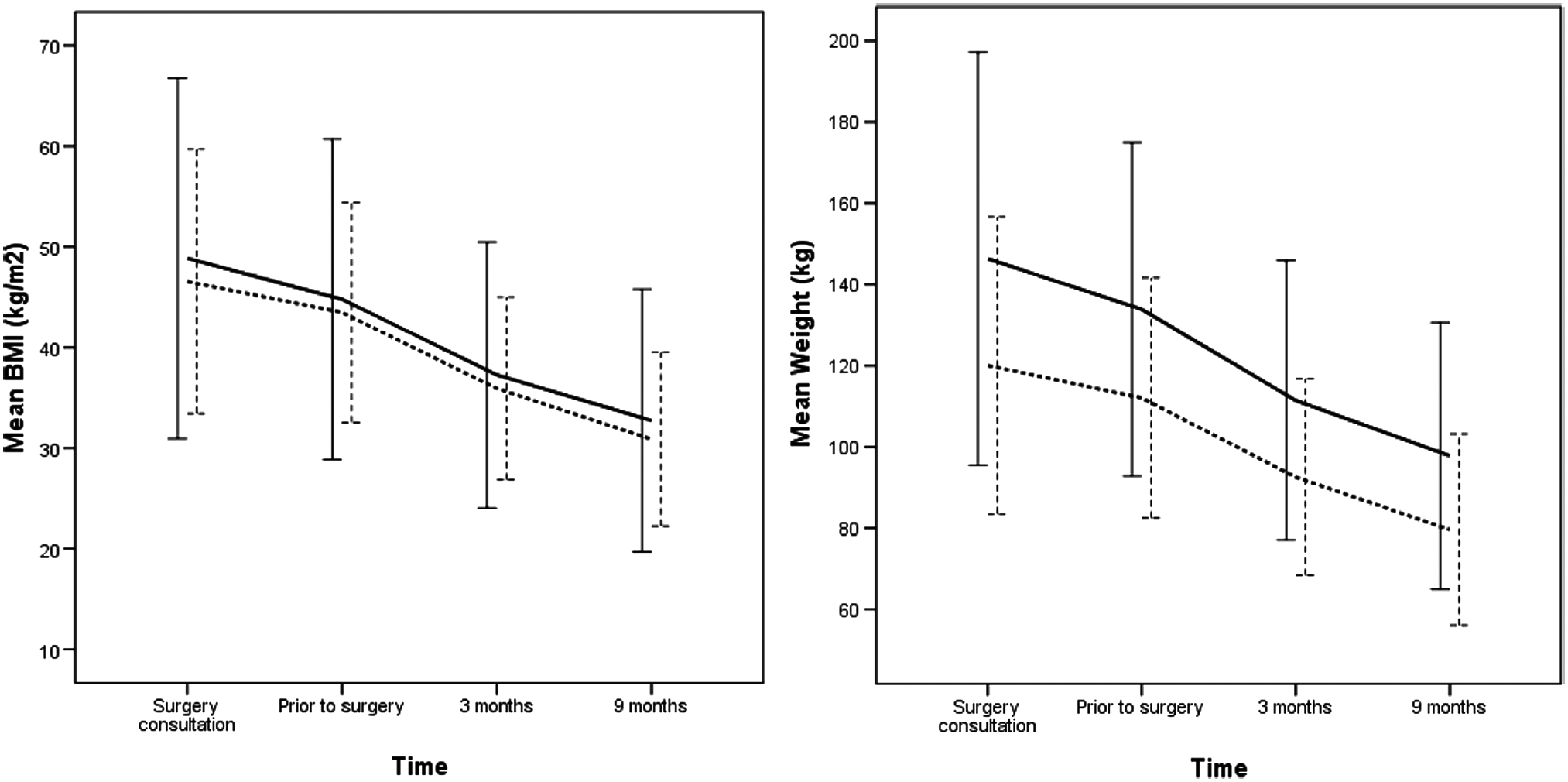
Progress of weight and BMI from the decision to undergo RYGB until 9 months following surgery. Solid line: males; Dashed line: females. Bars = ±2 SD. BMI, body mass index; RYGB, Roux-en-Y Gastric Bypass; SD, standard deviation.
Furthermore, statistically significant differences between measurements are shown for paired comparisons of all possible combinations between follow-up stages, with a decrease in weight and BMI being observed at each consecutive stage (Tables 2 and 3).
M ± SD, mean ± standard deviation.
The partially repeated measures multivariate analysis revealed age [F(2,137) = 1.298; p = 0.276] and gender [F(1,137) = 0.320; p = 0.572] to have no relevance in the efficacy of RYGB surgery. Significant differences are observed solely in weight loss according to the time elapsed since surgery, whereby the greatest weight loss occurred at 9 months [F(1,137) = 390.057; p < 0.001; Eta2 = 0.740].
Patient progress in terms of CVR
Before surgery, the mean CVR estimated at 10 years was 7.64% ± 7.45%, in which 68.5% of patients were classified as having low CVR, 26% as intermediate CVR, and 5.5% as high CVR; whereas 9 months following RYGB, these figures would drop to 0.10% ± 0.77%, thereby situating all patients in the low CVR interval. Furthermore, gender also proved to have a significant effect on CVR [F (1,144) = 24.183; p < 0.001; Eta2 = 0.144] (Fig. 4).
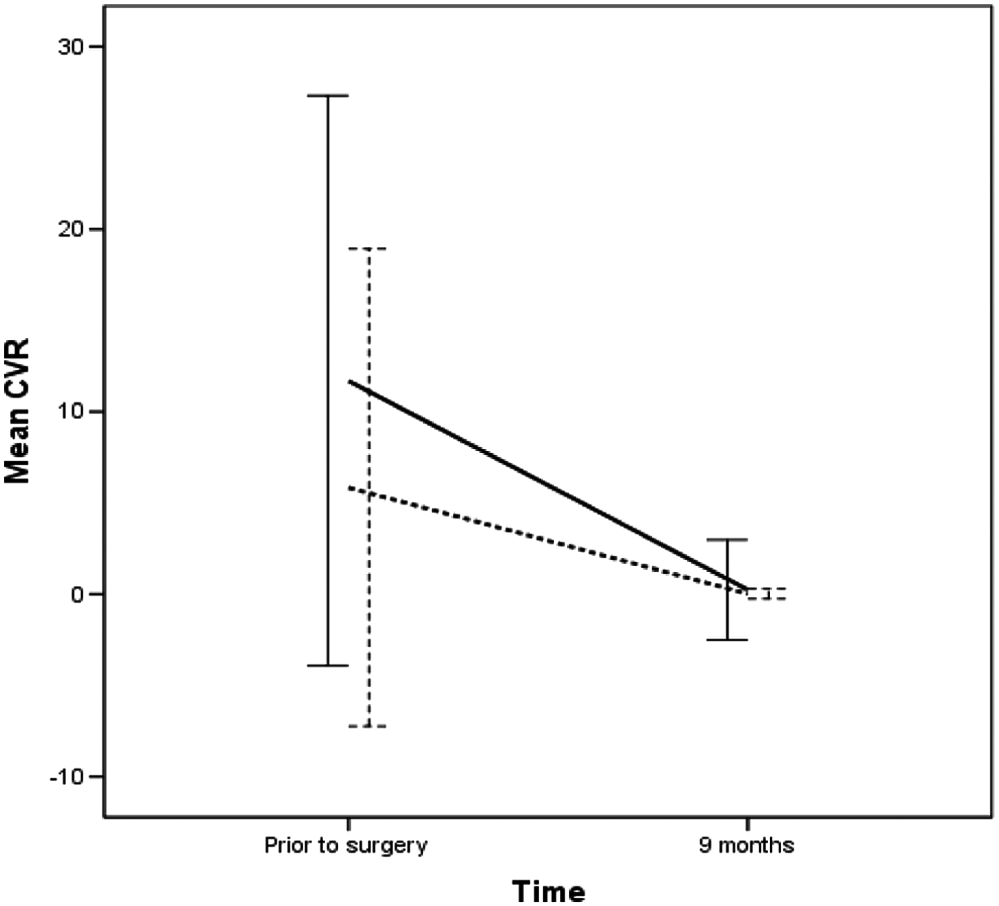
Progress in terms of CVR before and 9 months following surgery for both males and females. Solid line: males; Dashed line: females. Bars = ±2 SD. CVR, cardiovascular risk.
Furthermore, if each CVR factor is assessed separately, it becomes evident that all figures are significantly reduced following this bariatric procedure except for HDL-C, which undergoes an increase in value, all of which is beneficial to patients (Table 4).
TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; DBP, diastolic blood pressure; SBP, systolic blood pressure.
The observed reduction in clinical variables (SBP/DBP) meant that 92.4% of those patients previously diagnosed with high blood pressure had experienced the remission of this condition, with only 6.2% requiring antihypertension medication at the 3-month stage, in contrast with 53.4% before surgery; with the noteworthy result at 9 months, whereby the entire study population had either significantly reduced the use of or no longer required antihypertension medication.
Anthropometric and CVR indicators regarding to Roux-limb lengths
With respect to BMI and weight, a significant interaction between time and RYGB length was observed [BMI: F(3,429) = 28.384; p < 0.001; Eta2 = 0.166; weight: F(3,429) = 28.185; p < 0.001; Eta2 = 0.165]. Patients in 100/200 cm RYGB-length group showed greater BMI and weight, but these differences declined on successive assessments.
However, tests performed with CVR indicators (TC, HDL-C, SBP, and DBP) did not show a significant interaction between time and RYGB length. TC values were similar in both groups [F(1,143) = 2.328; p = 0.129; Eta2 = 0.016]; HDL-C values were greater in patients with 100/150 cm RYGB length [F(1,143) = 6.386; p = 0.013; Eta2 = 0.043]. In respect of blood pressure outcomes, there are no differences between both groups at any time [SBP: F(1,143) = 0.399; p = 0.129; Eta 2 = 0.005; DBP: F(1,143) = 0.940; p = 0.344; Eta2 = 0.007] (Table 5).
Discussion
The inexorable global increase in the incidence of obesity has become a worldwide issue of the highest magnitude. 14 Formally recognized as a Global Epidemic by the World Health Organization 15 in 1997, it has continuously been considered such through to modern day, with more than 2.8 million deaths per year being attributed to this health condition across the globe. 16 Nonetheless, very few publications show the prevalence of clinically critical obesity or MO, despite having been reported as tripling the risk of cardiovascular mortality. 10 The latest studies performed in Spain show an increase of 200% in the prevalence of this level of obesity, 10 with the south of the country highlighted as one of the areas with a higher prevalence. 17 The aforementioned study, carried out in the Region of Murcia, reports figures for MO at 6.4%, which is above those for Spain overall and very similar to those of the USA 11 at 6.6%.
In this context, BS is to be considered a therapeutic option with a potentially far-reaching impact in the treatment of this worldwide epidemic since it has proven to be safe and effective in adult populations, 18 while complying with established safety criteria. 6 Recently, the acceptable limits for the incidence of complications established by safety criteria have been lowered,18,19 nonetheless, the data on levels of incidence reported to date are well below said limits. 20 The incidence of immediate postsurgical complications in this study was 3.4%, mostly due to infection of the surgical wound, with 0.7% being attributable to gastrojejunal stricture, the latter being well below figures published in other studies (4.9%). 21 Furthermore, only one quietus was registered in the immediate postsurgical period, which would suggest that the surgical procedure performed in this study population complies with the established safety criteria 6 , being a much lower proportion than those reported in recent scientific publications.
As the demand for surgery in cases of obesity increases, RYGB prevails as the most common procedure due to its low complication rates and excellent results for obesity and comorbid conditions over the long term.8,9,22 The greater majority of scientific literature on this particular surgical procedure report between 60% and 70% loss of excess body weight, which is equivalent to a mean weight loss of 40 kg. 23 Bretón et al. 24 described a mean weight before surgery of 129.7 kg, which dropped to 83 kg at the 12-month mark, in a sample group with similar sociodemographic characteristics to those of this study group. More recent scientific literature supports these results. 25 If one compares it to this study, a more pronounced weight loss is observed (before surgery: 128.16 ± 23.97 kg; at 3 months: 98.37 ± 16.35 kg; and at 9 months: 85.21 ± 15.71 kg).
In a previous study, 26 the drop in excess weight expressed in percentages at 1 month following RYGB surgery, as well as at 3, 6, and 12 months was 26.4% ± 8.6%, 53.3% ± 6.7%, 75.3% ± 7.9%, and 78.5% ± 8.5% respectively. Similar results can be found in a more recent study, which shows a mean BMI of 29.7 kg/m2 at 12 months following surgery, with an excess weight loss of 78.8% and a weight loss of 35.1%. 27 The results of this study confirm the efficacy of the RYGB surgical procedure observed in previous research articles, with a reduction in excess weight of more than 20 kg at 3 months following surgery and more than 33 kg at the 9-month mark, at which point, the mean BMI had reached 31.45 ± 5.15 kg/m2. These figures translate to a 66.6% weight loss at 9 months and an excess weight loss of 41% at 3 months and almost 69% at 9 months, which would indicate an excellent level of efficacy for this type of surgery in obese patients in this population. Furthermore, the success in weight loss of RYGB has been demonstrated in both men and women. For men, excess weight had been reduced by 65% at 9 months compared to figures before surgery, with the reduction being even greater in women, whose excess weight dropped by 70%. Moreover, the benefits of BS can be observed across all age groups, surpassing other treatments such as physical exercise, which may not be recommendable in older aged persons or those with special physical conditions (physical disabilities, cardiovascular conditions, etc.). The results of this study show a similar level of efficacy for RYGB in young, middle aged, and elderly subjects.
Concerning BS with regard to CVR, Ocon et al. 28 refer to the interaction between obesity, comorbidity, and CVR, stating that the favorable progression in body weight in turn generates a reduction in comorbidity (60.9% vs. 3.6%) at 2 years following RYGB, which consequently produces a drop in CVR (17.3% vs. 1%). A recent publication 29 using the Framingham Test, in which 42 patients (25.92%) were classified as having a CVR >10% at the time of surgery and overall, the estimated CVR dropped significantly from 5.82% ± 7.4% at the onset to 2.21% ± 2.02% (p < 0.001) 2 years following RYGB (p < 0.001), thereby supporting the aforementioned relationship, ratifying current evidence, 30 and taking the headlines in metabolic research. The results of this study are in line with the aforementioned findings in that they show a noteworthy reduction in CVR, for both men and women, whereby all subjects were reclassified to the low CVR group at the 9-month stage.
Conclusion
The RYGB has proven to be a safe and efficacious alternative treatment, which overcomes the limiting factors inherent in human beings wherein other more conservative therapies have reached a cul-de-sac. The incidence of immediate postsurgical complications and quietus comply with safety criteria at proportions below those published recently. The effects of RYGB surgery on BMI and excess body weight in this study were found to be statistically significant with a beneficial reduction in both parameters, regardless of age and/or gender. CVR displayed an identical tendency, whereby the entire study population reached a low-risk classification at the final stage.
Footnotes
Acknowledgments
We wish to express our deepest gratitude to the HCUVA Ethics Committee, Registry and Codification Departments. Thanks to their collaborative efforts this article is now available to readers. This project was sponsored by the Murcia Healthcare Service (Servicio Murciano de Salud).
Authors' Contributions
Concept/design and data analysis/interpretation: V.E.F.-R., D.A.-B., and J.M.X.-G.; Article writing: V.E.F.-R.; and Critical revision and approval of article: J.M., J.A.P.-U., and M.S.-A.
Author Disclosure Statement
No competing financial interests exist.