
Abstract
Introduction:
Obesity is one of the most important risk factors for complications of internal jugular vein (IJV) cannulation. The efficacy and safety of positive end-expiratory pressure (PEEP) are still under debate in obese patients. The aim of this prospective randomized ultrasound study was to investigate effects of different PEEP levels on the cross-sectional area (CSA) of right IJV and overlap with carotid artery (CA) in anesthetized obese patients.
Materials and Methods:
Seventy-two obese patients undergoing various elective surgeries under general endotracheal anesthesia were enrolled. We measured CSA of right IJV, margin of safety (MOS), and degree of overlap between CA and IJV at PEEP 0 (P0), 5 (P5), and 12 (P12) cm H2O levels. We defined a ≥20% increase in CSA as clinically relevant.
Results:
Data were collected for all the 72 patients enrolled in the study. Application of 12, but not 5 cm H2O PEEP, resulted in a clinically significant increase in CSA of right IJV. When compared to P0, application of P5 and P12 increased both degree of overlap (p < 0.001 each) and MOS (p < 0.001 each). None of the patients experienced severe hypotension or bradycardia.
Conclusions:
Application of 12 cm H2O PEEP provides a clinically significant increase in CSA of right IJV without relevant reduction of MOS in anesthetized obese patients.
Introduction
I
Positive end-expiratory pressure (PEEP) is defined as an elevation of transpulmonary pressures at the end of expiration. Application of PEEP is a relatively easy and handoff technique used in anesthetized patients. A small amount of PEEP (4–5 cm H2O) is used in most mechanically ventilated patients during the perioperative period to mitigate end-expiratory alveolar collapse and to increase the functional residual capacity and hence reducing atelectasis. 11 A higher level of PEEP is sometimes used to improve hypoxemia or to reduce ventilator-associated lung injury in intensive care units. 12 PEEP can increase CSA of IJV by 40–76% in anesthetized nonobese patients.13,14 Our systematic search of the National Library of Medicine (PubMed) returned only a brief report of obese patients concerning the effect of PEEP on CSA of IJV authored by Downey et al. 5 They reported a moderate increase in the size of IJV at ≥10 cm H2O PEEP, whereas 25% of patients experienced hypotension. 5 They do not recommend using PEEP ≥10 cm H2O solely to facilitate IJV cannulation in obese patients because of hemodynamic instability experienced. The primary aim of this ultrasound study was to investigate and quantify changes in CSA of right IJV during different PEEP levels in anesthetized obese patients and consequently promote validation of previous results.
Materials and Methods
The protocol of this prospective randomized controlled study was approved by the Institutional Review Board at Selcuk University and written informed consent was obtained from all participants. Obese adult patients (body–mass index [BMI] >30 kg/m2) aged between 18 and 65 years with American Society of Anesthesiologists (ASA) status II–III scheduled for elective surgery under general anesthesia were recruited to the study. Exclusion criteria were as follows: previous IJV cannulation, thrombosis of IJV, anatomical neck abnormalities, uncontrolled hypertension and diabetes, congestive heart failure, valvular heart disease, chronic obstructive pulmonary disease, and pulmonary hypertension. Patients who experienced severe hypotension (mean arterial blood pressure [MAP] of 30% below the baseline value) and bradycardia (heart rate [HR] below 45 beats/min) after induction of anesthesia and/or during the ultrasound measurements were excluded from the study.
In the operating room, all patients received a balanced hydroxyethyl starch solution (HES 130/0.4/6%, Voluven; Fresenius Kabi), 6 mL/kg of the calculated ideal body weight (IBW), over 15 min before induction of anesthesia. 15 Anesthesia was induced with propofol 1.5–2.5 mg/kg of lean body weight (LBW), fentanil 2–3 mcg/kg of LBW, and rocuronium 0.6–1.2 mg/kg of IBW. 16 Anesthesia was maintained with sevoflurane in an air:oxygen mixture (50:50) to keep a target minimum alveolar concentration (MAC) of 0.8 during image recordings and data collection to reduce the risk of hypotension. Lungs were ventilated in a volume-controlled mode with a tidal volume of 7 mL/kg IBW.
All of the measurements were obtained at <20° contralateral neck rotation. The CSA of right IJV was measured at the level of the cricoid cartilage using a two-dimensional ultrasound machine with a 10-MHz linear probe (Mindray M5®). The probe was placed perpendicular to the skin with minimal pressure to ensure that the examined vein was not compressed.
While the probe was held in proper position, an investigator applied three different PEEP levels:
1. A baseline condition without PEEP (P0). 2. A PEEP of 5 cm H2O (P5). 3. A PEEP of 12 cm H2O (P12).
With respect to the order given in randomly assigned sequence.
Randomization was achieved using the Orthogonal Latin Square Design method. 17 Computer-generated randomization codes were prepared and provided to investigators in sequentially numbered sealed opaque envelopes before induction of general anesthesia. Each PEEP condition is administered for 1 min and the ultrasound images were obtained at least 3 s after instituting each maneuver for 10 s. Image capture timing of the study was considered as a washout time. The same practitioner performed all the ultrasound examinations. After getting all images recorded in the ultrasound machine, the following measurements as illustrated in Figure 1 were obtained from those images with usage of preinstalled software by a different examiner who was blinded to the sequence given.

Anatomical illustration of study measurements: a, the depth of the IJV from the skin; b, anteroposterior diameter; c, transverse diameter; d, overlap distance; e, margin of safety; CA, carotid artery; IJV, internal jugular vein; L, left; R, right.
1. CSA of right IJV.
2. Transverse diameter (TD) and anteroposterior diameter (APD) of IJV.
3. Margin of safety (MOS) (defined as the distance from the lateral-most border of IJV and the lateral-most border of carotid artery (CA) at which IJV could be punctured without touching CA). 18
4. Depth of IJV from skin (DS, measured by drawing a line between skin and the closest margin of the vein to skin's surface).
5. Degree of overlap (categorized on the basis of percentage overlap of IJV with CA) no overlap (0%), less than 25%, between 25% and 50%, greater than 50%. 18
Intraoperative hemodynamics (HR, MAP) were monitored during the experiment. Hypotension was defined in this study as a 30% decrease in MAP with respect to baseline value, and upon occurrence, patients were to be treated immediately with 5 mg of ephedrine. Atropine (0.5 mg) was injected when HR decreases to less than 45 beats/min (bradycardia). The use of vasoactive drugs was recorded along with patients' blood pressure and HR.
The primary outcome was CSA of right IJV. We defined an increase in right IJV's CSA ≥20% as being clinically relevant and patients with an increase ≥20% as “responders,” while patients with an increase <20% as “nonresponders.” 19 The secondary outcomes were TD, APD, MOS, DS, and degree of overlap. We calculated that a sample size of 72 patients is necessary to detect a difference in CSA of right IJV following application of different PEEP levels with 80% power at a 0.05 significance level based on the results of a similar previous study. 5
Demographic characteristics of patients were evaluated by T-tests or chi-square tests. Mixed models are formed using SAS software 9.1 (SAS Institute) and SPSS version 21 (SPSS) to investigate effects of PEEP (taken both continuous and categorical) on outcomes. When the PEEP effect is significant, multiple comparisons were done by using the Tukey–Kramer adjustment. The association between degree of overlap ordinal variable and categorical PEEP variable is investigated using a Mantel–Haenszel test for trend. A p-value <0.05 was considered to be statistically significant.
Results
Complete data and images for analysis were obtained from 72 patients. Patient characteristics are presented in Table 1. Enrolled patients varied in age from 21 to 65 years, with a mean ± standard deviation (SD) of 42.93 ± 11.06 years. BMI values with mean ± SD of 37.34 ± 6.11 ranging from 30.5 to 60.2 were similar between male and female patients (p = 0.64). Seventeen patients (23.6%) had baseline hypertension with no significantly different BMI values 36.0 ± 4.04 and baseline CSA 1.07 ± 0.35 when compared to 55 normotensive patients BMI 37.76 ± 6.59 and baseline CSA 1.06 ± 0.38 (p = 0.302 and p = 0.905, respectively). Mixed models showed a significant effect of PEEP on all outcomes except DS (p = 0.01 for MOS, p = 0.34 for DS, and p < 0.001 for TD, APD, and MOS). A one unit increase in PEEP caused an average 0.021 unit increase in CSA of IJV confidence interval (CI) = 0.20–0.23, 0.009 unit increase in APD CI = 0.08–0.10, 0.013 unit increase in TD CI = 0.012–0.015, 0.007 unit decrease in DS CI = −0.009 to −0.005, and 0.006 unit increase in MOS CI = 0.003–0.009. Figure 2 shows boxplots of unadjusted CSA values of right IJV measured at different PEEP sequences.
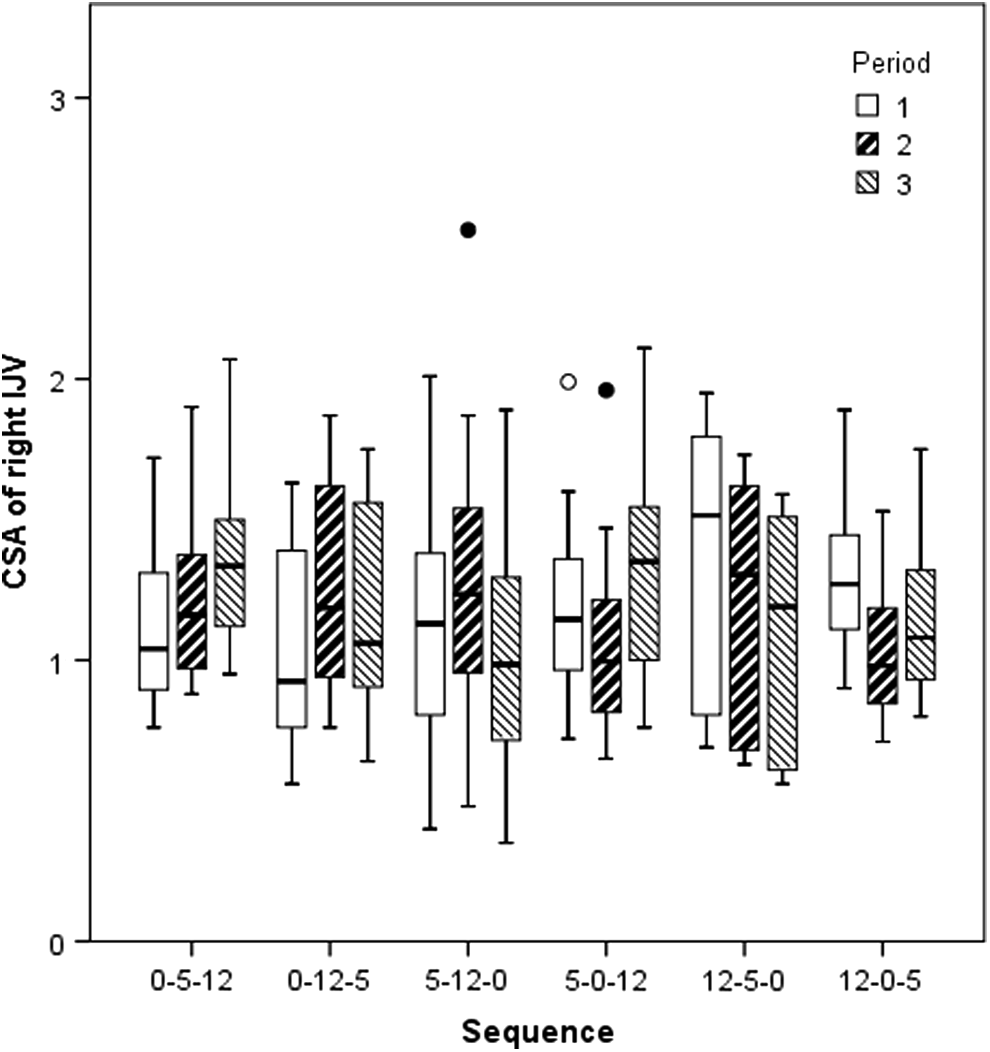
Boxplots of unadjusted CSA values of right IJV at different PEEP sequences.
Age is given as mean ± standard deviation. ASA status and BMI are given as frequencies and percentages.
ASA, American Society of Anesthesiologists; BMI, body–mass index.
Unadjusted means of outcome measurements and percentage changes with respect to P0 level are presented in Table 2, including degree of overlap. Even though mean CSA was significantly increased by each PEEP level when compared to P0 (p < 0.001 each by a mixed model with categorical PEEP variable), increments at P5 level were not clinically relevant (10.5%). No complications developed and no examinations had to be terminated because of hypotensive and bradycardic events. The hemodynamic measurements (HR and MAP) during the elevated PEEP levels are displayed in Table 2. When compared to P0, application of P5 and P12 increased both percentage of overlap (p < 0.001 each) and MOS (p = 0.032 for P5 and p = 0.003 for P12).
Data are given as means ± standard deviations except overlap. Degree of overlap is given as frequencies and percentages. Percentage increases are calculated with respect to P0 levels.
Indicates p < 0.05 when compared to P0 level.
APD, anteroposterior diameter; CSA, cross-sectional area; DS, depth of IJV from skin; HR, heart rate; MAP, mean arterial blood pressure; MOS, margin of safety; PEEP, positive end-expiratory pressure; TD, transverse diameter.
The Mantel–Haenszel test for trend showed that PEEP and degree of overlap are positively associated (p = 0.01). As shown in Table 3, there were no differences in age, sex, BMI, ASA status, and baseline measurements of CSA, TD, APD, DS, and MOS between responders and nonresponders.
Data are given as means ± standard deviations. Male and ASA grades are given as frequencies and percentages.
None of the characteristics is statistically different across two groups except transverse diameter where p = 0.032.
Discussion
The present study demonstrated that both 5 and 12 cm H2O PEEP levels significantly increase CSA of right IJV when compared to 0 cm H2O PEEP. We found that percentage overlap of CA with IJV increases when PEEP is increased. Beside these, MOS also increases at 5 and 12 cm H2O PEEP, compared to 0 cm H2O PEEP.
In obese patients, placement of a CVC may be challenging due to hidden anatomical neck landmarks. Obese patients have large neck circumferences, short thick necks that may obscure anatomic landmarks such as the trachea, CA pulsation, and margins of the sternocleidomastoid muscle. Because of increased tissue mass between skin and IJV, the depth of needle insertion may be extended and the insertion angle may be too steep. In addition to these handicaps, it was reported that anatomic variations in the position of right IJV were more frequent in morbidly obese patients than the general adult population. 3 There have been several reports about possible complications of CVC in obese patients. Brusasco et al. studied the efficacy and safety of ultrasound-guided CVC in 55 severely morbid obese patients. 3 They concluded that the success of catheter positioning on the first attempt was related to the vein's major diameter but not to other anatomical characteristics such as BMI, neck circumference, neck height, and vein depth. 3 Thus, increasing diameter of IJV promotes success of cannulation.3,10
There are several studies investigating the effects of various dynamic maneuvers such as the Trendelenburg position, hepatic compression, leg elevation, and Valsalva maneuver on CSA of IJV.10,13,20 The Trendelenburg position and Valsalva maneuver are found effective on increasing CSA of IJV by many authors.10,13 However, the patient populations in these studies are not specifically obese, rather a general population was recruited. Application of PEEP in anesthetized patients is an easy and handoff technique associated with an increase in intrathoracic and right atrial pressure, leading to a rise of mean central venous pressure, and as a consequence, enlarging CSA of IJV. Hollenbeck et al. concluded that application of a 10 cm H2O PEEP increases CSA of IJV to an extent similar to the aforementioned maneuvers such as Trendelenburg position and Valsalva in patients under general anesthesia. 13
A study in anesthetized obese patients by Downey et al. conducted to quantify the effect of different PEEP levels (5 and 10 cm H20) on CSA of IJV showed that PEEP modestly increases the size of IJV but was poorly tolerated due to hypotension.
5
They reported that a 5 cm H2O increase in PEEP enlarges CSA by 0.16 ± 0.02 cm2. Our findings showed that both PEEP at 5 and 12 cm H2O result in significant increases in CSA of right IJV by 0.11 ± 0.05 and 0.26 ± 0.10 cm2, respectively, where only application of P12 passed the clinically relevant degree (24.5%). Similar to this result, Downey et al. reported an approximate 25% increase in CSA of IJV at PEEP 10 cm H2O.
5
However, despite this relevant increase in size of vein, they do not recommend using PEEP ≥10 cm H2O solely to facilitate IJV cannulation in obese patients because of arterial hypotension observed in six patients (25%). However, in our study, we did not observe hypotension probably due to the following precautions taken:
(a) We used preoperative preloading to prevent circulatory depression because in recent studies on fasted morbidly obese patients, it is reported that intravascular volume loading before anesthesia induction prevented hemodynamic disturbance even with high PEEP application.15,21 (b) Through application of increased levels of PEEP, additive effect on blood pressure should be kept in mind. We have ruled out this additive hypotensive effect by using a randomized crossover design.17,22 (c) Anesthesia was maintained with sevoflurane to keep a target MAC 0.8 and the capture time of images was taken shorter to prevent long time exposure to inhalational anesthetic agents without surgical stimulation being another cause of hypotension.
Marcus et al. studied the degree of increase in CSA of IJV on 50 obese and nonobese ASA III surgical patients following application of different PEEP levels (5 and 10 cm H2O) in combination with the Trendelenburg position. 19 They defined patients with an increase <20% in CSA as “nonresponders” and found that mean CSA significantly increases by each maneuver, while 13 of 50 patients were nonresponders. These nonresponders did not differ in age, height, or hemodynamic variables, but in body weight and BMI. In our study at 5 cm H2O PEEP level, no patients were responders, whereas at 12 cm H2O PEEP level, 55 of 72 patients (76.3%) were responders.
Our study demonstrates that overlap between IJV and CA significantly increases as PEEP is increased from 0 to 5 cm H2O and 0 to 12 cm H2O, which may in turn be linked to a higher risk of accidental puncture of CA. However, our data show that application of increased PEEP levels increases MOS. Since MOS also increases in conjunction with degree of overlap, the risk of accidental puncture reduces and the linkage of increasing overlap to high risk of accidental CA puncture was diminished. The positive relationship we have found between MOS and PEEP maneuver in obese patients has not yet been documented elsewhere in the literature as to our knowledge.
There are some limitations in the current study. We did not examine the real success of IJV cannulation. This needs further confirmation especially in cases when an ultrasound machine is not available. Morbidly obese patients often have significant cardiopulmonary changes that affect the pulmonary and cardiovascular system. 23 Further studies will be required to investigate the effects of PEEP in critically ill obese patients who may be in more need of a CVC.
Conclusions
In conclusion, application of 12, but not 5 cm H2O PEEP, provides a clinically significant increase in CSA of right IJV and leads to increase in degree of overlap without relevant reduction of MOS in anesthetized obese patients. The results suggest improved safety of IJV catheterization without an increased risk of CA puncture and hypotension in obese patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.