
Abstract
Background:
Laparoscopic sleeve gastrectomy has become one of the most effective treatment options for adults with severe obesity. However, optimal anesthetic management for laparoscopic sleeve gastrectomy has not been described yet.
Methods:
In this prospective randomized study, we compared the effects of propofol anesthesia (Group 1) with desflurane anesthesia (Group II) in morbid obese patients for laparoscopic sleeve gastrectomy. We compared postoperative recovery and hemodynamic parameters of the patients. We also investigated the changes in tracheal cuff pressure and peak airway pressure of these obese patients during orogastric tube insertion and peritoneal CO2 insufflation.
Results:
Eye opening and extubation time were longer in the propofol group than in the desflurane group (p < 0.05). No statistical difference was found between the two groups with respect to recovery scores (p > 0.05). Six patients in Group I and eight patients in Group II had sore throat (p > 0.05). Eight patients in Group I and 12 patients in Group II had postoperative nausea. Only one patient had vomiting in Group I. Peak airway pressure and tracheal cuff pressure of the patients in both of the groups showed gradual increase in values during peritoneal insufflation and after orogastric tube insertion compared with the values at intubation during the procedure (p < 0.05).
Introduction
M
Anesthetic management of obese patients needs appropriate care and preventive measures because the risk of intraoperative complications such as hypoxemia (difficult ventilation and intubation) and postoperative major complications such as myocardial ischemia are observed more in obese adult patients than in nonobese patients.3,4 Fast induction, management of the airway, perioperative hemodynamic stability, and fast recovery are important.
Bariatric surgery has become an important treatment method for these patients with morbid obesity. The surgical method has changed from Roux-en-Y to sleeve gastrectomy with comparable results in adults. Previous reports reported that orogastric tube insertion during laparoscopic sleeve gastrectomy has a potential effect on tracheal cuff pressure. 5 Also peritoneal insufflation results in numerous cardiovascular, neuroendocrine, and renal changes. 6
Different anesthetic techniques have been recommended but there is no study showing superiority of one technique to another. Propofol is one of the most commonly used intravenous anesthetic agents in ambulatory procedures that provides fast induction. 7 Desflurane could be advantageous in obese patients because of its low solubility. 8 The aim of this study was to compare the postoperative recovery scores, tracheal cuff pressure, peak airway pressure, and hemodynamic parameters of 61 morbid obese patients randomized to receive propofol infusion or desflurane in combination with remifentanil to maintain anesthesia for laparoscopic sleeve gastrectomy.
Materials and Methods
After obtaining local ethics committee approval of Kecioren Training and Research Hospital and written informed consents of all participants, 61 American Society of Anesthesiologists (ASA) I–II morbidly obese patients (body mass index [BMI] >35 kg/m2) scheduled for laparoscopic sleeve gastrectomy were recruited in this prospective randomized study. All operations were performed by the same surgeon. Patients were randomized using a closed envelope method to one of two equal groups (Group I, propofol, or Group II, desflurane). On the day before each surgery, preoperative anesthesiological assesment was performed. Exclusion criteria of the study were patient refusal, severe cardiopulmonary disease, chronic alcohol or drug abuse, significant renal disfunction (serum creatinin >2 mg/dL), liver disfunction, chronic obstructive lung disease, allergy to an anesthetic, and psychiatric or neurological disorders. Antihypertensive medications (ACEI, ARB, and beta-blockers) were given to the patients at the morning of surgery.
When the patient arrived at the operating ward, standard monitoring was applied with a five-lead electrocardiogram, noninvasive blood pressure, pulse oximetry, and capnometry. All anesthetic drugs during the procedure were administered by using the empirical formula of corrected body weight or ideal body weight (corrected body weight [CBW] = ideal body weight [IBW]+[0.4 × excess weight]). After preoxygenation through 100% oxygen (2 min) by face mask, general anesthesia was induced with intravenous (IV) injection of propofol 2 mg·kg−1 CBW, and followed by fentanyl 1 mg·kg−1 IBW. Rocuronium 0.6 mg·kg−1 IBW was used to facilitate orotracheal intubation. After intubation, ventilation with a mixture of air–oxygen (50/50%) was delivered through a semiclosed circuit with a fresh gas flow of 3 L/min. Ventilator settings were 8 mL/kg tidal volume (IBW) and 10 cmH2O positive end expiratory pressure for all of the patients. Endotracheal intubation was performed by an experienced anesthesiologist using high-volume endotracheal tubes (Rusch, Kamunting, Malaysia) with internal diameters of 8.0 mm for men and 7.5 mm for women. After successful intubation, the pilot balloon of the tube cuff was inflated by the anesthesiologist and the cuff pressure was adjusted to range between 25 and 30 mmHg by using a cuff pressure manometer (Mallinckrodt, Athlone, Ireland). End tidal carbon dioxide (EtCO2) pressure was maintained between 35–45 mmHg. Intraoperative crystalloid infusion was administered at 7 mL/kg. Neuromuscular function was evaluated using a TOF monitor (TOF-Watch SX; Organon LTD., Dublin, Ireland) and neuromuscular blockade was maintained by keeping the train of four below two with additional rocuronium boluses. Patients were randomly divided into two groups: Group I (n = 31) received propofol and Group II (n = 30) received desflurane for the maintanence of anesthesia. In the propofol group, general anesthesia was maintained with a gradually reduced continuous IV infusion of propofol (21 mg·kg−1 CBW for 5 min, 12 mg·kg−1 CBW for 10 min, and then 6 mg·kg−1 CBW). Remifentanyl infusion was administered at 0.1–1 μ/kg·min in both of the groups. Bispectral index (BIS) monitoring (BIS VISTA, Aspect Medical Systems) was used to provide adequate depth of anesthesia during the maintenance of general anesthesia. Propofol and desflurane administrations were titrated to maintain the BIS level between 45 and 55.
Pneumoperitoneum pressure was maintained at 13–14 mmHg in all of the patients. Tracheal cuff pressure and peak airway pressure of the patients were measured at predefined points throughout the perioperative period: during intubation, before peritoneal insufflation, 5–10–15 min after onset of the pneumoperitoneum, at orogastric tube insertion (36F), after extraction of the orogastric tube, and before extubation. Pressure level more than 30 cmH2O was adjusted back to 25–30 cmH2O during the perioperative period.
During the last 10 min, the inhalational agent desflurane decreased to 0.5 minimum alveolar concentration and propofol infusion decreased to 3 mg·kg−1. Tramadol 1 mg·kg−1 and dexketoprofen (Arveles®) 50 mg IV were used for postoperative analgesia. Upon completion of surgical skin closure, the fresh gas flow rate was increased to 6 L/min on 100% oxygen and neuromuscular blockade was reversed with neostigmine (0.07 mg·kg−1) and atropine (0.01 mg·kg−1). All patients were extubated when they were able to sustain spontaneous ventilation with a tidal volume greater than 5 mL/kg, train of four ratio higher than 0.9, and response to verbal commands. The time from discontinuation of the study drug to eye opening and extubation was recorded by a blinded study person. We have used Aldrete scores to determine the recovery of anesthesia at post-anesthesia care unit (PACU) admission and at 5 min interval until patients achieve an Aldrete score higher than 8 for PACU discharge. Hemodynamic parameters were recorded at predefined points throughout the perioperative period: preoperatively, during intubation, 10–15 min after onset of the pneumoperitoneum, at orogastric tube insertion (36F), and after extraction of the orogastric tube. The decrease in systolic blood pressure (SBP) <15% of the baseline was treated with reducing the continuous infusion rate of remifentanyl. Ephedrine was used for decreased SBP (∼25% change from baseline) and atropine was used for decreased heart rate (<45/min). Society for Ambulatory Anesthesia for Postoperative nausea and vomiting (SAMBA PONV) risk (0–4 points) of the patients was recorded during the procedure. Risk factor scores for PONV are defined as female gender, nonsmoker, history of PONV, and usage of postoperative opioids. Basic PONV risk if no risk factors are present is 10%. Risk increases to 20%, 40%, 60%, and 80% for each additional risk factor. Sore throat of the patients was recorded as none, mild, moderate, or severe.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0. We expressed the data as mean, standard deviations, or percentage. For all continuous variables, Kolmogorov Smirnov test was used for normal distribution. Between groups, continuous variables were analyzed using independent samples t-test or Mann–Whitney U test. Chi square test or Fisher's exact test was used for categorical variables between groups. Intragroup comparisons were done using Friedman test or repeated measures ANOVA. Wilcoxan with a Bonferroni correction or Bonferroni test was used as a post hoc test. p Values <0.05 were considered statistically significant. Based on preliminary data that measured emergence time in morbidly obese patients, an a priori power analysis indicated a sample size of 20 per group would be sufficient to detect a 30% or greater decrease in time to emergence end points with a power of 0.8 (α = 0.05).
Results
A total of 61 patients were recruited into the study. One ASA II asthmatic patient in the desflurane group developed bronchospasm, requiring sedation and mechanical ventilation during extubation and was transferred to the intensive care unit. The data of this patient were excluded from the study. Table 1 presents the demographic and intraoperative data of the patients. No differences were found in demographic data (age, height, BMI, and sex), duration of anesthesia, and duration of surgery between the groups. There was no difference between groups with respect to preoperative and intraoperative SBP and mean arterial blood pressure (Table 1). Seven patients (22%) in Group I and six patients in Group II (20%) were treated with ephedrine (p = 0.806). Intraoperative crystalloid infusion was administered at 7 mL/kg. Fluid boluses were not used in this study. A decrease in SBP was treated with reducing the infusion of remifentanil. Five patients in Group I and four patients in Group II needed dose reduction. Heart rate (beats per min), ETCO2, and SPO2 were similar between the two groups (p > 0.05). The times from the end of the operation to eye opening (desflurane, 3.6 ± 1.03 min; propofol, 6.19 ± 3.62 min) and extubation (desflurane, 3.16 ± 1.26 min; propofol, 6.06 ± 3.18) were significantly shorter in the desflurane group than in the propofol group (p < 0.05). We have used Aldrete scores for determining the recovery from anesthesia at admission to PACU and 5, 10, 20 min after the completion of the procedure. The results of PACU scores were similar in the two groups (Table 2). No differences were found with respect to SAMBA PONV risk score (Group I, 2.03 ± 1.14; Group II, 2.13 ± 1.53) between the two groups (p = 0.806). Eight patients in Group I and 12 patients in Group II had postoperative nausea. Only one patient had vomiting in Group I. Six patients in Group I and eight patients in Group II had sore throat (p > 0.05). All of the patients had mild sore throat scores except for two patients in Group II who had moderate sore throat scores.
Data are expressed as mean ± SD.
Mann–Whitney U test and t-test were used.
SBP, systolic blood pressure; MAP, mean arterial pressure.
Data are expressed as mean ± standard deviation.
PACU, post-anesthesia care unit.
Tracheal cuff pressure and peak airway pressure of the patients were increased at 5, 10, and 15 min of peritoneal CO2 insufflation and during orogastric tube insertion compared with the values measured at intubation in both of the groups (p < 0.05). The increase in tracheal and peak airway pressure of the patients was similar in both of the groups. Tracheal and peak airway pressure of Group I did not increase faster or more than that of Group II. No intervention was required in both of the groups. Figure 1 presents the changes in tracheal cuff pressure and Figure 2 presents the changes in peak airway pressure in both of the groups.
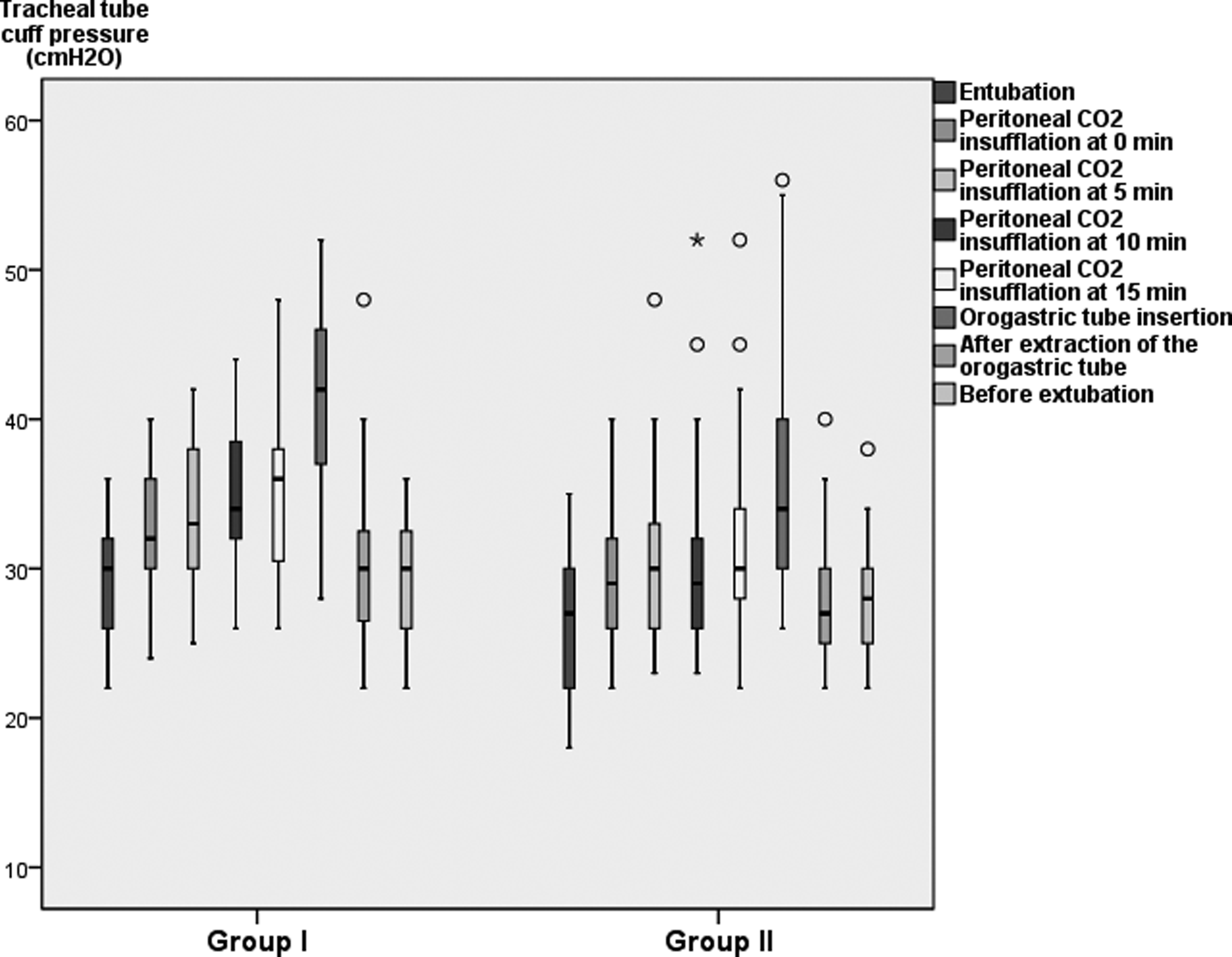
Tracheal cuff pressure of patients in both the groups. Tracheal cuff pressure (cmH2O) = (10–60 cmH2O).
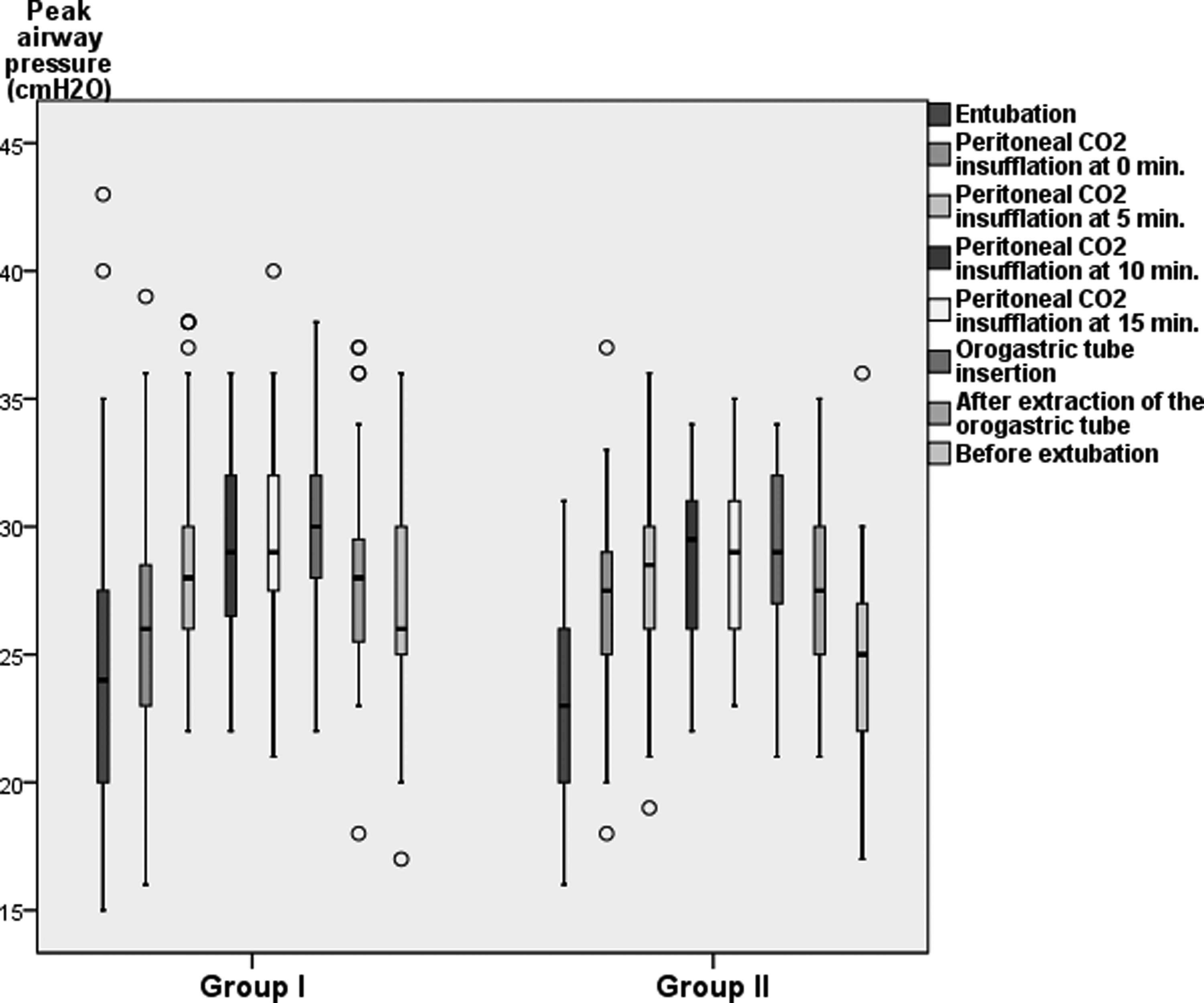
Peak airway pressure of patients in both the groups. Peak airway pressure (cmH2O) = (15–45 cmH2O).
Discussion
Morbid obese patients are at increased risk for perioperative pulmonary complications, deep venous thrombosis, and pulmonary embolism.9,10 Also, carbon dioxide pneumoperitoneum can adversely affect respiratory mechanics by causing hypercarbia and elevated intraabdominal pressure. In this study, we investigated the differences in postoperative recovery after desflurane and propofol anesthesia combined with remifentanil in morbidly obese patients undergoing laparoscopic sleeve gastrectomy. We also evaluated tracheal and peak airway pressure of the patients during the procedure in both of the groups.
Desflurane has a low solubility. For this reason, the partial pressure of this agent in blood and tissues reaches the inspired partial pressure more rapidly than the blood and tissue pressures of other potent volatile agents. Also, desflurane resists biodegradation in humans and has a little or no toxic potential. 11 Propofol is one of the most commonly used anesthetic agents that provides fast induction and decreased prevalance of postoperative nausea and vomiting. 7 However, prolonged emergence time from anesthesia was observed in obese adults undergoing clinically titrated propofol total intravenous anesthesia (TIVA) without BIS monitoring, because of propofol accumulation and slow washout.12,13
In recent studies, desflurane has been suggested as an effective option for obese patients by providing faster recovery than sevoflurane when used without premedication. 8 Strum et al. compared postoperative recovery and emergence of desflurane with those of sevoflurane in morbid obese adult surgical patients. The patients in the desflurane group showed significantly early recovery of response to commands and required shorter tracheal extubation time than patients in the sevoflurane group. 14 In contrast to these studies, Vallejo et al. found no differences in emergence and recovery parameters of the morbid obese patients receiving desflurane or sevoflurane for laparoscopic gastroplasty. They explained that the difference in emerge time between desflurane and sevoflurane becomes minimal when the concentration at the time the volatile agent is turned off is ≤80% of the maintenance dose. For this reason, they have decreased the MAC of the volatile agent to 0.5 MAC at the beginning of the surgical closure. 15
Total intravenous anesthesia applied with propofol provides rapid recovery and a lower incidence of postoperative nausea and vomiting. 7 Salihoglu et al. found no significant difference between TIVA and sevoflurane anesthesia in bariatric surgery. 16 Siampalioti et al. found that patients who were given sevoflurane required shorter recovery time and better hemodynamic stability than patients given propofol. 17 Juvin et al. compared postoperative recovery of the morbid obese patients after desflurane, propofol, or isoflurane anesthesia. They have used inhaled nitrous oxide, alfentanil, and the study drug for the maintanence of anesthesia, and they have found that desflurane provided rapid immediate postoperative recovery than propofol and isoflurane. 18
There are only a limited number of studies comparing the effects of propofol with those of the other anesthetic agents in morbidly obese patients, only Juvin et al. and our study compared propofol and desflurane anesthesia among morbidly obese patients undergoing bariatric surgery. In this study, we did not use inhaled nitrous oxide. We used remifentanil for the maintanence of anesthesia. During the last 10 min of the operation, the inhalational agent desflurane was decreased to 0.5 MAC and propofol infusion was decreased to 3 mg·kg−1. Similar to the study of Juvin et al., the time from the end of operation to eye opening and time to tracheal extubation were found shorter in the desflurane group than in the propofol group. However, the Aldrete scores were found similar in both of the groups.
It was shown that CO2 pneumoperitoneum and trendelenburg position used during laparoscopic surgery affect the intrathoracic pressure by approaching the diaphragm upward. 6 Also, peak inspiratory pressure and mean airway pressures increase. 19 Yıldırım ZB et al. showed that the cuff pressure of the endotracheal tube progressively increased during pneumoperitoneum with the increase in intraabdominal pressure caused by carbon dioxide insufflation. Tracheal cuff pressure of the patients was increased from 29 to 35 cmH2O at the beginning of CO2 pneumoperitoneum (maximum intraabdominal pressure was set at 14 mmHg). Patients requiring gastric tube insertion were not included in this study. 20 The insertion of an orogastric tube is a routine procedure in a sleeve gastrectomy to facilitate gastric pouch formation. However, this procedure may increase the tracheal tube pressure and cause laryngotracheal complications and esophageal perforation.5,21 In this study, we did not use inhaled nitrous oxide because of it has diffusing effect on the endotracheal tube cuff. In our study, tracheal cuff pressure and peak airway pressure of the patients were progressively increased during peritoneal CO2 insufflation and highest levels were obtained during orogastric tube insertion compared with the values measured at entubation in both the groups. The tracheal cuff pressure returned to the levels measured at entubation after orogastric tube extraction. Despite the previously reported antiemetic effect of propofol, 22 postoperative nausea and vomiting incidences were found similar in both the groups in this study. The incidence of sorethroat was similar for the two groups. Six patients in Group I and eight patients in Group II had sore throat. All of the patients had mild sore throat scores except for two patients in Group II who had moderate sore throat scores. The endotracheal cuff pressure level more than 30 cmH2O was adjusted back to 25–30 cmH2O during the perioperative period and this can explain why only few patients had mild sore throat.
In our study, emergence of the morbid obese patients as measured by the time to eye opening and the time to extubation was found shorter with desflurane than with propofol anesthesia. In conclusion, desflurane anesthesia with the measurement of endotracheal cuff pressure can provide rapid recovery and minimize the possibility of tracheal injury.
Footnotes
Author Disclosure Statement
No competing financial interests exist.