
Abstract
Objective:
This study was conducted to analyze if bariatric surgery interventions can induce changes in quality of life (QoL) perception of obese people and to compare the outcomes of two different kinds of bariatric surgery interventions.
Methods:
A before–after study on a cohort of obese patients who were subjected to bariatric surgery in the years 2013–2015 was conducted. QoL using the Laval Questionnaire, a tool specifically created for the evaluation of QoL on obese people waiting for surgery, was assessed.
Results:
One hundred sixty subjects were enrolled in the final sample (62 for gastric bypass vs. 98 for adjustable gastric banding [GB]). Incremental improvements in QoL have occurred in the third month after surgery, with a contextual progressive weight loss. Subjects who underwent gastric bypass experienced greater improvements in QoL and a more important weight loss than patients who were subjected to adjustable GB.
Conclusions:
After 12 months, general QoL shows an improvement and an important weight loss occurs in many patients; hopefully, these results will be sustained in a longer period. Bariatric surgery could be an important solution for the improvement of QoL in obese people.
Background
O
Obesity is a complex and multifactorial condition that can be related to emotional, environmental, and genetic causes.2–4 It is defined by the presence of a body mass index (BMI) greater than 30 kg/m2. When BMI exceeds 40 kg/m2, the condition is defined like morbid obesity and it is associated with the increase of several physical health problems, including cardiovascular diseases, type 2 diabetes, dyslipidemia, osteoarthritis, cancer (including colon, breast, prostate, and endometrium cancer),2,3,5 skin deterioration, and movement difficulties. 2 Breathlessness and dyspnea are common symptoms in obese people 6 along with obstructive sleep apnea and respiratory failure.2,7 Obesity also represents a risk factor for urinary incontinence, 8 metabolic syndrome, 2 and female infertility. 5 The risk of death, especially in people affected by morbid obesity, is increased from 50 up to 100%7,9,10 and life expectation may be reduced till 10–15 years if compared with the nonbariatric population. 11
Morbid obesity is often complicated by the presence of depression, which compromises quality of life (QoL).7,12 The decrease in health-related QoL perception is especially evident in obese patients who try to undergo surgical treatments to lose weight.13,14 Bariatric surgery is aimed at improving QoL in people affected by obesity as well as at reducing mortality and medical risk factors. 15
The purpose of this study is to analyze how much bariatric surgery interventions can induce changes in QoL perceptions in a sample of subjects with morbid obesity, simultaneously comparing the outcomes of two different types of bariatric surgery interventions (Roux-en-Y gastric bypass vs. adjustable gastric banding [GB]).
Materials and Methods
This multicenter before–after study was conducted in the period 2013–2015 at the “Fondazione IRCCS Ospedale Maggiore Policlinico of Milan” and at the “Casa di Cura San Pio X in Milan,” two Italian bariatric surgery centers. In the observational study, we included patients aged between 19 and 65 years with morbid obesity and BMI ≥35 kg/m2, who were candidates for bariatric surgery (GB or gastric bypass) in accordance with the international guidelines and who were waiting for interventions. The presence of comorbidity was not considered as an exclusion criterion for participation in the study. Instead, patients with impaired cognitive status, people who were not candidates for bariatric surgery, or patients who did not accept to provide the verbal informed consent were all excluded.
The recruitment of patients for the study was carried out during the first visit with the bariatric surgeon, when the first administration of a specific tool took place.
To assess QoL in this cohort of obese patients, we used the Italian Laval Questionnaire, originally developed in Canada and written in French. This tool is specifically developed for the assessment of QoL of obese people waiting for or subjected to bariatric surgery. It includes 44 items divided into six domains: symptoms, activity/mobility, personal hygiene/clothing, emotions, social interaction, and sexual life. Each domain is scored on a seven-point Likert scale. Total value of HRQoL can be between 6 and 42, higher scores meaning a better QoL. Patients are asked to indicate how their obesity has affected their lives in the last 4 weeks. The administration takes about 10 min on average. 7 In this study, we used the Italian version created on the basis of a process of back-translation.
The assessment of QoL with the Laval Questionnaire was done at time 0 (before the intervention) and at times 1, 2, 3 and 4 (1, 3, 6, and 12 months after the intervention).
The study was conducted according to the principles contained in the Declaration of Helsinki and after approval of the local ethics committee.
Statistical analysis
We used methods of descriptive statistics to describe sample features. Linear regression after Blom's transformation was undertaken to describe data, to explain the relationship between dependent and independent variables, and to make comparisons between the two groups (gastric bypass and adjustable GB); in case of failure of the inverse normal transformation, the Wilcoxon's signed-rank test for matched pairs was used. Statistical analysis was conducted with STATA 11.2 for Windows (Copyright © 1985–2009 StataCorp LP Statistics/Data Analysis StataCorp College Station, TX). A statistician reviewed the analysis and checked the results.
Results
One hundred sixty-six patients were enrolled in the study, according to the inclusion criteria. Six of them were ongoing excluded because of some complications that led to the impossibility to perform the intervention or because they refused surgery. According to the guidelines, 62 subjects underwent gastric bypass and 98 underwent adjustable GB.
Our sample comprised 34 males and 126 females aged 43 ± 11 years (95% confidence interval, 41–45). Most patients were Italian (n = 149). One patient was illiterate, 8 had primary school license, 61 had secondary school license, 76 had high school degree, and 20 were university graduates. At time 0, patients who were waiting for gastric bypass intervention (BY) had a higher weight than people waiting for GB (BY: 135.33 ± 12.05 kg vs. GB: 107.70 ± 19.50 kg).
The mean weights of the sample during different times of observation are summarized in Figure 1.

Changes in mean weights between T4 and T0 for gastric banding (GB) sample versus gastric bypass sample. The difference in weight between the last detection of follow-up and preoperative time was assessed using a simple linear regression model, after processing data according to the Blom method, based on the inverse normal function. The difference between the weights is statistically significant for both GB (p < 0.001, R2 = 0.80) and gastric bypass (p < 0.001, R2 = 0.74), as shown in figure. The solid line indicates the Stima; the dotted line indicates the prediction limits, with 95% confidence limits. The regression models have tight bands of confidence, supporting the robustness of the conclusions above.
For each patient, the ideal weight was calculated with Lorenz's formula. It is possible to state that excess weight loss percentage (%EWL) values present statistically significant differences between one observation period and the next: data obtained by linear regression show an R2 of 0.8588 (p < 0.0001) with regard to the evaluation at time 4 compared with time 1. Similar data were recorded between time 4 and time 3, (R2 = 0.8588; p < 0.0001) and between time 3 and time 2 (R2 = 0.8374; p < 0.0001). Instead, statistical significance was lower when comparing time 2 and time 1 (R2 = 0.495; p < 0.0001). Related to %EWL, the gastric bypass group had better outcomes than the group who underwent GB, especially from the sixth postoperative month, with a statistically significant difference (R2 > 0.8; p < 000.1) (Fig. 2).
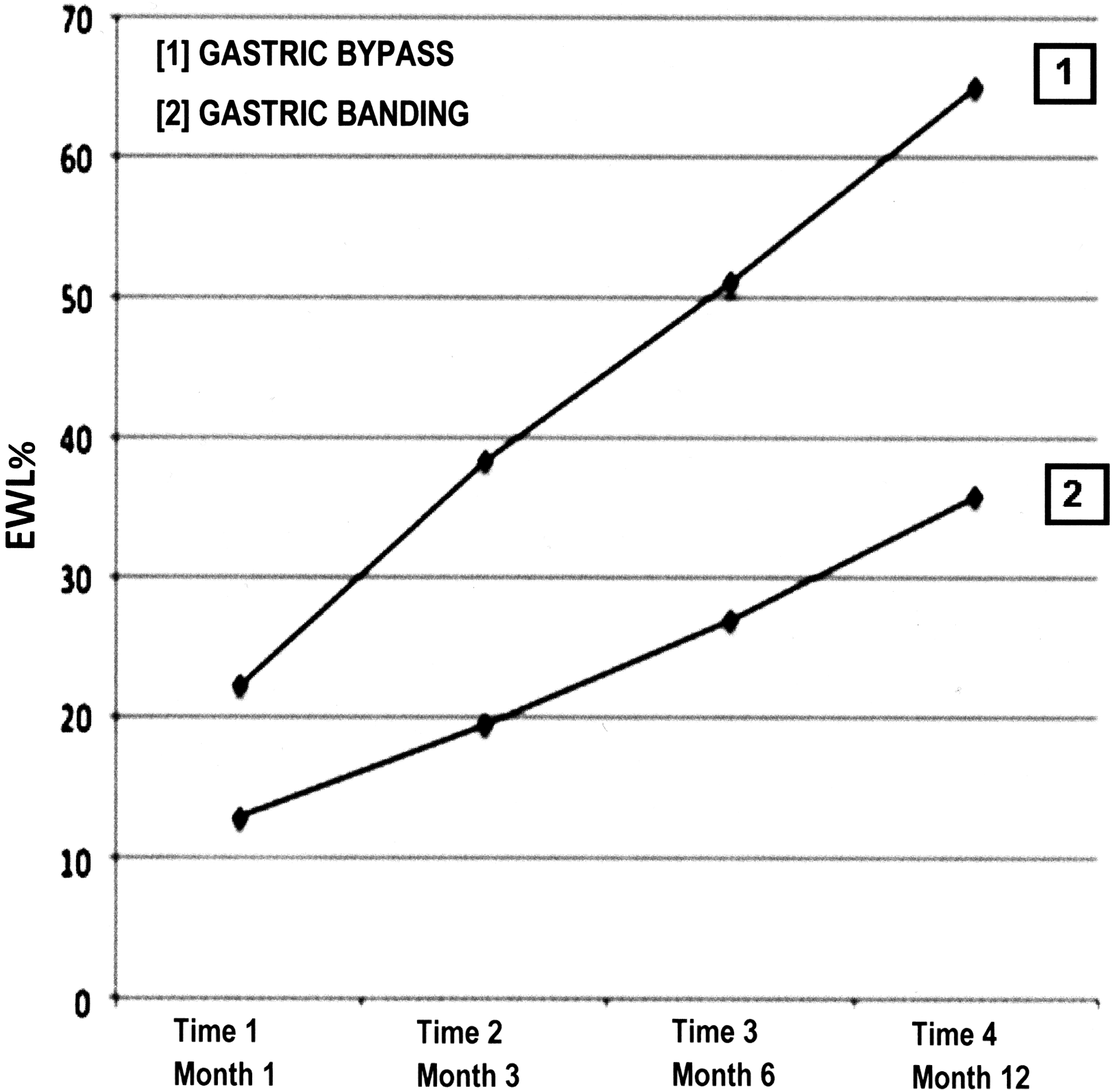
Excess weight loss percentage (%EWL): comparisons between times 1 and 4. By comparing the curves for the variation of %EWL, we can highlight a trend whereby the gastric bypass group has better results than the gastric band group.
The descriptive statistics show that the average scores of QoL improved in relation to the observation time in postoperative periods (Fig. 3).
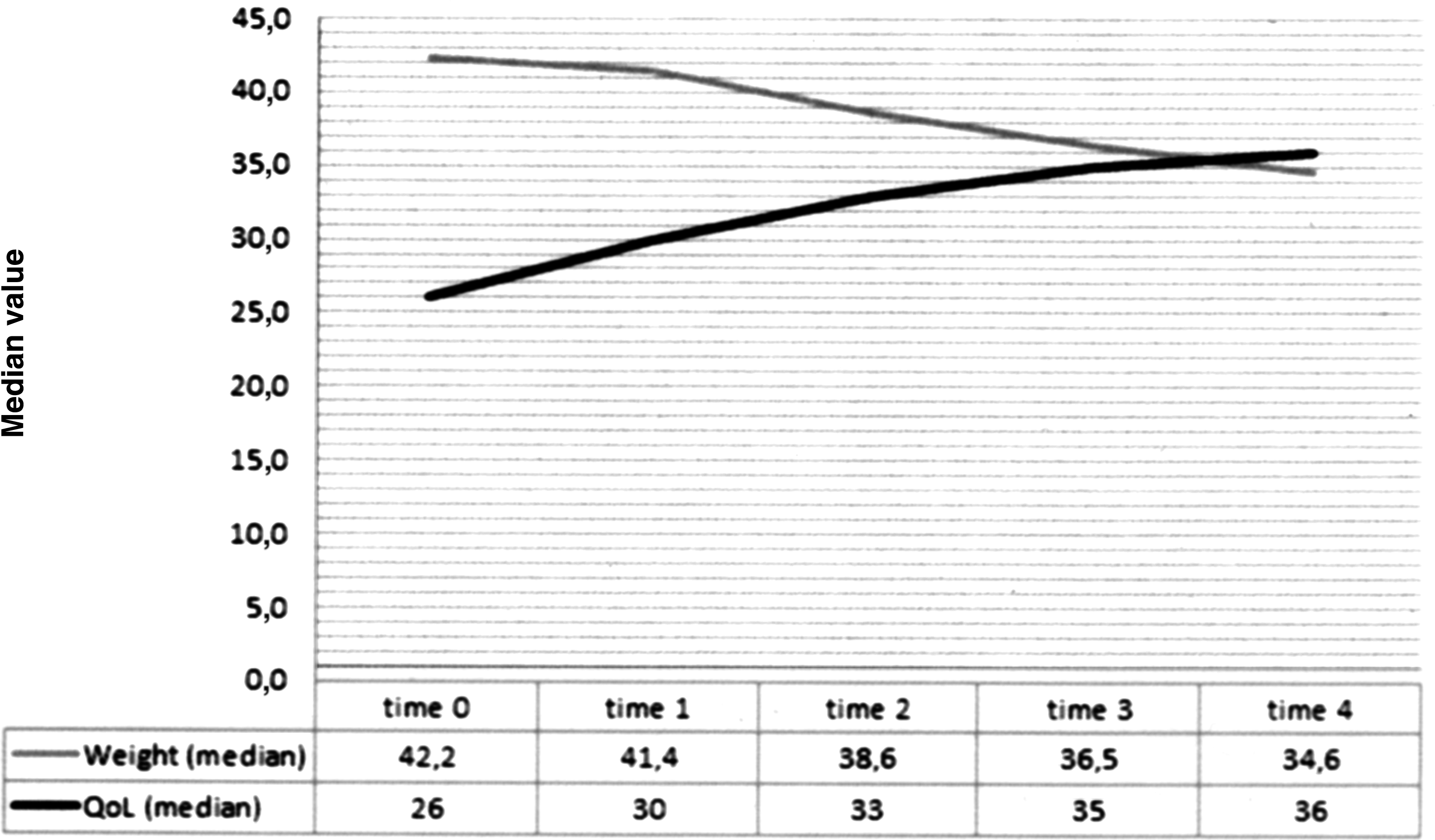
Improvement in quality of life (QoL) versus weight loss (time 0–time 4). Data from descriptive statistics show that the median scores of QoL improved in relation to the observation time in postoperative periods (time 0: 26 [19–31]; time 1: 30 [23.5–30.5], time 2: 33 [26–37]; time 3: 35 [29–38]; and time 4: 36 [32–39]; p < 0.001) and in relation to decrease of median weight (time 0: 42.2 [38.0–46.9]; time 1: 41.4 [37.9–47.4]; time 2: 38.6 [34.3–43.9]; time 3: 36.5 [32.4–41.2]; and time 4: 34.6 [30.7–39.7]; p < 0.001).
In addition, linear regression shows that the time factor is a major variable in the evolution of QoL perceived by each patient. In fact, there is a strong correlation between the course of perceived QoL and the observation periods ranging from 12 to 6 months (R2 = 0.90; p < 0.0001), from 6 to 3 months (R2 = 0.87; p < 0.0001), and from 3 to 1 month postsurgery (R2 = 0.82; p < 0.0001).
Similar data can be obtained after subdivision of the sample into two groups on the basis of the type of intervention. It is important to note that in this study, the group of subjects who underwent gastric bypass had more benefits in terms of better HRQoL than the GB group (Table 2), even if there are no statistically significant differences between the time periods examined. In fact, a statistically significant difference emerges only in the 3–6 months period and in the 6–12 months period after surgery (p < 0.05) (Table 1).
p-Value from Wilcoxon test.
BY, bypass intervention; GB, gastric banding; QoL, quality of life.
The strong correlation, noticed using linear regression on the total sample, is confirmed even after subdivision of the sample (Table 2).
Discussion
The results of this study show that weight loss in patients undergoing gastric bypass is higher than weight loss in those who underwent GB, with a statistically significant difference especially in the time period between the third and the twelfth month (p < 0.0001). In literature, there are only few studies providing data about the comparison between the results of these two kinds of interventions.
The positive outcomes of weight loss are reflected in the perceived QoL: important incremental improvements occur in the observation following the third month after surgery. With reference to the Laval Questionnaire, greater improvements are identified between the 6th and 12th month in all domains: emotions (R2 = 0.85; p < 0.0001), activity (R2 = 0.83; p < 0.0001), hygiene (R2 = 0.78; p < 0.0001), social interactions (R2 = 0.78; p < 0.0001), symptoms (R2 = 0.76; p < 0.0001), and last, sexual life (R2 = 0.70; p < 0.0001). These positive changes, along with a better QoL, occur simultaneously with weight loss, which shows that surgery impacts not only on physical health but also on aspects related to the improvement of self-acceptance and self-image. These great improvements between the sixth and twelfth month are related to the fact that surgery induces improvements in body image and perceived attractiveness. 16 Even though surgery-related changes allow the person to build a new and more positive self-concept, 17 this process is slower and more difficult than adaptation to physical and exterior changes: 18 we expect these changes in psychological dimension of QoL will appear later than the ones in physical dimension.
It is important to underline that in the first 3-month postoperative period, there are no statistically significant differences between data collected from patients undergoing gastric bypass and those collected from subjects who underwent adjustable GB. Starting by the sixth month, there is a significant change between these two groups, with a higher increase of excess weight loss, a major decrease in BMI, and a greater improvement in the scores related to the QoL in subjects undergoing gastric bypass: after the third month, in the sixth month, the QoL of patients undergoing Roux-en-Y gastric bypass becomes better than the QoL of those who underwent adjustable GB (Fig. 4).
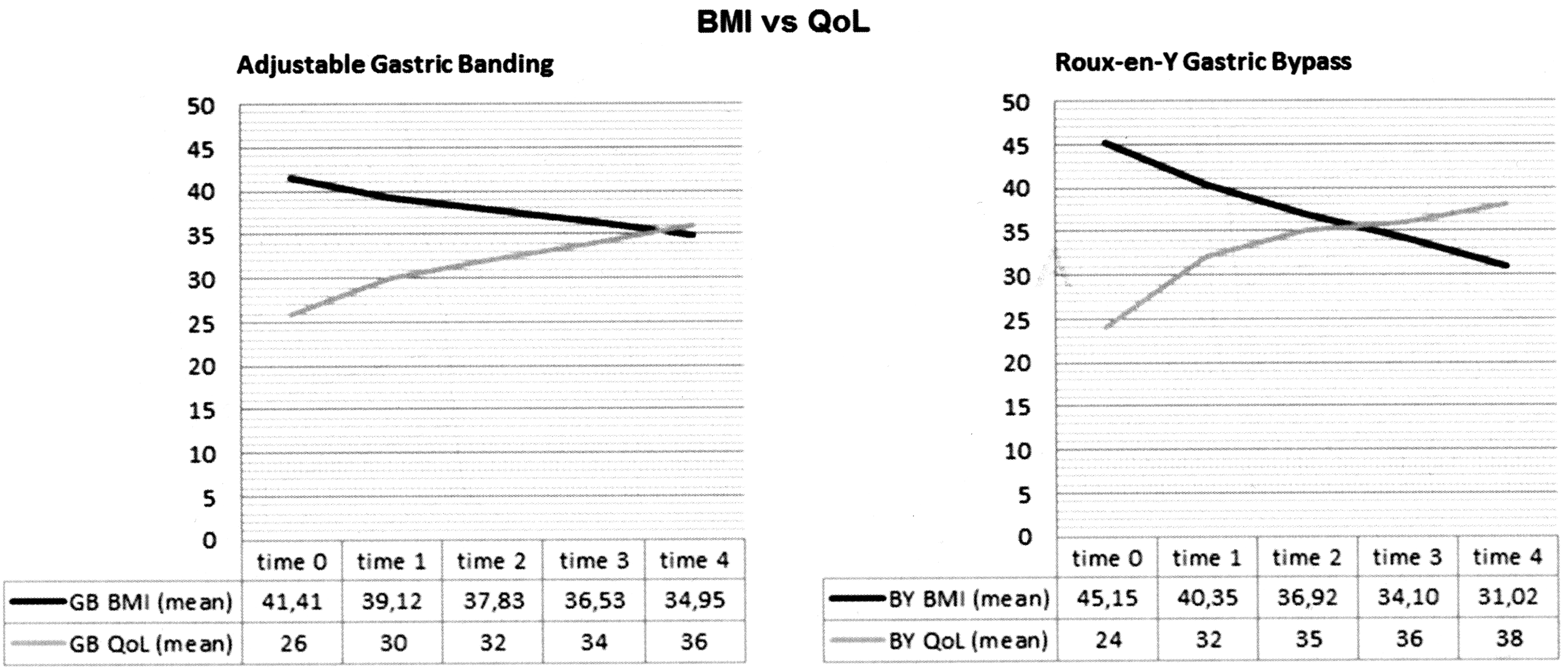
Improvement in QoL versus decrease in BMI: comparison between interventions. Starting by the third month, the QoL of patients who underwent Roux-en-Y gastric bypass becomes better than the QoL of those who underwent adjustable GB. At the first time of observations in the gastric bypass group, weight loss was greater; for the improvement in QoL, statistically significant differences between the two groups did not occur. Statistically significant differences emerged instead from the sixth month of observation. BY, bypass intervention.
Conclusions
This study investigated how bariatric surgery and weight loss can induce changes in the perceptions of QoL in obese people. Different studies show that bariatric surgery interventions have an important influence on QoL, which is improved regardless of the type of surgery. 19 Our results confirm data obtained from several studies conducted on patients undergoing laparoscopic GB and show that during the first year after surgery, people experience rapid and highly significant improvements in QoL. 20 Levels of perceived QoL already return to general community normal values 12 months after surgery.20,21 These previous studies assessed QoL using generic tools, such as the SF36. The strength of our study is the use of Laval Questionnaire, a tool specifically created for QoL assessment in obese patients undergoing bariatric surgery. We also compared the effects on QoL of Roux-en-Y gastric bypass and laparoscopic adjustable GB, an aspect poorly treated in literature: many studies have investigated the results of the interventions in terms of weight loss, but only few studies have compared the impact of these interventions on QoL.
A limit of this study can be found in the shortness of the follow-up period: future research might consider a longer follow-up period (3–7 years, according to the literature) to verify whether the improvements obtained by surgical interventions are maintained over time.
In conclusion, we can say that bariatric surgery has the potential to be not only an esthetic solution but also an appropriate procedure for the improvement in QoL of obese people.
Funding Sources
None.
Footnotes
Authors' Contributions
R.A. and A.D. conceived the study, S.T. performed the statistical analysis, and E.L., S.R., and E.R. supervised the clinical content of the study and helped in data collection.
Author Disclosure Statement
No competing financial interests exist.