
Abstract
Objective:
To report on the changes over time in inflammatory and cardiometabolic profile after Roux-en-Y gastric bypass in an overweight Chinese cohort.
Setting:
Outpatient clinic of a hospital in Beijing, China.
Methods:
This prospective cohort study involved 89 patients who met the indications for bariatric surgery in China. Serum leptin, tumor necrosis factor α (TNF-α), adiponectin, C-reactive protein (CRP), interleukin-6 (IL-6), and cardiometabolic profile were monitored at baseline (presurgery) to 12 months postsurgery.
Results:
Serum CRP decreased from 39.39 mg/dL at baseline to 31.06 mg/dL at 12 months (p < 0.001). Serum leptin and IL-6 also steadily decreased throughout this time course, whereas serum adiponectin decreased to 5.52 μg/mL at 6 months and increased thereafter. An inconsistent pattern was observed for TNF-α. Fasted lipid profile, blood glucose, and HbA1c improved during follow-up.
Conclusion:
Weight loss after bariatric surgery was associated with lower serum concentrations of several inflammatory markers and an improved cardiometabolic profile during the first 12 months of follow-up in this Chinese cohort. These findings may reflect improvement in subclinical inflammation secondary to the reduction of the body fat mass, but also suggest other potential mechanisms to explain the improvement of cardiometabolic profile after metabolic surgery.
Introduction
T
Roux-en-Y gastric bypass (RYGB) is a bariatric surgical procedure that has been shown to induce considerable weight loss in obese patients through restriction and malabsorption.13,14 The RYGB procedure involves creating a 30 mL pouch from the upper stomach, which is anastomosed to the dissected jejunum, bypassing the remaining stomach and upper part of the small intestine. Previous studies have shown a substantial reduction in serum concentrations of leptin, but nonsignificant changes in soluble TNF-α receptor-1 and adiponectin levels, in the 6 months after bariatric surgery.11,15,16 A significant reduction in serum CRP and IL-6 and an increase in adiponectin were also reported 6 months after surgery4,13,15; whereas the reported effects of bariatric surgery on inflammatory markers have been inconsistent, especially in patients with diabetes.
As there have only been a handful of studies that have explored the effect of bariatric surgery on overweight subjects, we aimed to investigate the changes in serum concentrations of inflammatory and cardiometabolic factors in overweight Chinese subjects who were followed up for 12 months after RYGB surgery.
Materials and Methods
Study design, setting, and participants
This prospective observational cohort study was conducted in 89 participants (of whom 61 were women) between 2014 and 2016 in the outpatient clinics of hospitals in Beijing, China. The patients met the criteria for surgery, based on guidelines for bariatric surgery for obesity in China.17,18 These guidelines stipulate that for patients with a body mass index (BMI) of 27.5–32.5 kg/m2, surgery is recommended if they fail to achieve metabolic control for diabetes after lifestyle modification and drug treatment, and have at least two of the following metabolic disorders: serum triglycerides ≥1.70 mmol/L, high-density lipoprotein (HDL) cholesterol <1.03 mmol/L in men or HDL cholesterol <1.29 mmol/L in women, and systolic blood pressure ≥130 mm Hg and/or diastolic blood pressure ≥85 mm Hg. For patients with a BMI of 25–27.5 kg/m2, surgical intervention should only be used when the patients cannot achieve glycemic control after lifestyle modification and drug therapy and have at least two other metabolic disorders. 17 None of the patients had previously undergone bariatric surgery.
Index surgical procedure and sequence of follow-up
The surgical procedure was similar (RYGB) for all patients. In brief, after exposing the ligament of Trietz by advancing the omentum toward the upper abdomen, the jejunum was transected with a laparoscopic linear stapler, 50 cm from the ligament of Trietz. A side-to-side functional end-to-side jejunojejunostomy was created 100 cm distal to this point. The linear stapler was used to create the enteroenterosotomy. Once the stapler was removed, a running 2-0 surgical suture was used to close the common opening with an endoscopic suturing device. 19 A small stomach pouch, approximately 30 mL in volume, was created by dividing the top of the stomach from the rest of the stomach. The bottom end of the divided small intestine was brought up and connected to the newly created small stomach pouch. 20 Patients had no oral intake by mouth for 3 days after the surgery. Then, a liquid diet was carefully introduced after a swallow test with gastrografin. The liquid diet was continued for 2 weeks. Upon discharge, patients were followed up in outpatient clinics for 12 months, with follow-up visits at 3, 6, and 12 months.
Baseline and follow-up evaluations
At baseline and at follow-up evaluations, height (to the nearest 0.1 cm) was measured using a portable stadiometer in a participant without shoes, stretching to the maximum height with the head positioned in the Frankfort plane. Weight was measured and BMI derived using a body composition analyzer. For each participant, blood samples were drawn after an overnight fast. The serum concentration of CRP was determined using a high-sensitivity immunoturbidimetry method. Serum concentrations of leptin, adiponectin, IL-6, and TNF-α were determined using enzyme linked immunosorbent assay kits (DGR, Marburg, Germany). Lipid profile was measured using an auto analyzer (Abbott analyzer, Chicago, IL). Fasting glucose was measured in plasma by a hexokinase method using a Roche/Hitachi 911 Analyzer and Roche Modular P Chemistry Analyzer.
Ethical considerations
All patients were informed about the operative procedure offered, including potential advantages and probable complications, and signed the written informed consent and agreed to participate in the study. Moreover, they were informed about the study procedures. The study protocol was approved by General Hospital of Chinese's Ethics Committee.
Statistical analysis
SPSS software (version 11.5; Chicago, IL) was used for statistical analysis. The Kolmogorov–Smirnov test was used to evaluate the distribution of data. Values are expressed as median and 25th to 75th percentiles confidence interval. The trajectory of BMI and inflammatory markers during follow-up was investigated with the use of Kruskal–Wallis for repeated measures. A p value <0.05 was used to characterize statistically significant results.
Results
In our study, mean age was 43.5 ± 10.2 years for the whole group (42.3 ± 9.8 years for men and 45.6 ± 11.9 years for women participants, respectively (p = 0.236)). The marital status of participants was 10.1% single, 88.8%, married, and 1.1% divorced. There was a positive smoking habit in 30.7% of the subjects.
As is shown in Table 1, the mean CRP was 39.3 mg/dL at baseline, with a downward trajectory during follow-up to the lowest value of 31.0 mg/dL at 12 months (p < 0.001). Serum leptin and IL-6 also steadily decreased from baseline to 12 months of follow-up (p < 0.001). Most follow-up values were also lower than the baseline values for TNF-α; however, a variable trajectory was observed during follow-up with values falling between baseline and 3 months and between 6 and 12 months, but rising between 3 and 6 months. Mean serum adiponectin concentrations were 7.0 μg/mL at baseline, but decreased and remained at 5.5 μg/mL between 3 and 6 months, before increasing to 6.5 μg/mL at 12 months (Table 1). In diabetic patients, all inflammatory markers fell significantly over the 12-month period (p < 0.001 for all).
Values are expressed as median and 25th to 75th percentiles. p Value is from the Kruskal–Wallis test and refers to the overall differences between follow-up times.
CRP, C-reactive protein.
The mean BMI was 29.9 kg/m2 at baseline and steadily fell during the 12-month follow-up period with a value of 25.3 kg/m2 at 6 months and a value of 25.3 kg/m21at 2 months (p < 0.001). As can be seen from Figure 1, lipid profile, fasting blood glucose, and HbA1c improved during this period (p < 0.001, Fig. 1). HDL-C remained relatively stable from the baseline till 6 months (1.07 mmol/L vs. 1.14 mmol/L); however, at 12 months it decreased to 0.58 (mmol/L) (p < 0.001, Fig. 1).
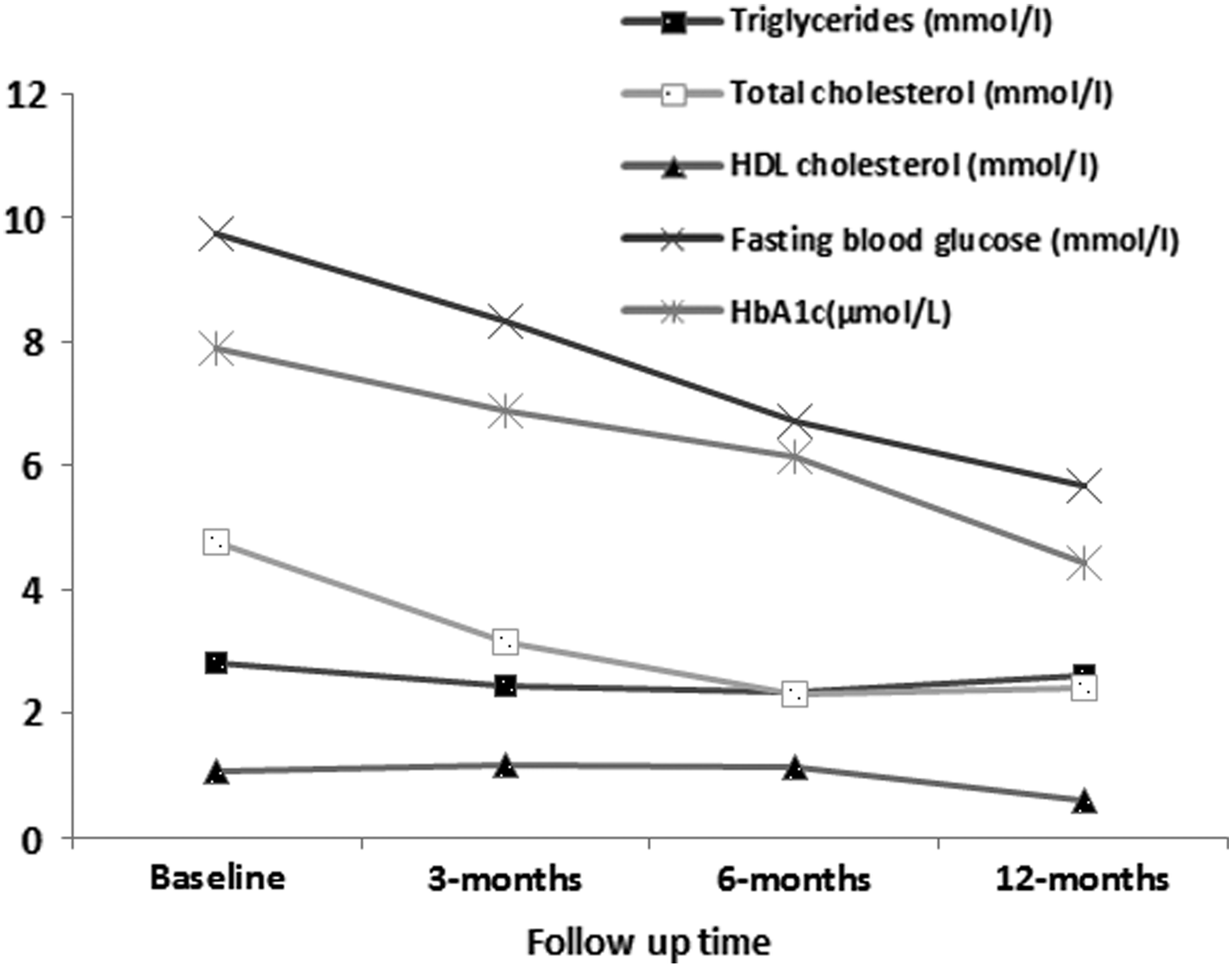
Changes in lipid profile and glucose hemostatic parameters during follow-up after bariatric surgery.
The changes in BMI (end of observation–baseline) were inversely related to serum CRP (r = −0.125, p = 0.023) and serum IL-6 concentrations (r = −0.182, p = 0.011), whereas positively correlated with adiponectin (r = 0.265, p = 0.001) at the end of the follow-up period. Moreover, changes in fasting blood glucose (end of observation–baseline) were positively correlated with adiponectin (r = 0.142, p = 0.039) and negatively correlated with CRP (r = −0.096, p = 0.048) and IL-6 (r = −0.106, p = 0.042) at the end of the follow-up period.
Discussion
We have investigated changes of inflammatory markers over a period of 12 months after bariatric surgery in Chinese participants. The main finding of this study is that inflammatory markers decreased significantly over the 1-year period of follow-up, paralleling a decrement in total adiposity and improvement in cardiometabolic profile.
The effects of bariatric surgery on inflammatory markers have been examined in a number of observational studies, many of which have been reviewed by Rao a few years ago. 21 In this systematic review and meta-analysis, a favorable effect of surgery on CRP and IL-6 levels throughout the first year of follow-up, and mostly nonsignificant on TNF-α, is consistent with our findings. However, other studies have reported favorable effects of bariatric surgery on TNF-α. 22 In general, changes in inflammatory markers after bariatric surgery have been inconsistent, but have generally shown a decline in proinflammatory markers such as CRP, IL-6, TNF-α, leptin, intracellular adhesion molecule 1, and plasminogen activator inhibitor 1, and an increase in anti-inflammatory markers such as adiponectin and interleukin-10 (IL-10).21–23
Adipose tissue from obese subjects is characterized by an inflammatory state, which is believed to contribute to systemic low-grade inflammation in obesity. 24 More than 24 inflammatory makers have been reported, whose circulating levels are altered in obese human subjects. 25 The source of the elevated levels of these markers and their specific role in obesity, and its complications, have not been fully elucidated, rendering very challenging interpretations of changes in their levels after surgery and other interventions to treat obesity. Although most of these markers are expressed by adipose tissues, they are also produced by other tissues; within the adipose tissue, fat cell and nonfat cell productions coexist. Furthermore, the profile of adipose tissue-derived inflammatory markers varies across adipose tissues from different body sites. 21 A focus on total fat mass reduction alone is likely to be a very simplistic view of the underlying mechanisms of inflammation control after bariatric surgery. However, changes in inflammatory status are related to an improvement in cardiometabolic risk profile, and this suggests that it is at least part of the dynamics toward overall health improvement after surgery for obesity.
Limitations and strengths
This study has some limitations. Only patients receiving a RYGB were included. Whether the direction and magnitude of the observed effects may be applied to other bariatric surgical procedures is, therefore, not addressed. A systematic review of the few available long-term outcome studies of bariatric surgery tends to suggest better outcomes for gastric bypass.26–27 Moreover, we did not collect information on medication during our follow-up. It is possible that changes in drug treatment may affect the metabolic and inflammatory marker profile. It may have been useful to have collected data on body composition and other measures of adiposity, such as fat percentage and waist circumference. Our study also has major strengths including the relatively large patient sample and the repeated investigations of a range of inflammatory markers at baseline and during follow-up, which allowed us to carefully characterize their trajectories up to 12 months after bariatric surgery. Also there are only a handful of studies that have investigated the effect of the bariatric surgery on overweight and diabetics patients.
Findings from this cohort of Chinese patients indicate that bariatric surgery can significantly improve inflammatory factors in eligible patients with type 2 diabetes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.