
Abstract
Background:
Laparoscopic Roux-en-Y gastric bypass (LRYGB) is a complex procedure. Increasing case experience improves operative times for surgeons. Less is known about the impact of experience of other surgical team members.
Methods:
One hundred seventy-nine consecutive LRYGB cases were analyzed. Total operating room times (ORT) and surgical times (STs) were tabulated, and linear regression was used to detect correlation between these times and the case counts of surgical team members. Efficiency measures were evaluated for cases done synchronously on a given day versus individual cases.
Results:
Minimum case count of any scrub nurse present showed a statistically significant relationship to both ORT and ST, with mean decreases of 0.686 ± 0.224 and 0.561 ± 0.207 min per one-case increase in experience, respectively. Successive cases averaged less than standalone procedures.
Conclusions:
Case count of the least experienced scrub nurse appeared to have a significant impact on efficiency in LRYGB. LRYGB cases performed successively showed improved efficiency.
Introduction
O
The learning curve for laparoscopic Roux-en-Y gastric bypass (LRYGB) is steep.1–3 The procedure is often done in high volumes in single centers, and the materials and steps become standardized with repetition within the surgical team. The operation is technically demanding on all members of the team, and cohesion is essential to achieve efficiency and desirable patient outcomes in a procedure with considerable potential for adverse events. 4
Team members
The members of a surgical team can be generally divided into three groups: nursing (including scrub nurses and circulating nurses), anesthesia (including anesthesiologists and anesthetists), and surgeons (including the attending surgeon and first assistant).
The scrub nurses directly assist the surgeons by repeatedly organizing, cleaning, preparing, and passing a variety of surgical instruments, staplers, and other devices. Besides being familiar and facile with these devices, they must anticipate the course of the procedure and the needs of the surgeons to achieve maximum efficiency in executing these tasks. 5 Circulating nurses play a crucial role in room setup, breakdown, and equipment maintenance throughout the perioperative period. Preoperative huddle and accurate setup can prevent missing items and delays in progression of the procedure.
The role of the anesthesia team is particularly prominent in LRYGB. Typical functions within laparoscopic surgery include induction, emergence, and physiologic control of the patient during the procedure, which can be challenging in morbidly obese patients. In addition, maneuvers such as transoral passage of orogastric tubes or the transoral stapling device represent a significant potential source of difficulty and inefficiency.
The primary surgeon performs the great majority of the procedure and thus is largely responsible for case efficiency. At academic institutions, fellows typically participate as either the primary surgeon or assistant. Generally, fellow contribution toward accomplishment of the case increases through the year with increasing experience with the procedure. Efficiency and operative times may vary significantly based on both the experience of the fellow and their degree of participation relative to the attending surgeon. 5
Measures of experience
Understanding the role of each team member's experience in the overall efficiency of the procedure may lead to improvements in personnel allocation. Due to scheduled staffing breaks during the procedure, multiple individuals may contribute to fulfill the role of scrub nurse, anesthetist, or circulator within a given case. Understanding the effects and dynamics of these changing teams is critical in the attempt to identify potential sources for process improvement.
There are several variations in the teams, which may lead to hypothetical gains or losses in efficiency. Factors that would likely be associated with improved efficiency might include the participation of nurses with great experience in the procedure and cases completed with minimal breaks and personnel variations within the team. Factors associated with decreased efficiency measures might include new team members being proctored in the procedure, members with lesser experience in the procedure, or cases with multiple changes in the team due to breaks or shift changes. Therefore, an assessment of efficiency relative to experience should account for multiple possible determining factors.
OR team experience and case efficiency
Literature investigating the impact of the case experience of individual team members on efficiency in laparoscopic gastric bypass surgery is limited, despite the proven utility of such multidisciplinary assessments within the field of surgery.6–8 However, with improvements shown by surgeons as their case count increases1,2 and greater morbidity and mortality associated with less experienced assistants, 9 the potential yield for such research is significant.
Material and Methods
A single institution, American College of Surgeons Center of Excellence, database was queried for all LRYGB cases performed during three academic calendar years, from June 1, 2007 to June 30, 2010. The study was conducted with the approval of the Institutional Review Board. Cases were completed within the auspices of a minimally invasive surgery fellowship, and so academic calendar years were used to control the progress of fellows during their year of training. All the procedures were completed by three primary surgeons, each of who had a case experience with LRYGB of greater than 500 cases.
In addition, the program has endeavored to standardize aspects of the process, including preoperative assessment, intraoperative technique, and postoperative care. Operative and perioperative data were compiled from the existing database, nursing, and anesthesia records recorded during the procedure. Cases with additionally performed procedures identified by secondary Current Procedural Terminology codes or those with incomplete data were excluded from analysis.
The initial query provided the following relevant times: time patient entered operating room (“in room time”), surgical start time, surgical end time, and time patient exited operating room (“out of room time”). For all cases, “total operating room time (ORT)” was calculated from the difference between “in room time” and “out of room time.” “Surgical time (ST)” was calculated from the difference between “surgical start time” and “surgical end time” and represents the time from incision to skin closure.
All personnel logged as present during the operation were tabulated. Personnel were categorized as surgeon, fellow, attending anesthesiologist, anesthetist, scrub nurse, or circulating nurse, as labeled in the intraoperative nursing report. Furthermore, the team member who spent the greatest total amount of time in the operating room during the procedure was designated as the “primary” team member within their given category. Medical students and observers were disregarded for this study. For each entrant, the total number of cases in which they participated during the series was designated as his “case count.” Once each team member's case count had been calculated, this information was used to generate additional data for each case.
Primary Team Member Experience for a case was designated as the case count for the team member of the given category (Scrub Nurse, Circulating Nurse, or Anesthetist) present for the most total time during the case. Average Team Member Experience was the calculated mathematical average of the experience of all team members of a given category within the given category present for a case. Maximum Team Member Experience denotes the highest case count of any team member of a given category present for a case and Minimum Team Member Experience represents the case count of the least experienced team member.
The relationships between measures of team member experience (Primary, Average, Maximum, and Minimum as described above) and efficiency measures (ORT and ST) were evaluated for the Scrub Nurse, Circulating Nurse, and Anesthetist categories. Attending anesthesiologists were also not included, as PA-Anesthetists and Nurse Anesthetists perform the great majority of the case.
Bivariate analyses of the association between team member case counts and operative times yielded a value labeled Mean Time Decrease Per Additional Case. This value represents the expected decrease in the given operative time as the measure of experience (Primary, Average, Maximum, or Minimum) increases by one case. For example, a Mean Time Decrease of 0.5 min for Primary Anesthetist experience would represent a mean 0.5 min decrease in case time if the Primary Anesthetist case experience was increased by 1.0. Negative values for Mean Time Decrease indicate a mean increase in operative times with increasing values for team member experience.
To analyze the impact of fellow's training experience on operative times, all cases were designated as either First Half of the Training Year, performed from July 1 to December 31, or Second Half of the Training Year, covering cases between January 1 and June 30. The mean ORT and mean ST were calculated for each of these groups, and these means were compared and tested for statistical significance.
Finally, for a secondary analysis, cases were designated as First in Series, indicating a case that was immediately succeeded by another LRYGB, Successive in Series, indicating a case that was immediately preceded by another laparoscopic RYGB, or Not in Series for cases that were neither preceded nor succeeded by other laparoscopic RYGB cases. A series of cases were identified as cases following one another (based on surgery stop and surgery start times) with the same primary surgeon.
Statistical analysis was done using SAS software. A p-value <0.05 was used for statistical significance.
Results
General
A total of 182 cases were identified with three exclusions for concurrent procedures. The mean ORT for all cases was 231.6 min (standard error of the mean [SEM] = 3.79, standard deviation [SD] = 51.1). The mean ST for all cases was 176.1 min (SEM = 3.49, SD = 47.1).
Team member demographics
A total of 42 unique scrub nurses were present in the 179-case database. The highest documented case count during this series for any individual nurse was 63 cases. Mean case count was 7.8 cases, and 33 nurses participated in 10 cases or less during the series.
A total of 54 unique circulating nurses were present in the database. Circulating nurse data were incomplete for 5 cases, leaving 174 total cases for analyses. The maximum case count of any individual circulating nurse was 30 cases, and the average case count was 6.5.
Among anesthetists, 39 individuals were counted among 169 cases for which data were complete. Maximum case count was 31, and mean case count was 5.8 cases (Table 1).
Experience refers to total case count in database.
Team member experience and ORT
Analysis of Primary Scrub Nurse Experience (case count of scrub nurse present for the most total time during given case), Average Scrub Nurse Experience (mean case count of all scrub nurses present during case), and Maximum Scrub Nurse Experience (highest case count of any scrub nurse present for case) showed a mean decrease in ORT with increasing case experience. These results were not statistically significant. However, Minimum Scrub Nurse Experience (lowest case count of any scrub nurse present for case) was associated with a statistically significant decrease in mean ORT (p = 0.003) (Table 2 and Fig. 1).
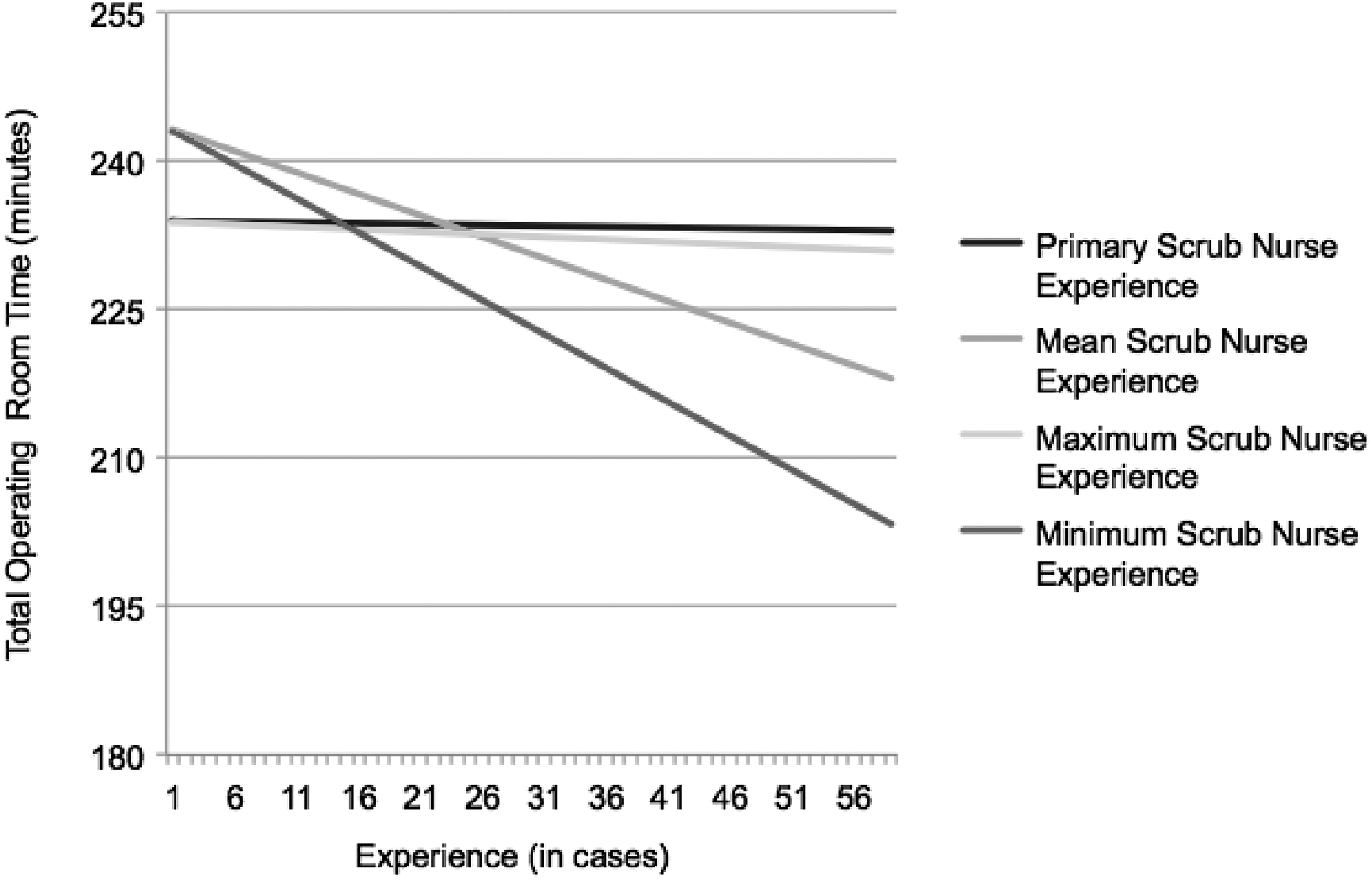
Effect of scrub nurse experience on total operating room time. Figure represents mean time decreases in total operating room time by increasing the given nurse's experience, as demonstrated by the slopes of the lines. Minimum and maximum values of x-axis were arbitrarily chosen to suggest the potential difference in surgical times for an experience (case count) value of 1 (minimum) versus 60 (approximate maximum in our 179-case database).
“Time Decrease Per Additional Case” represents mean decrease in operative time associated with increase in experience by one case. Bold font indicates statistically significant values.
Analysis of Primary, Average, Maximum, and Minimum Circulating Nurse Experience showed a mean decrease in ORT per additional case. These results were not statistically significant (Table 2).
Analysis of Primary, Average, Maximum, and Minimum Anesthetist Experience also showed a mean decrease in ORT per additional case, which was not statistically significant (Table 2).
Team member experience and ST
Bivariate analyses were run on all measures of scrub nurse experience with regard to ST (elapsed time from surgery start to surgery stop) as with ORT. Primary, Average, and Maximum Scrub Nurse Experience were associated with a mean decrease in ST (ST) per additional case. As with ORT, Minimum Scrub Nurse Experience showed a statistically significant mean decrease in ST (p = 0.007) (Table 3 and Fig. 2).

Effect of scrub nurse experience on surgical time. Figure represents expected mean time decreases in surgical time by increasing given nurse's experience, as demonstrated by the slopes of the lines. Minimum and maximum values for the x-axis were arbitrarily chosen to suggest the potential difference in surgical times for an experience (case count) value of 1 (minimum) versus 60 (approximate maximum in our 179-case database). Note that lines for primary scrub nurse experience and maximum scrub nurse experience are approximately overlain.
“Time Decrease Per Additional Case” represents mean decrease in operative time associated with increase in experience by one case. Bold font indicates statistically significant values.
Analysis of Primary, Average, Maximum, and Minimum Circulating Nurse Experience showed a statistically insignificant mean decrease in ST per additional case (Table 3).
Analysis of Primary, Average, Maximum, and Minimum Anesthetist Experience showed a mean decrease in ST per additional case. These results were not statistically significant (Table 3).
Fellow and resident experience: first half of year versus second half of year
Mean ORT for all cases performed from July 1 to December 31 was 225.0 min (SD = 49.1; SEM = 5.143). Mean ORT for all cases performed from January 1 to June 30 was 238.4 min (SD = 52.9; SEM = 5.64). The difference between the ORT was not statistically significant (p = 0.107).
Mean ST for all cases performed from July 1 to December 31 was 170.7 min (SD = 44.1; SEM = 4.62). Mean ST for all cases performed from January 1 to June 30 was 182.5 min (SD = 49.9; SEM = 5.32). The difference between the ST was not statistically significant (p = 0.096).
Cases in succession versus individual cases
Mean ORT for cases Not in Series (i.e., not preceded or followed by LRYGB) was 238.9 min (n = 109; SEM = 4.97). Mean ORT for First Cases in Series (i.e., followed by laparoscopic RYGB; not preceded by LRYGB) was 235.5 min (n = 34; SEM = 8.11 min). Mean ORT for Successive Cases in Series (i.e., preceded by LRYGB) was 205.4 min (n = 36; SEM = 6.93).
The difference in mean ORT between Cases Not in Series and First Cases in Series was not statistically significant (3.4 min; p = 0.730). However, the difference in mean ORT between Cases Not in Series and Successive Cases in Series was statistically significant (33.5 min; p = 0.001). The difference in ORT between First Cases in Series and Successive Cases in Series was also significant (30.1 min; p = 0.012) (Table 4).
n indicates number of cases in a given series. p-Values correspond to difference between two means indicated by “x&z,” “x&y,” and “y&z.” Times are represented as mean ± standard error.
Mean ST for cases Not in Series was 183.0 min (SEM = 4.65). Mean ST for First Cases in Series was 178.0 min (SEM = 7.43 min). Mean ST for Successive Cases in Series was 152.7 min (SEM = 6.07).
The difference in mean ORT between Cases Not in Series and First Cases in Series was not statistically significant (5.0 min; p = 0.578). The difference in mean ORT between Cases Not in Series and Successive Cases in Series was statistically significant (30.3 min; p = 0.001). The difference in ORT between First Cases in Series and Successive Cases in Series was also significant (25.3 min; p = 0.022) (Table 4).
Discussion
Overview
In this study of 179 LRYGB cases, measures of scrub nurse, circulating nurse, anesthetist, and fellow experience were used as an indicator of the surgical team's familiarity with the procedure and with each other. Primary outcomes included ST and ORT. Comparing these times provided insight as to whether time variation occurred during the operation itself, during the preparation and breakdown periods, or both. In addition, individual cases were compared with those that occurred in a series of LRYGB cases. This allowed brief analysis of any potential temporal, hour-to-hour effect on team dynamics.
Scrub nurse experience
The most statistically significant effect on operative times came from Minimum Scrub Nurse Experience. In this study, Minimum Scrub Nurse Experience represented the case count of the least experienced scrub nurse in the room at any point during the operation. The data showed that for each one-case increase in this value, ORT decreased by an average of 0.686 min and ST decreased by an average of 0.561 min. Thus, if expected total OR time using only the most experienced nurse (case count = 63) is compared to the expected time if a new trainee is added (case count = 1) to that same case, the result is a difference of ∼43 min (0.686 × 63).
This “limiting factor” association is highlighted by the lack of significance of our other measures of scrub nurse experience. Only Average Experience approaches a statistically significant association with operative times, and this average case count is likely to be heavily influenced by the same inexperienced nurses who make up the bottom end of Minimum Experience. It may be expected that the case count of the primary scrub nurse in any given case would be most influential on STs, but this relationship did not prove significant. In addition, Maximum Experience showed a much weaker association than its apparent counterpart, Minimum Experience; maximum experience tended to vary much less between cases, as a more seasoned scrub nurse almost always accompanied nurses with lower case counts.
These outcomes are consistent with subjective reports from the included surgeons, who have noted that cases seem to be least efficient when inexperienced team members are present. In an academic institution, there may be different reasons for this to occur, including training of a new nurse at the institution, relieving a more experienced nurse for breaks or lunches, or even when it is necessary to staff the room with a nurse not experienced in the procedure due to staffing constraints on a given day. These data can be used to evaluate both the efficacy of current nurse training processes and also estimate potential costs of such training.
Alternate training protocols may need to be developed and potentially adopted if these costs are deemed unsatisfactory. Likewise, knowing the cost, alternate strategies for room staffing by operating room administrators may be developed to maximize nurse experience for more complicated procedures such as laparoscopic gastric bypass. It may be more appealing to relegate the training of scrub nurses to less complex technically demanding cases when possible. Cross training is often done with nurses as they rotate through many different services as an introduction to the operating room. This allows for more flexibility in call pool scheduling for off hour cases.
As is happening in current evaluations of general surgical residency training, perhaps more track-specific training algorithms can be used to improve the efficiency and cost of complex procedures. For instance, cross training nurses in general surgery may not require them to learn familiarity with complex procedures such as gastric bypass, which in general do not occur at night. Training of nurses for complex procedures could then be done in a track-specific manner and perhaps some type of out of the OR team training would be beneficial and more effective. Indeed, prior studies have shown that as a scrub nurse gains experience with a procedure, objective measures of cognition and performance improve. 5 Such nurses become highly valuable as the volume of cases for a given procedure increases.
One final point suggested by the data is that majority of time saved by scrub nurse experience occurs during the procedure itself. The 0.561 min per additional case of saved ST represents 81.8% of the total saved OR time (mean = 0.686 s). This evidence supports the hypothesis that the largest improvement comes in the scrub nurse's increasing familiarity with the surgeons and the procedure, rather than simply in room setup or breakdown.
Anesthetist/circulating nurse experience
In this study, no significant association was shown between anesthetist or circulating nurse experience and operative times. One explanation for this phenomenon is the less mechanically intense role of these team members with respect to that of surgeons and scrub nurses, which likely results in both a shorter learning curve and less overall impact on the efficiency of the case. As with other team members, multivariate analyses may yield a more complete view of their role in these cases.
Fellow/resident experience
When mean operative times from the first half of the training year were compared to those from the second half, no significant difference was identified. Increased fellow case counts would presumably lead to increased skill, and thus, it may be expected that times during the second half of the year would be reduced. The most likely explanation for the lack of improvement is that the increased presence and participation of attending surgeons during the first half of the year offsets any increase in the skill of fellows as their training progresses.
During the beginning of the year, the attending surgeon is aware of the potential for cases to take longer and that more teaching will be needed. This may also be true for other members of the surgical team. It is likely that this leads to more involvement in all parts of the procedure by the attending during this time of year, including room setup, scrub table setup, and the conduction of the case. As the year goes on, increasing responsibility may be relegated to the fellow, including all of these aspects, starting or finishing the case autonomously. We did not identify any other means to control for these aspects of the case given the data available.
Cases in series versus individual cases
Our data suggest that dedicating multiple consecutive time slots to laparoscopic gastric bypass cases may also lead to greater efficiency. Out of 179 total cases in our study, we identified 70 that were part of series of LRYGBs (two or three consecutive LRYGB cases). For the 34 “First Cases” in these series, that is, the first LRYGB cases of the day, the mean ORT and ST were nearly identical to the means of the 109 standalone cases: differences were 3.4 and 5.0 min for ORT and ST, respectively. However, when compared to standalone cases, the mean times for the second or third cases in a series showed a highly significant difference at more than 33 min lower for total OR time and 30 min for ST.
These data suggest that surgical teams have the capability of streamlining their procedures and increasing efficiency by performing the same operation multiple times in a given day. The possibility of saving over 30 min per case is a clinically and administratively significant prospect; when compounded over the course of three or four cases, an institution may approach the possibility of scheduling additional surgeries. Improving standardization and decreasing case-to-case variability have also been shown to decrease morbidity and mortality in Roux-en-Y gastric bypass, which is another overarching goal of all efficiency measures. 10 As dedicated minimally invasive suites have been shown to significantly increase intraoperative efficiency, 11 future research may illuminate similar advantages to dedicating extended multiple-case time slots, or even full OR days, to specific procedures.
Potential limitations
By the subjective report of nurses, the intraoperative record is inherently difficult to maintain. Thus, records of nurse attendance and time logs are prone to inaccuracy. With the current system in place, there is no easily identifiable way to improve this aspect of the data.
No analyses or corrective factors were applied to account for the increasing experience of the attending surgeons over the time frame included in the database. However, studies have shown that after a steep learning curve of up to 100 cases, improvements in operating time tend to become less dramatic.1–3 With the chosen surgeons each conducting over 500 cases and thus residing on the flat segment of the proposed learning curve, it is unlikely that their additional experience would have a significant impact on the results of the study.
While analyzing the relationship between case experience and operative times, lines of fit were used to generate projected decreases in time as experience increases. In reality, as with the surgeon's learning curve, skill improvement for nurses and other team members likely plateaus after a certain number of cases. A database with more cases would better allow for a polynomial best-fit line, which is likely more realistic over extended experience.
Indeed, many of the scrub nurses in this study had experience with LRYGB procedures before the time period included in our database. The case counts gleaned from the database could not account for this prior experience or their increasing familiarity with the procedure over the included range. However, it is likely that case counts over the course of the database were suggestive of overall case experience for the nurses' careers.
Finally, patient demographics, comorbidities, or risk factors for complications were not included in this study. The LRYGB is a highly standardized elective procedure and only primary bypasses were included, but additional analyses may be necessary to account for patient-specific impact on STs.
Conclusions
A significant association was found between the minimum case experience of participating scrub nurses and both ST and ORT. Case experience of anesthetists and circulating nurses did not show a significant relationship to operative times. Data also suggested a significant difference in mean ST and mean operating room time between successive LRYGB cases and single cases. Institutions may use these data to develop and adopt alternate training initiatives or staffing protocols for members of the operating room team, which may lead to improvements in efficiency, should these findings be deemed too costly.
Footnotes
Author Disclosure Statement
No competing financial interests exist.