
Abstract
Background:
Obesity poses challenges to male reproduction, but the effect of bariatric surgery on semen parameters and fertility is debated. This study evaluates Roux-en-Y gastric bypass (RYGB) influence on these variables.
Methods:
Seventy-nine sexually active men attempting to conceive with a partner were stratified into four groups: Group 1 (n = 23)—bariatric follow-up ≥5 years; Group 2 (n = 23)—mean bariatric follow-up 2 years; Group 3—obese controls (n = 18); Group 4—lean controls (n = 15). Groups 2, 3, and 4 were matched for age; Groups 1, 2, and 3 were matched for body mass index (BMI). Sexual quality of life questionnaire for males (SQOL-M), fasting blood glucose, C-reactive protein, vitamin D, zinc, total testosterone (TT), and free testosterone (FT), estradiol (E2), sex hormone-binding globulin (SHBG), and semen parameters were investigated.
Results:
SQOL-M scores increased; vitamin D was low in most of Group 2 and Group 3 participants, negatively correlating with BMI (p < 0.01). TT, FT, and SHBG improved postoperatively; however, E2 remained elevated. Semen aberrations occurred in 57.1% of Group 2 patients and BMI correlated with oligoasthenoteratospermia. Scant bariatric men fathered a child (13.0% preoperatively, 4.3% postoperatively, not significant).
Conclusion:
Semen abnormalities and subfertility were observed after RYGB, despite improved androgenic profile and SQOL-M. Possible negative impacts of hyperestrogenism and hypovitaminosis D on semen parameters warrant further studies.
Introduction
A
In view of the conflicting reports, the long-term effect of weight loss induced by bariatric surgery on semen parameters and fertility was addressed in a controlled study. It was hypothesized that frequent sperm aberrations and low fertility rate would be encountered, despite the metabolic and hormonal benefits of the bariatric intervention, and the improved sexual quality of life (SQL).
Materials and Methods
Ethical considerations
This protocol was approved by the Institutional Ethical Committee, and all participants gave written informed consent.
Experimental design, eligibility, and patient enrollment
This was a partly prospective, partly retrospective, observational, controlled cohort study. Male patients (n = 79) from a public academic hospital were consecutively recruited for clinical and biochemical assessment, including retrospective information collected from the hospital files, and standard semen analysis. The inclusion criteria were sexually active men of reproductive age (18–49 years), with or without type 2 diabetes, subjected to Roux-en-Y gastric bypass (RYGB). Bariatric participants with very long follow-up (Group 1, n = 23) were often out of this age bracket, thus in this group semen analysis was not part of the protocol. In addition to regular sexual life with a female partner, recruited bariatric and control participants were also attempting to conceive with a partner.
The exclusion criteria were take down of the bariatric operation, history of endocrine disorders (except for type 2 diabetes), cancer including radiotherapy or chemotherapy, hormonal replacement therapy, HIV/AIDS, or other sexually transmitted infection, vasectomy, organ failure, substance abuse, cognitive impairment, or refusal to participate in the study.
Stratification
Group 1: Operated participants with very long-term follow-up (≥5 years, n = 23).
Group 2: Recently operated participants (1–2 years, n = 23).
Group 3: Overweight and obese nonsurgical controls (n = 18).
Group 4: Lean controls (n = 15);
Surgical intervention
Laparoscopic or open RYGB entailed the creation of a 30–50 mL gastric pouch, a 100 cm alimentary limb, and a 60–80 cm biliopancreatic limb.
Clinical and laboratory assessment
Relevant demographic and clinical variables were recorded, including the sexual quality of life questionnaire for males (SQOL-M), and confirmed whenever appropriate by analysis of hospital files. Physical examination included anthropometric variables, blood pressure, and testicular examination. Biochemical tests targeted glucose homeostasis, C-reactive protein (CRP), 25-OH vitamin D, zinc, and the hormones total testosterone (TT), free testosterone (FT), sex hormone-binding globulin (SHBG), estradiol (E2), thyroid-stimulating hormone, and thyroxin.
Sperm samples were collected in a clean container through masturbation, 2–5 days after sexual abstinence, liquefied for 30 min at 37°C, and sperm morphology was subsequently assessed by light microscopy at a final magnification of 1000 × . Smears were prepared from a 10 μL well-mixed drop of semen, air dried, and fixed by incubation for 1 h with ethanol (2/3) and acetic acid (1/3), before Shorr staining. All procedures were carried out in a single center specialized in human reproduction by an experienced professional. General findings were interpreted in agreement with the 2010 World Health Organization guidelines,2,3 and morphology was assessed according to Auger's classification. 4 As photographic images of sperm aberrations are already available,2,4 they were not included in the protocol.
Statistical analysis
Normally distributed variables (Kolmogorov–Smirnov) were compared by analysis of variance and posthoc Bonferroni test using log transformation when appropriate. The Chi-square test was used for discrete variables. Univariate and multivariate regression analyses of clinical and biochemical variables were conducted. Sample size estimation indicated that 22 participants in each group would be required to demonstrate an effect size of 35% in the main outcome variable (sperm morphological aberrations), using a type 1 error rate of 0.05, and a power of 0.8. SPSS® version 17 (IBM, Armonk, NY) was used, and differences were considered significant when p < 0.05.
Results
Demographic and nutritional findings
The age and body mass index (BMI) of all populations were matched, with the exception of Group 1 (higher age) and Group 4 (lower BMI), as expected. No patient was addicted to alcohol or drugs, and only in Group 1 were a significant proportion of tobacco addiction (p < 0.01) and obstructive sleep apnea identified (p < 0.01).
Preoperatively, Group 1 patients were heavier than Group 2 patients (59.8 ± 12.2 and 49.7 ± 7.6 kg/m2; p < 0.01) and, postoperatively, both groups had a weight loss of about 71% of excess weight (24.8 ± 10 and 17.6 ± 6.3 kg/m2). By the time of the study, both populations were in the obese range, without differences (35.1 ± 7.7 and 32.2 ± 5.5 kg/m2, not significant [NS]) (Table 1).
Sig., significance; BMI, body mass index.
General biochemistry and hormones
Fasting blood glucose, plasma lipid fractions, liver enzymes, CRP, white blood cell count, and thyroid hormones exhibited relatively minor differences among the groups (Table 2).
HDL, high-density lipoprotein; SHBG, sex hormone-binding globulin.
TT (p < 0.01), FT (p = 0.03), and SHBG (p < 0.01) were remarkably higher in operated participants (Groups 1 and 2) than in the lean and obese controls. The same occurred with E2 (p = 0.006) (Fig. 1); however, elevated values were registered as well in obese controls (Group 3), with a normal range only for Group 4 (Table 2).
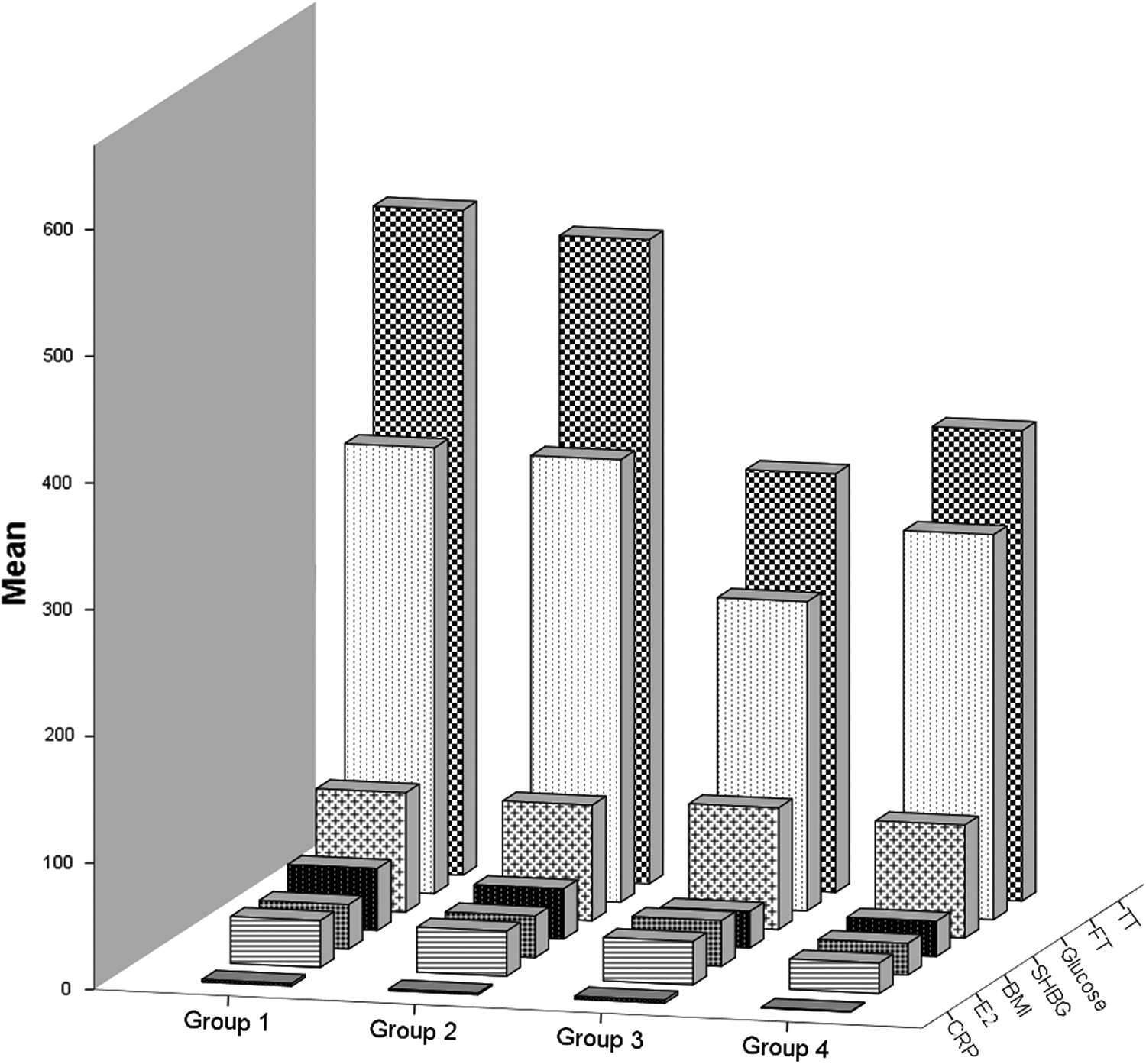
Demographic, sex hormones, biochemical and inflammatory profile of the studied populations. TT, total testosterone; FT, free testosterone; SHBG, sex hormone-binding globulin; E2, estradiol; CRP, C-reactive protein; BMI, body mass index.
Sperm parameters were normal in 42.9% of recently operated men, 66.7% of obese controls, and 80.0% of lean controls (NS). Among the semen abnormalities observed in the bariatric population, oligoasthenoteratospermia was documented in 14.3%, oligospermia, asthenospermia, teratospermia, and oligoasthenospermia occurred in 9.5% each, and azoospermia in 4.8% (Fig. 2). BMI positively correlated with oligoasthenoteratospermia (p = 0.008).
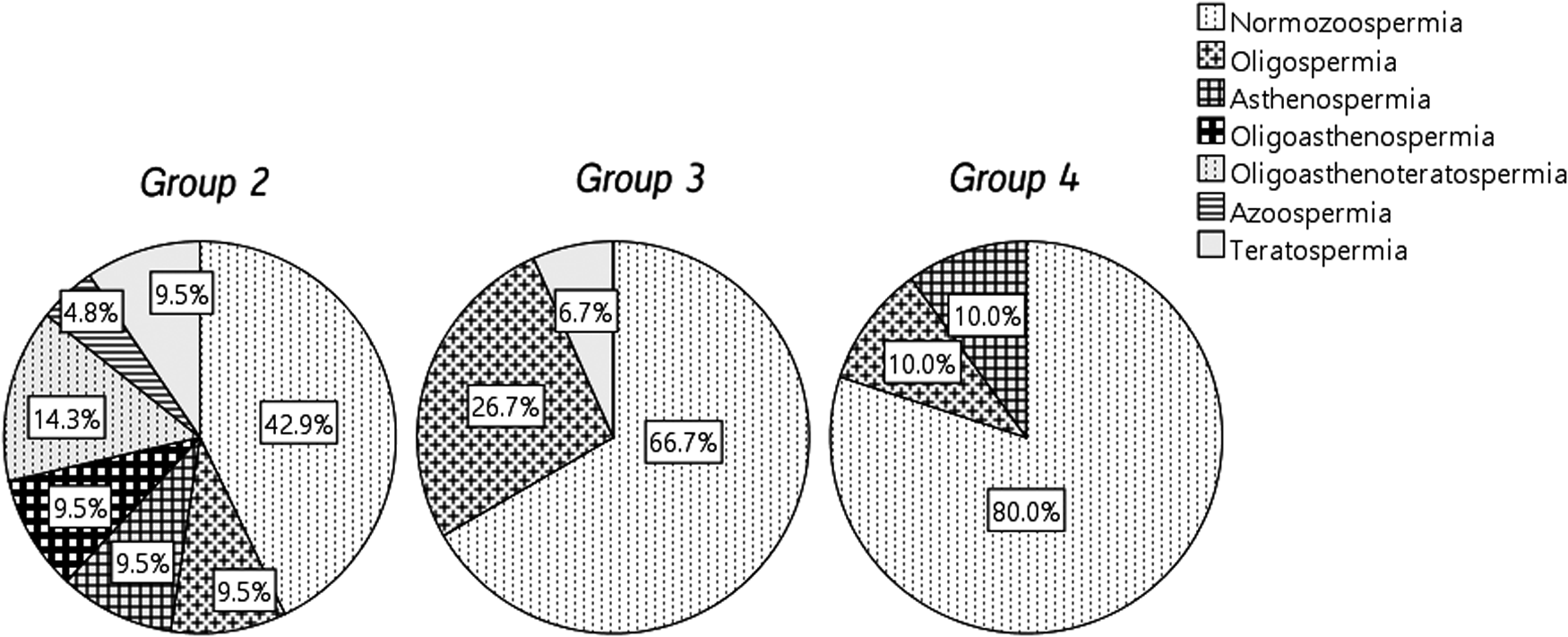
Semen parameters of the studied groups. 2
Fertile bariatric men, who had fathered a child before surgery, were 13.0%. This proportion was reduced to just one participant (1/23, 4.3%) after the bariatric intervention, without statistical difference concerning the obese population (21.4%) or lean controls (12.5%, NS). Gonadal status was not different among the groups, nor did it correlate with fertility or semen quality.
Vitamin D concentration, available in all groups except Group 1, was in the insufficiency range (<30 ng/mL), compared with lean controls who had normal levels. It negatively correlated with BMI (R2 = 0.325; p < 0.01). Zinc was acceptable in all groups and failed to exhibit significant correlations (Table 2).
Both bariatric populations (Groups 1 and 2) displayed higher SQOL-M scores after operation than the preoperative findings, without statistical differences regarding controls.
Discussion
Sperm count correlation with BMI has been defined as a J-shaped curve. 5 Abnormally low BMI is a milder drawback than obesity, as only this last abnormality was conspicuously associated with oligozoospermia and azoospermia.
In a retrospective study tracing >20,000 planned pregnancies, Nguyen et al. 6 reported that the odds ratio for infertility was 1.20 for overweight and 1.36 for obese men compared with those with low–normal BMI (20.0–22.4 kg/m2). Also Ramlau-Hansen et al., 7 after analyzing BMI and waiting time to pregnancy (TTP) of 47.835 couples, demonstrated a relationship between increased BMI and subfecundity (TTP of more than 12 months).
Analysis of bariatric surgery and semen parameters has shown conflicting results (Table 3). Reis et al. 8 and Legro et al. 9 found no significant differences in sperm characteristics postoperatively, whereas di Frega et al. 10 were alarmed by the observance of secondary azoospermy and complete spermatogenic arrest, in occasional circumstances, despite normal levels of circulating androgens.
LM, lifestyle modification; TT, total testosterone; FT, free testosterone; PRL, prolactin; FSH, follicle-stimulating hormone; SQL, sexual quality of life; RYGB, Roux-en-Y gastric bypass; AR, assisted reproduction; SG, sleeve gastrectomy.
Also Sermondade et al. 11 reported severe worsening of semen parameters (including oligoasthenoteratozoospermia) in three men, shortly after bariatric treatment, normalization occurring in only one subject, 24 months postoperatively. In the experience of Lazaros et al., 12 deteriorated semen variables were registered in two males 12–18 months after bariatric intervention. This condition negatively influenced the assisted reproduction outcome of the corresponding couples.
Recently, the sex hormone profile and semen characteristic of 46 patients, before and after sleeve gastrectomy, were analyzed. 13 Testosterone increased, and a trend toward semen improvement was noticed. Patients with preoperative azoospermia and oligospermia were benefited. However, no conclusion could be drawn regarding long-term effects.
This study confirmed that postoperative weight reduction was associated with increased androgens, in agreement with our previous findings. 14 Nevertheless, E2 levels persisted higher in bariatric patients, without significance between operated groups (p > 0.05).
Altered semen characteristics correlated with BMI, and although bariatric surgery was effective in improving male hormones, semen parameters were apparently refractory. More than 50% of bariatric patients displayed semen abnormalities, with a more disadvantageous pattern than obese controls. In addition, only one (normospermic and normogonadal) bariatric patient fathered a child after surgery, which could suggest a reduced testicular function of these individuals.
In common with our semen results, RYGB was the surgery performed in other studies reporting semen aberrations (Table 3). RYGB surgery, a restrictive and malabsorptive procedure, is believed to be associated with more severe nutritional consequences, 15 including deficits of several vitamins and trace elements. 16 Therefore, it is not unlikely that nutrient deficiencies could have exerted a deleterious influence on semen quality.
Bariatric patients receive a restricted, liquid diet during the first 30 days, followed by a balanced, dietitian-guided solid diet. A multivitamin, multimineral oral supplement is prescribed for daily use, as recommended by all professional societies. Compliance with the supplement is not perfect in any part of the world, and especial attention to vitamin D and zinc could be justified. However, there is little consensus about the optimal supplementation dose in the bariatric population, notably of vitamin D. 17
In experimental and clinical investigations, vitamin D deficiency alters reproductive function, possibly influencing sex hormone signaling, and the fertilizing ability of human sperm.18,19 Moreover, vitamin D acts as a regulator of several enzymes involved in steroid hormone production, including aromatase cytochrome P450 activity in osteoblasts.20,21
Secondary and compensated hypogonadism also tend to be associated with vitamin D deficiency. 22 In the current experience, hypogonadism was reversed after bariatric surgery, but not the insufficient vitamin D results.
Limitations and strengths of our study
Semen analysis was not performed preoperatively in our bariatric patients because of technical reasons, nor could it be conducted in those with long-term follow-up (group 1), because of age constraints. This limitation was addressed by including obese and lean nonoperated men, with paired age and BMI, as controls for preoperative and late postoperative participants. Sperm chromatin integrity was not part of the protocol, as the interest of the DNA fragmentation index in this context is still questioned. 23
The strengths of our investigation were the long follow-up period, the use of double controls, and the documentation of pertinent nutrients, namely vitamin D and zinc, which could play a role in the reproductive health of obese men.
Conclusions
Semen abnormalities were observed after bariatric surgery, and they were more severe than in nonoperated obese controls, although without statistical significance. Still, postoperative fertility was neither abolished nor improved. Androgen levels recovered after RYGB surgery and remained elevated in the long term. It is, therefore, unlikely that hypoandrogenism played a role in poor semen quality of bariatric men. General metabolism and glucose homeostasis also benefitted from the bariatric intervention, and these variables were probably not involved with reproductive troubles. No significant complaints concerning erectile function and SQL were registered; therefore, these should not be blamed for the apparent subfertility of bariatric men.
Estrogen levels did not diminish after operation, and remained in the same range as in nonbariatric obese controls. Consequently, involvement with semen aberrations cannot be ruled out. Other possibilities that deserve consideration in future studies are nutritional derangements such as vitamin D deficiency, mitochondrial DNA damage, and epididymal function abnormalities.
Footnotes
Acknowledgment
A Postdoctoral Grant (CAPES, PNPD20131663–USP/3300201022P2—Brazil) to A.R. is gratefully acknowledged.
Author Disclosure Statement
The authors declare no conflict of interest. All listed authors substantially contributed to the article. The article was read and approved by all authors, and it was submitted only to Bariatric Surgical Practice and Patient Care.