
Abstract
Background/Aim of Study:
Identifying the effect of adherence to a routine postoperative follow-up program on weight loss after surgery.
Methods:
Eighty-six patients who underwent a bariatric procedure were included. According to their compliance to follow-up visits, patients were classified into two groups: the Drop-Out group (patients who did not attend the follow-up appointments n = 45) and regular follow-up group (patients compliant with their scheduled postoperative appointments n = 41). Both groups were compared in terms of weight loss at four fixed time points: time of operation (T0), next to last (T1), last follow-up appointments (T2), and time of interview (T3).
Results:
Weight decreased in the time interval between T0 and T2 without a significant difference between both groups. A significant difference, however, was observed during the time interval T2 to T3, as weight continued to decrease among the regular follow-up patients versus a rise within the Drop-Outs patients (62.7 ± 24.1% vs. 49.9 ± 22.9%; p = 0.014).
Conclusion:
Adherence to a follow-up program is crucial to improve and sustain weight loss.
Background
A
The published evaluations with respect to weight loss after different bariatric procedures may be overestimated. This may be attributed to the fact that most published case series are based upon patients who attended the postoperative follow-up program. The corresponding data series did not analyze the results of patients who did not adhere to the follow-up program. 4
Several published studies confirmed the fact that a large number of patients are lost to follow-up programs (up to 49%),5–8 so called Drop-Outs. Such a limitation casts a shadow over the reliability of the results on long-term weight loss of bariatric procedures as many studies take into consideration only patients who attended the follow-up.
Some studies compared both patients' groups and reported that patients who regularly attended their postoperative appointments had better results in percentage of excess weight loss (%EWL) compared to those who failed to attend follow-up.9–11
However, all previously published data focused only on the percentage of weight loss as the main point of evaluation, mainly at a certain single time point at the end of the study, and did not take into consideration other outcomes such as QOL.
This study was aimed to identify the effect of adherence to a routine postoperative follow-up program (regular follow-up) in comparison to patients who failed to attend their scheduled follow-up visits for more than 12 months (Drop-Outs). This was done in terms of weight loss and improvement of QOL after surgery.
Methods
Included are all patients who underwent bariatric surgery at the University Medical Center between January 2003 and December 2010.
To examine the long-term effect of follow-up programs, only patients with a minimal time interval of 18 months after the operation are included. Patients who were not able to attend the follow-up programs because of compulsory reasons such as pregnancy or movement to a new address are excluded.
The research protocol was approved by the Institutional Review Board and all subjects gave consent to participate.
Our postoperative follow-up program included consultation with the surgeon and nutritionist and a bioelectrical impedance analysis on the same day. Follow-up visits were scheduled at the outpatient clinic 10 days after surgery for stitch removal, then thrice every 6 weeks, twice every 3 months, twice half yearly, and then once every year thereafter. At each visit, the next appointment with the patient was scheduled.
Based on the above criteria, 132 patients were initially included. We were able to contact, by telephone, 113 patients (85.6%) who accepted to participate in our study. The other 19 patients (14.4%) were not reachable, refused to participate, or were dead.
The 119 patients included in the study received four different bariatric procedures, namely SG (sleeve gastrectomy) (26), RYGB (Roux-en-Y gastric bypass) (65), LAGB (adjustable gastric banding) (7), and BPD (biliopancreatic diversion with duodenal switch) (15).
To better assess the impact of patients' adherence to our postoperative follow-up program, patients were further classified into two groups: regular follow-up and Drop-Out patients.
Drop-Out patients (control group) were defined to be patients who did not attend the follow-up appointments for more than 12 months.
The reason for choosing 1 year is that this is the maximum period of patient's follow-up absence that can still achieve a satisfactory postoperative control (German guidelines). 12
However, patients during the third postoperative year are appointed yearly for follow-up. For these patients, the period of absence was extended up to 15 months.
In the Drop-Out group of patients, we reported actual weight at time of phone interview and at time point of last and next-to-last appointment.
The second group, namely regular follow-up patients, was defined to be those who followed their scheduled postoperative outpatient appointments.
To correctly compare both groups in terms of weight loss, the time interval between the operation and the three reference time points (time of phone interview and time of last and next-to-last appointments) has to be similar.
To achieve this, we calculated the median time interval between the operation and the next-to-last appointment (9.9 months) as well as between the operation and the last appointment (14.6 months) for the Drop-Out group.
Then, we included, for our analysis, patients from the follow-up group (45 patients out of total of 86) with full available data at these three comparable fixed time points, namely time of operation, at 9.9 months as reference to next-to-last appointment, and at 14.6 months as reference to last appointment (Fig. 1).
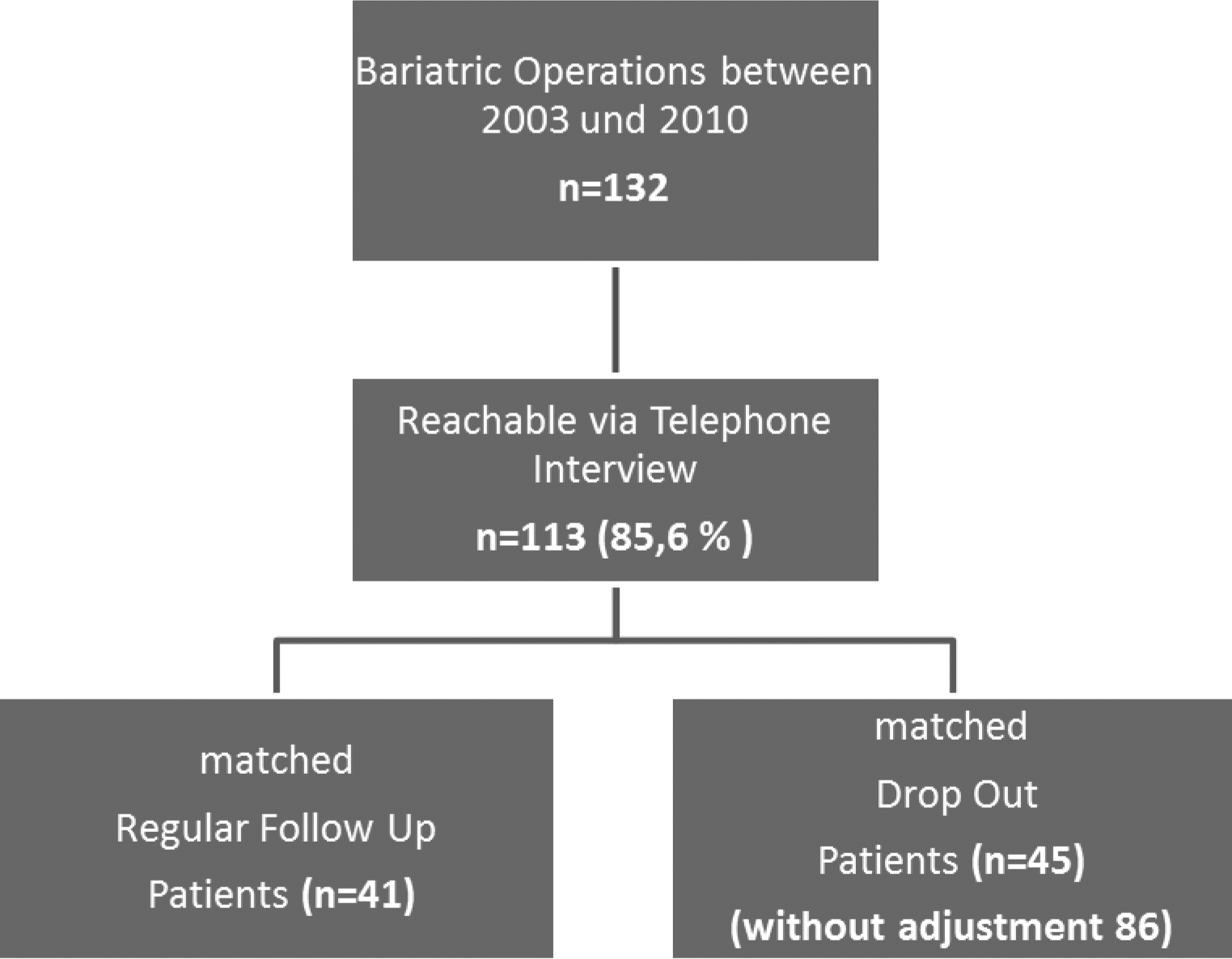
Distribution of study population into subgroups.
During the phone interview, the following data were collected and calculated: actual weight, %EWL, and %TWL (total weight loss).
Participants were requested to answer a range of questions. The German version of the bariatric QOL index questionnaire was used as it is validated (40). It evaluates the patient's subjective impression of his/her QOL, both in terms of psychological well-being as well as social and physical functionality.
The questionnaire consists of 13 questions. Each answer is assessed by a point scale from 1 to 5 that are in the end summed up giving a maximal value of 65 points and a minimal of 13 points. This questionnaire was previously implemented by the authors in the same group of patients to compare the impact of four different bariatric procedures (RYGB, SG, LAGB, and BPD) on QOL after surgery. The result of the questionnaire showed, in this respect, no significant difference between the different operations.
Statistical analysis
The data were evaluated using the statistical program SAS, version 9.3 (SAS Institute, Cary, NC). Quantitative variables were given as mean and standard deviation (in most cases, including median, minimum, and maximum, to facilitate comparison with the data from other studies). If appropriate, the absolute number plus the percentage was also included.
For the comparison of two mean values, the t-test was used, as far as normal data were concerned. In the case of nonnormalized data, the Mann–Whitney test was used as a nonparametric method. The correlation coefficient according to Pearson was used for the correlation analysis. Simple number comparisons were performed with the Chi-square test (Fisher's exact test). The significance level was adjusted in all cases with p < 0.05.
Results
The study included 86 patients (30 males and 56 females). The average age of our total population was 47.4 ± 11 years. The mean preoperative body mass index (BMI) was 49.2 ± 6.4 kg/m2. The median time interval between operation and time of interview was 38 ± 18.8 months.
There were 41 patients (47.7%) in Group A (regular follow-up) and 45 patients (52.3%) in Group B (Drop-Outs). The patients in each group did not differ in terms of age, gender, or initial BMI.
Data of both patients' groups were collected, recorded, and compared at four fixed time points adjusted according to the Drop-Out groups: time of operation (T0), next to last (T1), last follow-up appointments (T2), and time of interview (T3).
Weight loss
BMI, %EWL, and %TWL were tracked and compared between both groups.
A significant decrease of mean BMI was observed among both patients' groups from T0 through T1 up to T2. BMI fell from 50.1 ± 6.1 to 32.9 ± 6.2 kg/m2 in the regular follow-up patients and decreased from 47.6 ± 5.6 to 33.8 ± 4.9 kg/m2 among the Drop-Out patients (control group). Nevertheless, the difference between the two groups during the time interval between T0 and T2 was not statistically significant.
However, further tracking of mean BMI during time interval between T2 and T3 showed a decrease among the regular follow-up patients versus an increase in the Drop-Outs (control group). Difference between both patients' groups was statistically significant (32.3 ± 6.5 kg/m2 vs. 34.9 ± 6.2 kg/m2; p = 0.05) (Fig. 2).
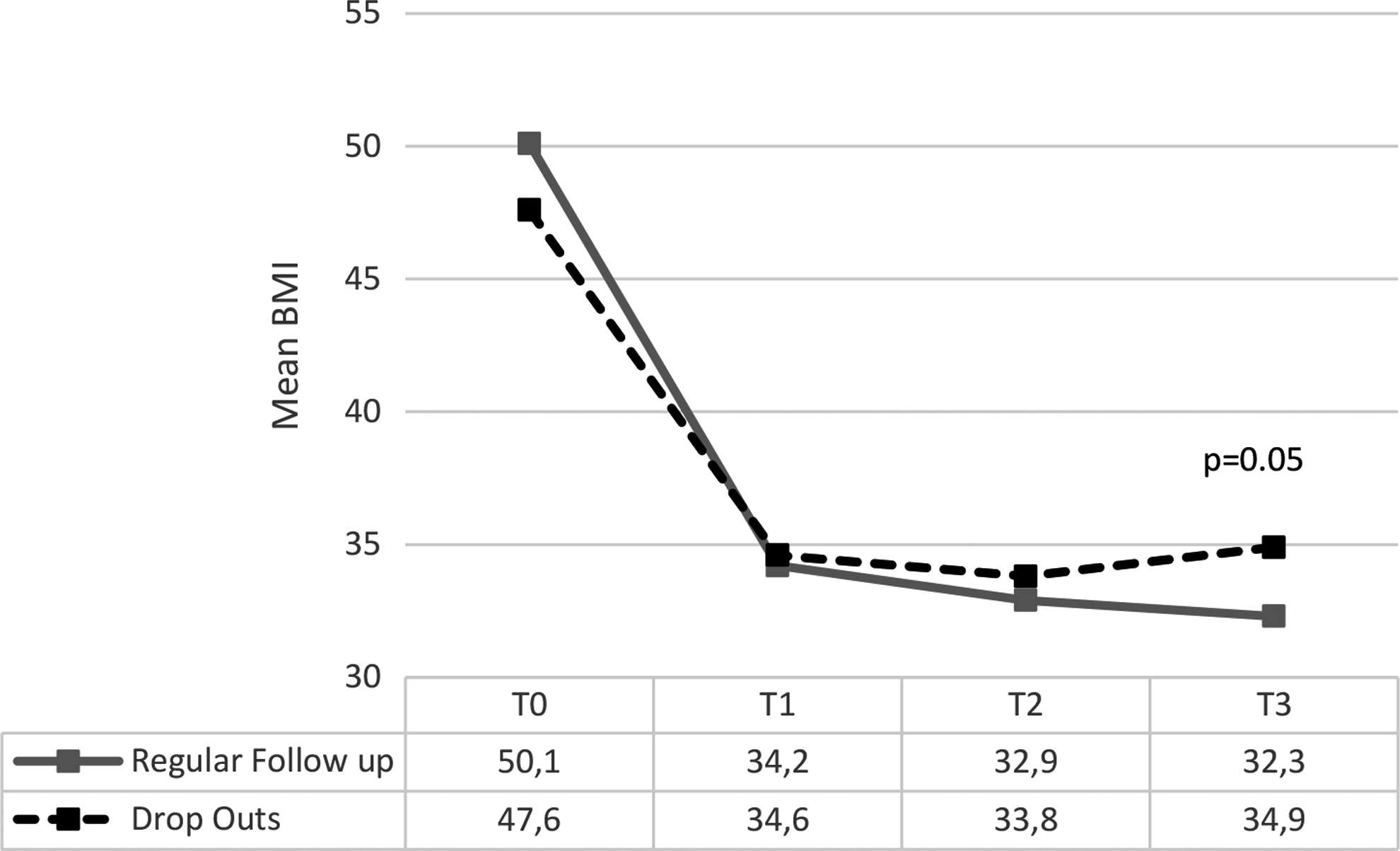
BMI changes in regular follow-up group and Drop-Out group. BMI, body mass index.
Similarly, %EWL and %TWL decreased in the time interval between T0 and T2 without a significant difference between both groups.
However, also for these measurements, %EWL continued to decrease among the regular follow-up patients versus a rise within the Drop-Out patients (control group) during time interval between T2 and T3. The difference in %EWL between follow-up and Drop-Outs at time point T3 (interview) was strongly significant (62.7 ± 24.1% vs. 49.9 ± 22.9%; p = 0.014) (Fig. 3).

Percentage of EWL (excess weight loss) in regular follow-up group and Drop-Out group. EWL, excess weight loss.
Similar results were recorded in %TWL in the time interval T0–T2 and T2–T3 (Fig. 4).
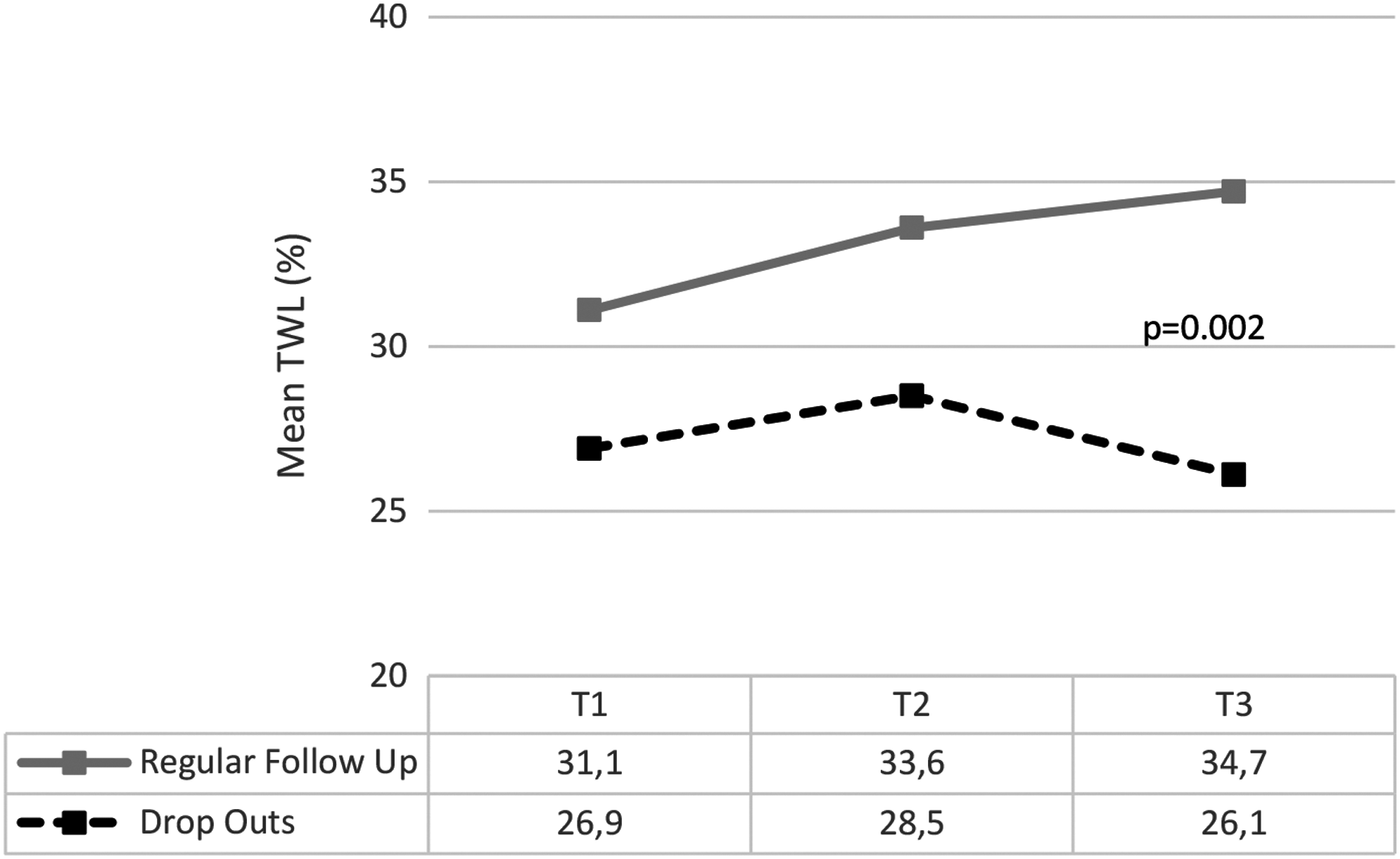
Percentage of TWL in regular follow-up group and Drop-Out group. TWL, total weight loss.
Quality of life
Mean QOL score using bariatric QOL (BQL) index questionnaire was higher among regular follow-up patients than Drop-Outs, yet did not reach a statistical significance (51.9 ± 11.0 vs. 50.0 ± 10.4; p = 0.257).
Discussion
Importance of follow-up
Follow-up after bariatric surgery is important to assess outcomes, such as weight loss, resolution of obesity-related comorbidities, and early identification of vitamin deficiencies or malnutrition. Also, postoperative complications such as anastomotic stricture, overtight LAGB, Dumping Syndrome, hernias, and anorexia affect the result of the patients.
Moreover, bariatric patients usually require dietary or lifestyle recommendations.
Adherence to regular complete bariatric aftercare programs is not satisfactory. 13 Also, Puzziferri et al. pointed out in his systematic review that <3% of bariatric studies included >80% long-term follow-up. 14
Causes of noncompliance
Several studies reported that greater distance to the clinic and greater patient's initial BMI are associated with a higher rate of attrition.13,15 However, Moroshko et al. did not find, in his review of relevant literature, any consistent predictors of attrition across the eight available studies. 13
Larjani et al. examined preoperative predictors of adherence to follow-up care after surgery. He identified employment as the strongest predictor of attendance to follow-up clinic. Also, patients with obstructive sleep apnea and older patients were more compliant to return for scheduled follow-up. 16
Patients in this study received the same offer of our free of charge follow-up program and always got fixed follow-up dates. Nevertheless, some patients stop participating. Male patients were more likely to avoid scheduled follow-up appointments than female patients. Among the Drop-Outs, 70% were men (p = 0.023). The time elapsed since the operation appeared to be another predictive parameter of avoiding follow-up; the longer the period after surgery, the more likely to Drop-Out (33.6 months in regular follow-up vs. 47.7 months in Drop-Outs, p = 0.003). Other factors like age and preoperative BMI did not play a role.
Follow-up and weight loss
Several other studies tested the effect of follow-up visits on weight loss after bariatric surgery. Harper et al. reported a higher %EWL in patients after laparoscopic gastric bypass who returned for their annual appointment without repeated notification than the group of patients who did not automatically return for their annual appointment (76% vs. 65%; p < 0.003). 8
Shen et al. examined the impact of attending half of the scheduled clinic appointments on weight loss after laparoscopic adjustable gastric band (LAGB) and laparoscopic gastric bypass procedures. Results suggested that patient's follow-up during the first year plays a significant role in the amount of weight lost after LAGB, but not after RYGBP. This was attributed to the frequency of band adjustment. 9
In contrast to this, the majority of patients included in our study received SG or RYGB, and our results demonstrate the advantage of adherence to a routine postoperative follow-up program, in particular for these two operations. If all operations should be included in a follow-up program the same way, could not be answered by our results, but patients after SG or RYGB seem to profit.
To determine the relationship between the length of follow-up and EWL after LRYGB, Gould et al. divided patients into three groups: first group consisted of patients who had attended every scheduled postoperative appointment up to 3 years, the second one of patients who attended every appointment, but only for 1 year, and third group of patients who had already been stopping follow-up during the first year after surgery. Interestingly, weight loss did not differ at 1 year of follow-up. However, a significant difference in the EWL was observed at 3 to 4 years (74% for group 1 vs. 61% for group 2 vs. 56% for group 3; p < 0.05). 10
In this study, we clearly provide evidence on the effect of adherence to scheduled follow-up program in terms of weight loss.
Our patients in both groups lost weight to a similar extent as long as they were adhering to the follow-up till time point T2 (last appointment). Afterward, however, the difference in weight loss between both groups started to become noticeable. %EWL and %TWL continued to rise among regular follow-up patients, while at the same time started to decrease in Drop-Out patients.
This trend became more evident at the time of the interview (T3) at which %EWL and %TWL were 62.7 and 34.7 in the follow-up group versus 49.9 and 26.1 in the Drop-Out group, respectively (p = 0.01, 0.02).
Regarding the weight loss, two assumptions may be postulated to explain why patients who did not come to the postoperative appointments after T3.
First, the patients were doing well and decided to ignore attending their scheduled visits because they felt that follow-up is unnecessary and thus started to gain weight.
Second, patients were not satisfied with their weight loss after the surgery and felt embarrassed to return to follow-up.
Detailed analysis of our results at fixed time points clearly suggests the first assumption as an explanation of the patients' noncompliance behavior and weight regain. Drop-Outs had comparable weight loss to follow-up patients until the time of their nonadherence to bariatric aftercare.
Some authors attributed poor compliance with follow-up program to unsatisfactory weight loss until Drop-Out. However, our results showed that this conclusion seems not to be true. Harper et al. 8 compared patients' adherence to follow-up after both gastric banding and RYGB. Despite lesser EWL, patients with gastric bands were more compliant to attend their scheduled appointment follow-up rather than RYGB.
Our study highlights the importance of patients' adherence to a scheduled follow-up program after surgery. Patients attached to follow-up benefit from surveillance, counseling, and dietary and lifestyle recommendations and modifications continuously offered by their bariatric team.
Follow-up and QOL
Attendance of follow-up visits did not alter the QOL of both patient groups after surgery. This may be attributed to the fact that even patients of the Drop-Out group did in fact reduce weight after surgery compared to preoperative weight. However, a longer follow-up may be required for a difference between both groups to elaborate.
Weight loss surgery is an excellent option that provides a new start for morbidly obese patients to achieve sustained weight loss and improve QOL. However, patients need to know that surgery alone, without a follow-up program, is not enough to help lose weight and keep it off. 17
Tracking the weight changes over a period at fixed time points is a key strength of this article. Plotting the relationship between patients' weight and adherence to scheduled visits over time clearly yielded the conclusion that avoiding follow-up leads to reduced weight loss after surgery.
This study is not without limitations. Answers of the implemented questionnaire were self-reported by the patients themselves through a phone interview, without being confirmed by physical measurements. Second, no randomization was done.
In addition, the time frame of postoperative observation may still be too short. A future study with longer follow-up may be required to confirm the findings and needs to focus on the metabolic parameters and clinical comorbidities.
Conclusion
Adherence to follow-up program is crucial to improve and sustain weight loss. Every effort should be done to contact patients who are lost to follow-up before they start to regain weight. Financing of the aftercare is necessary to optimize postbariatric weight loss.
Footnotes
Author Disclosure Statement
No competing financial interests exist.