
Abstract
Background:
Bariatric surgery patients are at a higher risk for venous thrombotic events. Inferior vena cava filter (IVCf) placement to prevent thrombotic complications is still considered controversial in bariatric surgery patients, especially when left in place long term. In this study, we describe our experience with the use of retrievable IVCf and their safety in bariatric surgery patients.
Methods:
A retrospective chart review was performed in a single bariatric surgery center. Patients with a body mass index (BMI) greater than 50, with a history of thromboembolic events, hypercoagulable conditions, and low mobility were defined as high risk and underwent exclusively retrievable IVCf placement. All also received preoperative heparin and postoperative low-molecular weight heparin prophylaxis. All patients underwent venogram during the filter retrieval.
Results:
Forty-nine patients, 36 females and 13 males, were reviewed. Mean age was 48, mean BMI was 53.7. Thirty-five patients underwent laparoscopic gastric bypass, 8 laparoscopic gastric banding, and 5 laparoscopic sleeve gastrectomy. 54.1% of patients received retrievable inferior vena cava filter (rIVCF) for a BMI >50 (n = 26); 27.2% for a personal history of deep venous thrombosis (DVT)/pulmonary embolism (PE) (n = 13); 6.2% for a family history of DVT/PE (n = 3); 8.3% for known hyper coagulable state without prior DVT/PE (n = 4); and 4.2% for low mobility or immobility (n = 2). Forty-eight patients out of 49 successfully received rIVCF. 98% of filters (47 out of 48) were removed successfully without any complications. One patient did not return to follow-up. One patient developed nonfatal DVT and PE, while the filter was still in place. There were no complications from filter placement or removal.
Conclusions:
The use of retrievable IVC filters for the prophylaxis of venous thromboembolism in bariatric surgery in conjunction with chemoprophylaxis therapy is safe and effective.
Introduction
B
There is strong evidence in the literature that obesity is associated with increased risk of VTE. 2 Obesity interferes with both coagulation pathways, as well as with the anticoagulant mechanism, leading to a hypercoagulable state. 2 Perioperative factors such as surgical trauma, operative duration, anesthesia, and pneumoperitoneum likely increase this risk.3,4
VTE is associated with high morbidity and mortality and is cause of more than 2,50,000 hospital admissions annually in the United States, 2 making it a feared postoperative complication. The incidence in average risk bariatric surgery patients is 1.3% for DVT and 1.1% for PE.3–5 In patients defined at high risk, the incidence increases to 5.4% for DVT and 6.4% for PE.6–9 Factors that increase risk include body mass index (BMI) >50, truncal obesity, advanced age, personal or family history of VTE, known hypercoagulable state, immobilization, venous insufficiency/stasis, smoking, use of estrogen containing oral contraceptives and hormone replacement therapy, and the comorbidity of obesity-hypoventilation syndrome.10,11,12
In our study, we describe our experience with the use of retrievable inferior vena cava filter (rIVCF) and hypothesize their safety and efficacy in high-risk bariatric surgery patients for the routine prophylaxis of VTE.
Methods
Study design, settings, and patient population
In this retrospective report of case series, we evaluated the safety and the clinical outcomes of rIVCF placements in high-risk bariatric surgery patients. The center where the study was performed is a 247 bed academic hospital with 4 surgeons who routinely perform bariatric surgery and a well established vascular surgery service. To be included in the study, patients must have at least one of the following characteristics: BMI >50; nonambulatory patient or impaired ambulatory status; history of DVT or PE; family history of DVT or PE; severe pulmonary hypertension; and hypercoagulable state. All filters placed were retrievable in design. Patients underwent rIVCF placement surgery within 14 days of the anticipated bariatric surgery (Fig. 1).
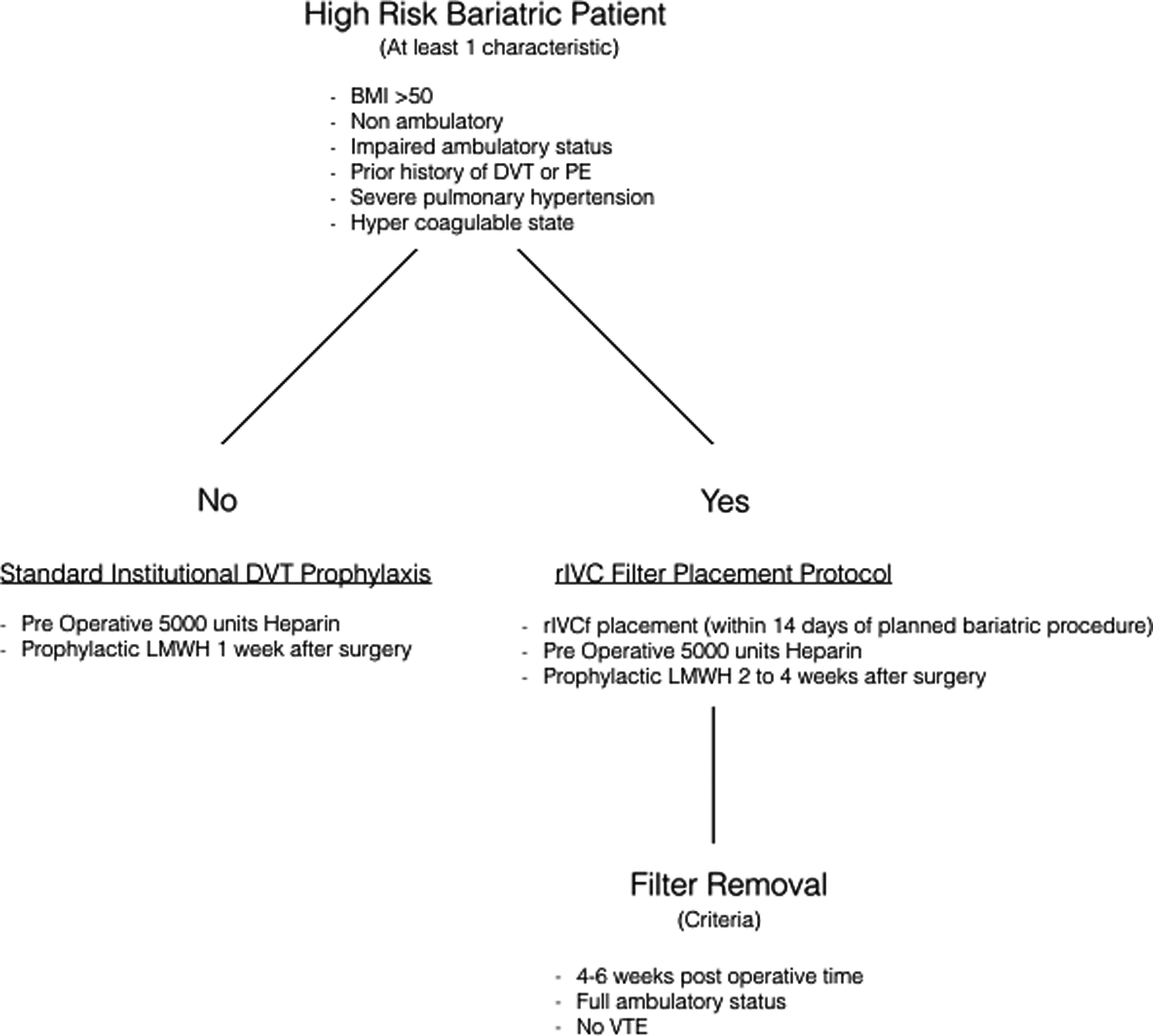
VTE prophylaxis protocol used at our institution. Patients considered high risk for VTE for bariatric surgery are enrolled in the rIVCF placement protocol and receive the filter within 14 days of the planned bariatric procedure. Everyone receives 5000 units of subcutaneous heparin preoperatively and prophylactic LMWH 2–4 weeks after surgery. Specific criteria have to be met in order for the filter to be removed, such as 4–6 weeks postoperative time, full ambulatory status, no clinical evidence of VTE. rIVCF, retrievable inferior vena cava filter; LMWH, low-molecular weight heparin; VTE, venous thromboembolism.
All patients considered high risk for undergoing bariatric surgery from December 2008 until July 2015 were enrolled in the study. Operations performed were laparoscopic gastric bypass (LGB), laparoscopic gastric banding (LGb), and laparoscopic sleeve gastrectomy (LSG). No revision surgeries were included. Preoperative heparin on the day of surgery (single dose of 5000 units subcutaneous) and prophylactic low-molecular weight heparin (LMWH) for 2–4 weeks postbariatric surgery (60 mg twice a day) were administered to all subjects. LMWH was given for 4 weeks when patients had a personal history of DVT/PE and/or immobility. All patients received Thromboembolism Deterrent Stockings (TEDs) and sequential compression devices (SCDs) intra- and postoperatively and were encouraged to ambulate in the immediate postsurgery period. Criteria for filter removal were as follows: 4–6 weeks postoperative time frame; full ambulatory status; and no thromboembolic (VTE) complications. Imaging studies were performed on patients only when clinical suspicion was present to detect DVT/PEs pre- or postoperatively. Review of the medical record, discharge summary, and office progress notes were used to validate the appropriateness of study enrollment. Pediatric patients, patients with incomplete medical records, and nonhigh-risk bariatric patients were excluded.
Operative technique of rIVC placement and removal
In this group of patients due to body habitus, the rIVC filters were placed through the right internal jugular route and similarly removed through a right neck puncture. This was all performed using direct visualization through ultrasound followed by fluoroscopy. In filter placement, the most important steps were to visualize the renal veins to ensure infrarenal placement and proper positioning to mitigate filter tilt. Filter retrieval was done percutaneously using the company-specific retrieval kits, first, ensnaring the filter hook and subsequently swallowing the filter over the sheath to disengage the tines from the IVC wall. Pressure hemostasis was performed over the right neck puncture site and reinspected for bleeding in the perioperative period, which is important in the settings of possible anticoagulation.
End points
The primary outcomes were the safety of the rIVCF placement, the complication rate of both implantation and explantation such as breakage, perforation, and insertion site hematoma, infection, and the rate of retrieval. Low complication and high retrieval rates would suggest the safety of the technique, which could then potentially lower the incidence of postoperative VTE events in this high-risk subpopulation. Secondary outcomes were failure of placing rIVCF and VTE event rate.
Results
A total of 49 patients were enrolled in the study, 36 females and 13 males. All patients underwent bariatric surgery for Class III or IV obesity. Mean age was 48 and mean BMI was 53.7. Thirty-five patients underwent LGB, eight LGb, and five LSG. 54.1% of patients received rIVCF for a BMI >50 (n = 26); 27.2% for a personal history of DVT/PE (n = 13); 6.2% for a family history of DVT/PE (n = 3); 8.3% for known hypercoagulable state without prior DVT/PE (n = 4); and 4.2% for low mobility or immobility (n = 2). No patients had pulmonary hypertension. Seven patients out of 49 had 2 high-risk factors: One patient had high BMI and prior DVT, 2 patients had high BMI and prior PE, 1 patient had prior PE and hypercoagulable state, 1 patient high BMI and family history of VTE, 1 patient had hypercoagulable state and family history of VTE, and 1 patient had high BMI and hypercoagulable state (Table 1).
BMI, body mass index; VTE, venous thromboembolism.
There were no differences in the yearly rates of rIVCF placement, likely due to the defined indications for the procedure that were upheld over the 7 years of the study. Forty-eight patients out of 49 successfully received rIVCF, while the procedure was aborted in 1 case due to technical difficulty. Thirty-four patients (69.4%) received the Cook Celect® rIVCF, 6 patients (12.3%) received the Cook Gunter Tulip® retrievable filter, 5 patients (10.2%) Bard Denali® rIVCF, 3 patients (6.1%) Bard Eclipse® rIVCF, and 1 patient (2%) Argon® rIVCF. All subjects received preoperative heparin, intra- and postoperative TEDs/SCDs and LMWH, which was continued per protocol for 2–4 weeks after surgery depending on personal history of DVT/PE or immobility. Mean duration of filter placement was 92 days with a median of 62.5 days. One patient with a history of DVTs sustained DVT and PE 31 days after surgery, while the filter was still indwelling. The thrombus was found below the level of the filter.
The PE was nonfatal and the patient received appropriate anticoagulation therapy with heparin and warfarin. The filter was eventually retrieved 213 days after insertion after the DVT/PE was medically treated. Upon retrieval, 27% of patients (n = 13) had a blood clot on rIVCF pathology report. 98% of filters (47 out of 48) were removed successfully without any complications, while 1 patient did not return to follow-up. There were no breakages, perforations, insertion site hematoma, or infections. There were no deaths or long-term complications caused by the procedure (Table 2).
rIVCF, retrievable inferior vena cava filter.
Discussion
VTE prophylaxis for bariatric surgery has been the topic of much discussion in the literature. Mechanical modalities to prevent VTE include graduated compression stockings, intermittent pneumatic compression devices, and venous foot pumps. Perioperative use of the above devices and early mobilization of patients reduce the risk of VTE by increasing venous outflow and preventing venous stasis. 13 Unfractionated heparin and LMWH are effective and well established means in the prophylaxis of VTE in surgical and bariatric patients.14,15 The prophylactic use of IVCF remains controversial, with a complication rate of 4–36% reported in the literature for permanent devices. 16 Adverse events include thrombosis, DVT, migration, tilting, infection, and erosion. For this reason, retrievable filters (rIVCF) were created.
While some studies report lower incidence of DVT and PE with retrievable devices, others suggest that while the risk of PE may be lowered, the DVT rates are higher; likely because many of these filters do not get removed (up to 65%) and/or patients are lost to follow-up.16–18 Also, by recent Food and Drug Administration (FDA) recommendations, all retrievable IVC filters should be removed within 60 days of implantation, underlining the importance of appropriate follow-up for early retrieval. 19 The risks and complications deriving from the implantation and explantation of such devices, such as breakage, perforation, insertion site hematoma, and infection should also be considered; it has been reported in the literature that longer indwelling time, especially if greater than 3 months, is associated with a higher incidence of failed retrieval due to technical difficulties. 20
Although placement of rIVCF has remained controversial in the literature, our experience shows that routine placement for bariatric surgery patients at high risk for VTE can be safe and effective. We were able to achieve high compliance and low complication rates at our institution. We attribute this to good communication with our vascular surgery team and excellent compliance with recommended follow-up visits, leading to the 98% rate of filter removal. This compares very favorably to what has previously been reported in the literature, where the best results for filter removal are around 30%. 19 Our only patient who was lost to follow-up moved out of state in the immediate perioperative period. Our median duration to retrieval of rIVCF is similar to the recent FDA recommendations for rIVCF removals of 60 days. 19 There were no technical complications with filter removal, which is most likely because early retrieval is associated with technical ease. 20
In our population, rIVCF patients were also treated with mechanical and chemical VTE prophylaxis, as would be done for our standard risk patients. This could have contributed to our population experiencing lower rates of VTE than expected. At our institution, our observed rate of VTE for all bariatric patients is 0.4% over the same study period of total of 746 patients. We typically give all patients with BMI >40 1–4 weeks of 60 mg of LMWH twice daily after discharge from the hospital. The dose of LMWH used and the duration of therapy are higher than many uses for VTE prophylaxis in bariatric surgery patients.
We had one VTE complication in our study group. This patient had the risk factor of personal history of DVT. He presented to the emergency department 31 days postoperatively with complaints of leg and chest pain. A DVT was found below the filter while still indwelling. The only patient with this VTE may have been saved from a fatal PE due to the presence of a large volume DVT below the rIVCF where the filter had a protective effect.
The clinical significance of the presence of a clot on retrieval pathology report on 27% of filters is unknown. This could be due to stasis at the level of the filter, indicating that the rIVCF is a nidus for thrombosis; alternatively, it could be the filter that is catching thrombus as it circulates, thus providing a protective effect. More study is needed on this subject.
This was a retrospective review of prospectively gathered data, which has its intrinsic limitations as a study design. There was no control group, which limits the significance of the conclusions.
Conclusions
In our experience, the use of retrievable IVC filters for the prophylaxis of VTE in bariatric surgery in conjunction with standard VTE prophylaxis therapy can be safe and effective. Multidisciplinary care and the importance of follow-up for filter retrieval are both essential for successful rIVCF therapy as well as high retrieval rates to limit its device-related long-term complications. We feel this procedure can potentially expand access to the benefits of bariatric surgery for those who are high risk for VTE and should be considered to decrease morbidity in this population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.