
Abstract
Objective:
The aim of this study was to compare the ultrasonography (USG) measurements of anterior neck soft tissue and other clinical screening tests used to evaluate difficult laryngoscopy in morbidly obese patients.
Materials and Methods:
A total of 130 morbidly obese patients were scheduled for laparoscopic bariatric surgery. USG examination was performed of the vocal cords, thyroid isthmus, and suprasternal notch.
Results:
Analysis was made of 74 patients. Difficult laryngoscopy was considered as grade 3 or 4 on the Cormack and Lehane scale. In seven (9.5%) patients the classification was made of difficult laryngoscopy. The incidence of difficult laryngoscopy was significantly higher in patients with older age, hypertension, and obstructive sleep apnea syndrome. Grades of ≥5 on the intubation difficulty scale, which is a requirement for a styleted endotracheal tube and a high number of intubation attempts, were found to be significantly higher in the difficult laryngoscopy group. Sternomental distances for difficult and easy laryngoscopy were 11.5 ± 3.75 and 14.18 ± 2.63 cm, respectively.
Conclusion:
USG measurements of the anterior soft tissue thickness of the neck remain debatable for the prediction of difficult laryngoscopy in the literature. The results of this study demonstrated that USG measurements of anterior neck soft tissue have no advantage in the determination of difficult laryngoscopy in morbidly obese patients scheduled for bariatric surgery.
Introduction
O
The scenario of “can't intubate, can't ventilate” position can occur in 1 in 1000 elective and 1 in 250 rapid sequence cases. 6 The preoperative anesthesia evaluation is recommended especially for airway assessment. There are many preintubation clinical screening tests but these are not sufficient to detect difficult laryngoscopy. A history of obstructive sleep apnea syndrome (OSAS), high Mallampati score, limited mouth opening (<3 cm), short thyromental distance (<6 cm), short sternomental distance (<12.5 cm), limited neck extension, prominent upper teeth, large neck circumference, and high body mass index (BMI) have been suggested as predictors of difficult laryngoscopy and intubation.7,8
Ultrasonography (USG) examination can be performed for measurement of anterior soft tissue thickness. However, the acceptance of only high USG measurements of anterior neck soft tissue for good prediction of difficult laryngoscopy remains debatable.9,10 Although the role of USG for airway assessment is not clear, its usage should be supported because USG is inexpensive and a rapid tool that can be easily performed. 11
The aim of the current study was to compare the USG measurements of anterior neck soft tissue and clinical screening tests for the determination of difficult laryngoscopy in morbidly obese patients undergoing bariatric surgery.
Materials and Methods
Written informed consent was obtained from each patient. The study protocol was approved by the local ethics committee of our institution and Australian New Zealand Clinical Trials Registry (Ref: ACTRN12617000532303). The study was conducted in accordance with the principles of the Declaration of Helsinki. This prospective, observational single-center study was conducted between May and August 2015 and included a total of 130 consecutive patients aged >18 years and morbidly obese (BMI >35 kg/m2) who were scheduled for laparoscopic weight loss surgery under general anesthesia with endotracheal intubation. Patients with upper airway pathologies (maxillofacial fracture, tumours, etc.), any pathology causing limitation in head–neck movement (cervical spine fracture, rheumatoid arthritis, ankylosing spondylitis, etc.), contraindication of general anesthesia (history of malignant hyperthermia, full stomach, etc.), or a history of difficult laryngoscopy or intubation were excluded from study. The degree of obesity was calculated according to the classification of the BMI which was determined with the formula of weight/height 2 (kg/m2).
Preoperatively, patients were evaluated by an anesthesiologist for the following clinical screening variables: BMI, history of OSAS, protruding upper teeth, thyromental and sternomental distance with the neck extended, temporomandibular joint mobility assessed by mouth opening and forward movement of the jaw, the ability to protrude the lower teeth further than the upper teeth, modified Mallampati score, Wilson risk total score, limited neck movement, and neck circumference measured at the thyroid cartilage. This anesthesiologist was not involved in the laryngoscopy procedure.
The USG examination was performed while the patient was in supine position, and the head was placed into mild extension. The patient was ordered to breathe slowly to avoid airway changes due to inspirium–expirium. USG measurement was performed from the mid-front part of the neck using a linear probe at a frequency of 10 MHz (EsaoteMyLab™ 30, Florence, Italy). The distance from the skin to the anterior aspect of the trachea was measured at three different levels: vocal cords (zone 1; Fig. 1), thyroid isthmus (zone 2; Fig. 2), and suprasternal notch (zone 3; Fig. 3). At each level, three measurements (central axis and ∼15 mm to the left and right of the central axis) were taken by another anesthesiologist who performed all the USG measurements one day before surgery, and three measurements were averaged to obtain the soft tissue thickness. Each patient taken to the operating room was monitored routinely for heart rate, peripheral oxygen saturation, noninvasive blood pressure, and end-tidal carbon dioxide. The patient was positioned with a pillow under the shoulders, with the head elevated and neck extended in the sniffing position. After 3 min of preoxygenation, anesthesia was induced with intravenous fentanyl (Talinat®; Vem, Istanbul, Turkey) 1–2 μg/kg, propofol (Propofol 2% Fresenius®; FreseniusKabi, Bad Homburg, Germany) 2–4 mg/kg, and rocuronium (Curon®; Mustafa Nevzat, Istanbul, Turkey) 0.6–0.9 mg/kg. For the maintenance anesthesia, a minimum alveolar concentration of 1% sevoflurane (Sevorane® Likit 100%; AbbVie, Queenborough Kent, England) in a 50% air +50% O2 mixture was administered at 1 L/min flow rate.
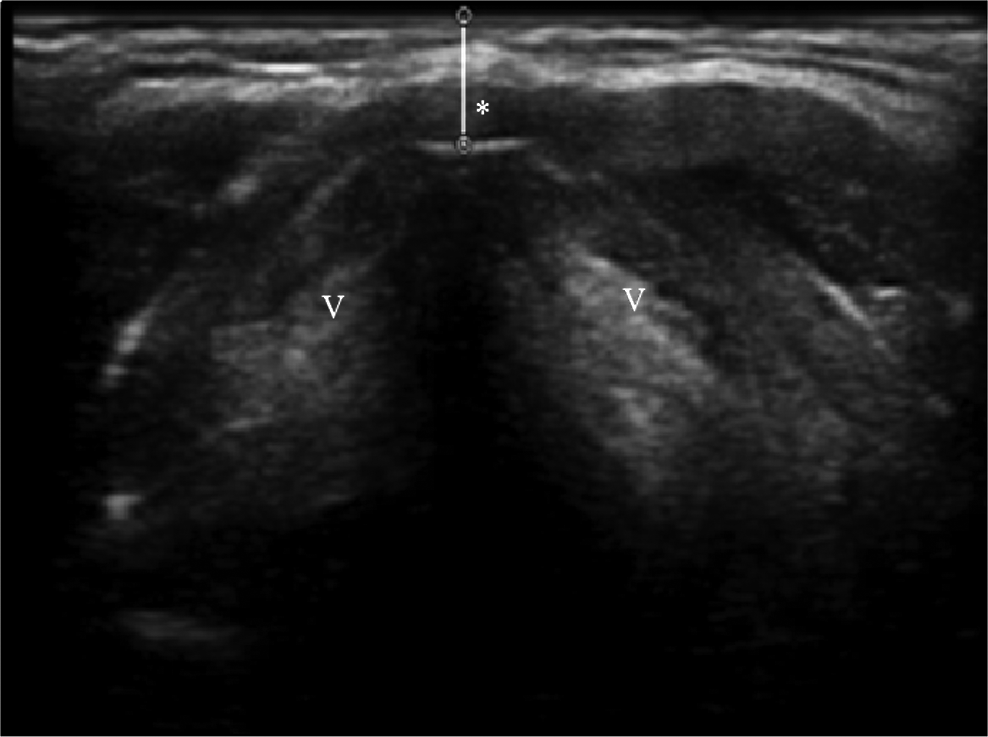
Vocal cords (zone 1). *The distance from the skin to the anterior commissure of vocal cords; V, vocal cord.
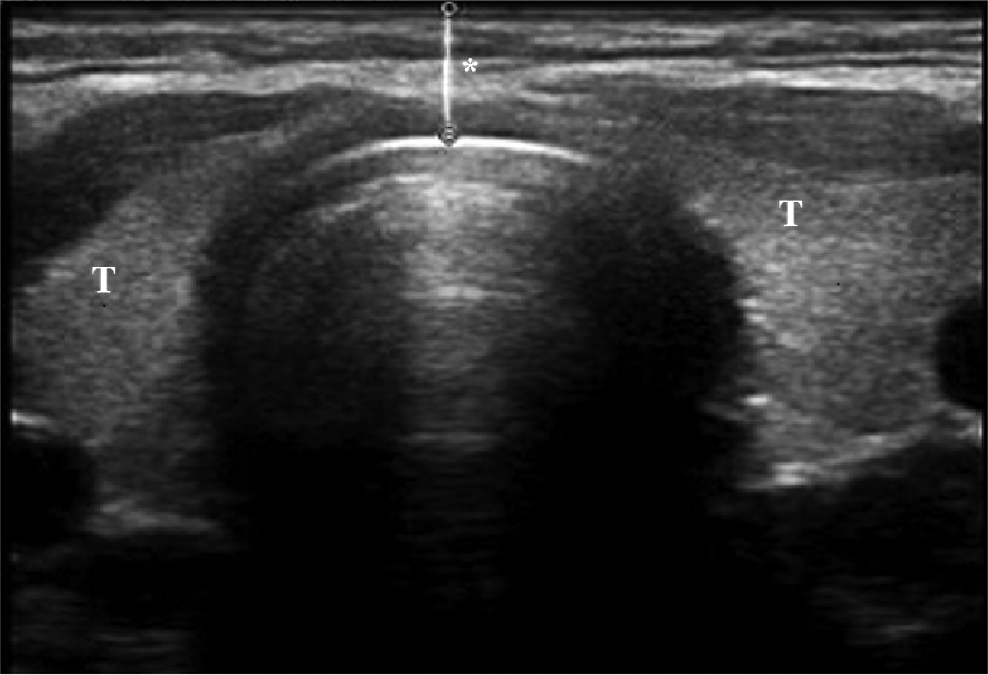
Thyroid isthmus (zone 2). *The distance from the skin to the anterior aspect of the trachea; T, Thyroid.

Suprasternal notch (zone 3). *The distance from the skin to the anterior aspect of the trachea.
Laryngoscopy was performed after full muscle relaxation. An anesthesiologist who was unaware of the clinical screening variables and USG results performed the laryngoscopy with a Macintosh No:3 blade, and the trachea was intubated without a stylet. If necessary, external laryngeal pressure-BURP (back, up, and rightward pressure) was applied, and a styleted endotracheal tube was used. Use of the BURP maneuver and the need for the stylet were recorded. The intubation difficulty scale (IDS) 12 had seven parameters as follows: N1 (number of additional intubation attempts), N2 (number of additional operators), N3 (number of intubation techniques used), N4 (laryngoscopy view as defined by Cormack and Lehane), N5 (lifting force applied during laryngoscopy), N6 (need to apply external laryngeal pressure to improve glottic pressure), and N7 (position of the vocal cord at intubation). The laryngoscopic view was graded according to the Cormack and Lehane classification without any external laryngeal pressure as follows: grade I (full view of glottis), grade II (glottis partly exposed, anterior commissure not seen), grade III (only epiglottis seen), and grade IV (epiglottis not seen). The patients were separated into two groups according to the Cormack and Lehane grading: a grade 1 or 2 was accepted as an easy laryngoscopy, whereas a grade 3 or 4 was considered a difficult laryngoscopy. If difficult laryngoscopy was encountered and the first attempt failed to supply an adequate laryngoscopic view, BURP was applied with adjustment of the head and neck position and a styleted endotracheal tube was used.
Statistical analysis
SPSS 21 Windows program (Statistical Package for Social Sciences, Armonk, NY) was used for the statistical evaluation. In the descriptive statistics of the data, qualitative data were stated as mean and standard deviation values and quantitative data as frequency and percentage values. The distribution of the variables was measured by the Kolmogorov–Smirnov test. The Mann–Whitney U test and independent samples t test were used in the analysis of quantitative data. The Chi-square test was used to analyze qualitative data, and if the conditions for that were not met, the Fisher exact test was used. The level of impact was measured using univariate logistic regression. A value of p < 0.05 was considered statistically significant. Significant potential explanatory variables from univariable logistic regression models were included in multivariable logistic regression models built using stepwise forward selection. The models were compared using Wald test p values.
Results
A total of 130 morbidly obese patients scheduled for laparoscopic weight reduction surgery under general anesthesia with endotracheal intubation were initially enrolled in the study. Of these, 42 were excluded from the study; 3 patients did not meet the inclusion criteria, 34 declined to participate, and 5 for other reasons. A further 14 were excluded due to missing USG records. Thus a final total of 74 patients (64 female, 10 male) were included in the analyses, of which 7 were classified as having difficult laryngoscopy (9.5%) (Fig. 4).
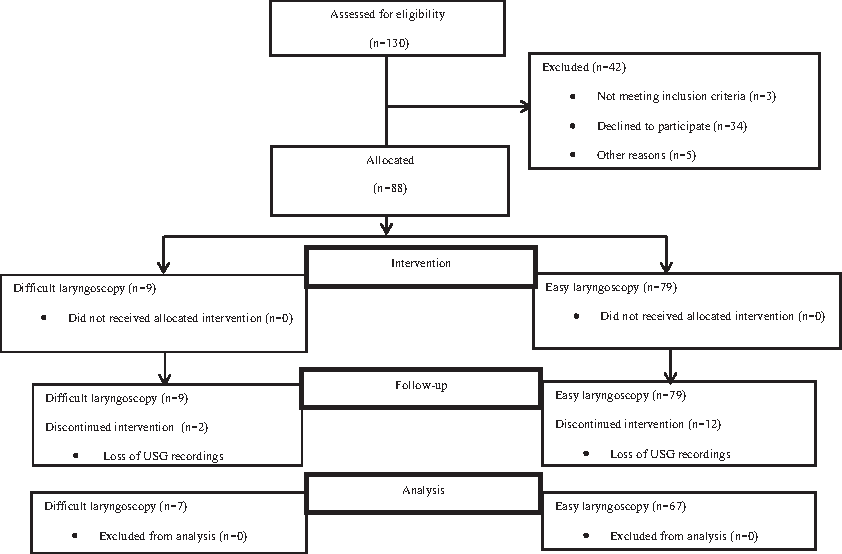
Trial flow diagram.
Patient demographics and preoperative variables according to difficult and easy laryngoscopy are summarized in Tables 1 and 2, respectively.All the patients were intubated successfully within three attempts. The risk factors identified for difficult laryngoscopy were increased age, hypertension (HT), OSAS, and high sternomental distance. The usage of a styleted endotracheal tube, IDS >5, and the number of intubation attempts were found to be statistically significant in the difficult laryngoscopy group (p < 0.05; Table 3). Patients with difficult laryngoscopy were significantly older than the patients with easy laryngoscopy (p = 0.029). The incidence of difficult laryngoscopy rather than easy laryngoscopy was significantly higher in patients with HT (p = 0.016). Patients with OSAS had significantly higher incidence of difficult laryngoscopy than easy laryngoscopy (p = 0.008). Measurements of sternomental distance for difficult laryngoscopy and easy laryngoscopy were 11.5 ± 3.75 and 14.18 ± 2.63 cm, respectively (p = 0.016). A statistically significant difference was determined between the difficult and easy laryngoscopy groups in respect of the incidence of IDS >5 (p < 0.001). The requirement for styleted endotracheal tube usage in the difficult laryngoscopy group was more frequent than in the easy laryngoscopy group (57.1% vs. 10.4%, p = 0.008). There was a significant difference between the two groups according to the number of intubation attempts (p = 0.032).
Values are n (%) unless otherwise indicated.
Fisher's exact test unless otherwise indicated.
Mean ± SD.
Kruskal–Wallis test.
Chi-square test.
ASA, American Society of Anesthesiologist; BMI, body mass index; OSAS, obstructive sleep apnea syndrome.
Values are n (%) unless otherwise indicated.
Fisher's exact test unless otherwise indicated.
Mean ± SD.
Kruskal–Wallis test.
Chi-square test.
USG, ultrasonography.
Values are n (%) unless otherwise indicated.
Fisher's exact test unless otherwise indicated.
Mean ± SD.
Kruskal–Wallis test.
Chi-square test.
BURP, back, up, and rightward pressure; IDS, intubation difficulty scale.
The multivariable logistic regression model identified IDS >5 and OSAS as two risk factors that were independently associated with an increased risk of difficult laryngoscopy. The model identified the IDS variable as the first step, and IDS and OSAS significantly contributed to the model as the second step. OSAS and IDS >5 together created a onefold increase in IDS variable of approximately about 1.96 times the difficulty risk, and OSAS increased the risk by ∼9.12-fold (Table 4).
Stepwise logistics regression (Forward: Wald).
Discussion
In this prospective study, a comparison was made of the role of USG measurements and traditional predictive screening tests of difficult laryngoscopy in morbidly obese patients. The incidence of difficult laryngoscopy was found to be 9.5%. In the preintubation clinical screening tests, increased age, HT, OSAS, and high sternomental distance were determined as risk factors for difficult laryngoscopy. The usage of a styleted endotracheal tube, the number of intubation attempts, and IDS >5 were determined to be statistically significantly high in the difficult laryngoscopy group. However, there was no statistically significant difference between difficult and easy laryngoscopy groups in respect of the USG measurements of anterior neck tissue in morbidly obese patients.
Many studies in literature have investigated the incidence of difficult laryngoscopy. The incidence of difficult laryngoscopy reported in literature has ranged from 3.5% to 31%.8–10,13,14 However, the incidence of difficult laryngoscopy in obese patients is 12–31%. In the current study, the incidence of difficult laryngoscopy was 9.5% in morbidly obese patients. In the current study, a laryngoscopic view as graded according to the Cormack and Lehane scale was used to decide difficult laryngoscopy. The different results between studies could be explained by the different criteria used to define difficult laryngoscopy or could be partially attributed to the demographic characteristics of the groups. In literature, the incidence of difficult laryngoscopy in male populations is higher than in female.9,10,14,15 It is known that fat distribution is different among various ethnic groups.10,16,17 Fulkerson et al. 18 reported that the difference in the incidence of difficult laryngoscopy may be due to the experience of the anesthesiologist, the application of external laryngeal compression, the monitoring of adequate muscle relaxation, the difference in the patient's head position, and the use of different laryngoscope blades.
In the adult population with OSAS, it has been reported that airway management, including endotracheal intubation, may be problematic. Moreover, in obese patients, the diagnosis of OSAS has shown a strong correlation with difficult laryngoscopy. In a previous study, HT and diabetes mellitus were more prevalent in obese patients. 19 Neligan et al. 20 found no relationship between the presence of OSAS, high BMI, or neck circumference and difficulty of intubation in morbidly obese patients undergoing bariatric surgery. In the current study, the incidence of HT and OSAS was significantly higher in the difficult laryngoscopy group than in the easy laryngoscopy group.
In many studies, the relationship between age and difficult laryngoscopy has been investigated, but nonstatistically significant differences have been reported.21,22 However, there are also articles in literature which indicate that the incidence of difficult laryngoscopy increases with age.10,23–25 Although the mean age in the difficult laryngoscopy group was significantly higher in the current study, this difference was not considered to be clinically relevant to the study outcome.
Sternomental distance can be an indicator of a short neck. The cutoff point of sternomental distance has been reported to be 12.5–13.5 cm. 26 Patel et al. 21 proposed that the combination of modified Mallampati test, sternomental distance, and thyromental distance measurements increased the validity of the prediction of difficult intubation in adult patients. In the current study, a statistically significant difference was determined between the difficult and easy laryngoscopy groups in the measurements of sternomental distance, whereas there was no statistically significant difference in the modified Mallampati test and thyromental distance measurements. IDS, first described by Adnet et al., 12 helps to assess the factors associated with difficult intubation and can provide a standardized approach to the determination of difficult intubation. Juvin et al. 3 determined that IDS >5 was more frequently seen in obese patients. The current study showed a significant increase in IDS in the group of difficult laryngoscopy, which was in accordance with the literature. It should be considered useful to determine difficult laryngoscopy in morbidly obese patients.
However, the use of high BMI only for the prediction of difficult laryngoscopy remains debatable. In many studies, BMI has not been found to be a predictive factor for difficult intubation or laryngoscopy.3,27,28 In another study, morbid obesity was found to be a predictor of difficult laryngoscopy, but it was not the increased BMI per se that was a good predictive factor for difficult laryngoscopy. 4 Obese patients have a greater tendency to have difficulties in face mask ventilation or laryngoscopy. 1 In the current study, the incidence of difficult laryngoscopy in morbidly obese patients was investigated and found to be 9.5%.
It has been noticed that a large neck circumference, which is among the recommended predictive factors of difficult intubation, predicts difficult laryngoscopy better than BMI. 1 Distribution of fat in the anterior neck soft tissue may provide a better indication of difficult intubation than neck circumference. 9 In the current study, no difference in neck circumference was determined between the easy and difficult laryngoscopy groups.
Ezri et al. 9 measured the thickness of anterior soft tissue with USG at three levels of the neck (vocal cords, thyroid isthmus, and suprasternal notch) in the same way as in the current study. No difference was determined at the thyroid isthmus level between difficult and easy laryngoscopy. They recommended that the distance from the skin to the anterior aspect of the trachea at the vocal cord level is a good predictor of difficult laryngoscopy. In contrast to that study, in the current study, no statistically significant difference was determined between the difficult and easy laryngoscopy groups at the level of the vocal cords, thyroid isthmus, and the suprasternal notch. Komatsu et al. 10 measured the anterior thickness of the neck only at the level of the vocal cords and no statistically significant difference was found between the easy and difficult laryngoscopy groups as in the current study. It was implied that measurement of the thickness of the pretracheal soft tissue at the vocal cord level was not the best predictor of difficult laryngoscopy in obese patients in the United States. In another study, the thickness of the tongue and anterior neck soft tissue was measured at five levels with USG, and the measurements of the anterior neck soft tissue at the hyoid bone and thyrohyoid membrane levels were found to be greater in the difficult laryngoscopy group. It was suggested that these two sonographic levels could be used to distinguish difficult intubation and it was specified that there was no significant correlation between clinically difficult laryngoscopy tests and sonographic measurements.However, Adhikari et al. found a significant correlation between sonographic measurements of anterior neck soft tissue and BMI. 14 In the current study, no statistically significant difference was determined between the easy and difficult laryngoscopy groups of morbidly obese patients in respect of sonographic variables.
Limitations of this study could be that the conclusions may have been limited by the small sample size of the difficult laryngoscopy group. In addition the anesthesiologists who performed the clinical screening variables and all USG measurements to obtain the soft tissue thickness 1 day before surgery were not blinded to the study hypothesis. Therefore, there may have been some prejudiced bias about the measurements of difficult laryngoscopy. USG measurements of the anterior neck soft tissue were only taken at three levels. The absence of USG measurement of the hyoid bone and thyrohyoid membrane thickness could also be a limitation of the study.
Conclusion
The results of this study demonstrated that USG measurements of anterior neck soft tissue at the level of vocal cords, thyroid isthmus, and suprasternal notch were not good predictive factors for the determination of difficult laryngoscopy in morbidly obese patients. There is a need for further prospectively designed studies with a greater number of patients to be able to evaluate the possible predictive effects of USG for difficult laryngoscopy in morbidly obese patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.