
Abstract
Background:
Obesity affects every aspect of life in obese patients and, in particular, it affects their quality of life. Increased body weight beyond normal is linked to many diseases such as infertility. Polycystic disease of the ovaries is common in childbearing females, with incidence of 7% in the population and 2/5 to 4/5 of this group are either overweight or obese. Changes in all aspects of quality of life after bariatric surgeries were studied widely. One aspect that needs more elaboration is the improvement of fertility in obese patients with polycystic ovarian syndrome (PCOS) postbariatric surgery.
Setting:
All operations and follow-ups were carried out at the Hatwan Private Hospital for Laparoscopic and Bariatric Surgery and the Obesity Unit at the Sulaimani Teaching Hospital (Sulaimani Governorate, Kurdistan Region/Iraq).
Methodology:
The prospective observational study was from a total 167 patients who underwent sleeve gastrectomy for a period of 4 years (from July 4, 2012, to July 5, 2016). Of all the patients, 123 were female with a male to female ratio of 4.3 to 1.23. Forty-two of the female patients had primary goal of improvement in their fertility. Of these 42 obese patients, 8 had PCOS, they were evaluated, and included in this study. These patients were compared in the conception of case matching to eight other patients who were obese and infertile, but otherwise healthy. All study participants were interviewed by the same team, and a questionnaire was administered relating to information on the patient's gynecological and obstetric aspects of life, before and after operation.
Results:
Of the 123 female patients who underwent bariatric surgery, 8 of them were obese and married with PCOS, with a body mass index of 40–60 kg/m2, and a primary aim of becoming fertile. Patients with primary and secondary infertility were included.
Conclusion:
Significant changes in fertility were recorded in obese females with PCOS postbariatric surgery as early as 3 months after the operation. This was particularly true in patients with a shorter duration and onset of obesity after the age of 18 years.
Introduction
O
Body fat is essential for prodigality, while the extra fat lead to certain reproductive dysfunctions. 6 The grade of extra body fat and its location issue are significant factors that affect the childbearing capacity. 1 Sex hormones are primarily condensed in the fat more than the blood. 7
Polycystic disease of the ovaries is common in childbearing females, with incidence of 7% in the population and 2/5 to 4/5 of this group being either overweight or obese.4,8,9
The clinical manifestations of polycystic ovarian syndrome (PCOS) may include aberrations in menses, features of male sex hormone overactivity, and obesity, as well as insulin resistance. 10 In addition, body mass index (BMI) in excess of 30 kg/m2, when leptin and ghrelin hormones are disturbed, may exaggerate these effects. In addition, it is known that leptin is a possible factor that results in overactivity of androgens and infertility in females with PCOS.1,11 The inconsistency between high leptin blood levels and its core influence exemplifies the basis for the connotation that morbid weight gain may reflect a state of body that is unresponsive to the leptin.11,12
The main factors entangled in the link may be insulin excess and insulin resistance. These aspects of high body weight are clearer in cases of polycystic ovarian syndrome.13,14 Similarly, it also increments the hazard of ovarian achievement and insulin resistance and can also decrease the chance of conception in females with normal menstruations.14,15
Finally, high body weight in early life increments abnormal cycles, chronic oligo/anovulation, and failure of conception, as well as excess hair growth and hormonal abnormalities during adulthood.13,16 In addition, obese females with PCOS have utmost frequency of abnormal menses 14 and higher rates of amenorrhea, infertility, 5 and hirsutism, compared with females of normal BMI with the same syndrome. 14
Most of these studies in the literature are not from this region, and there may be differences in statistics and different ethnic backgrounds of European/American women to women from Middle Eastern background. This article aims to find the effect of weight-loss surgery on infertility in obese females with ovarian cystic disorders.
Patents, Materials, and Methods
From the total 167 patients, who underwent sleeve gastrectomy within a 4-year period, from July 4, 2012 to July 5, 2016, sixteen infertile obese female patients were included in this work. The study was conducted at the Hatwan Private Hospital for Laparoscopic and Bariatric Surgery and the Obesity Unit at the Sulaimani Teaching Hospital. One hundred twenty-three were female with a male to female ratio of 4.3:1.23. Forty-two of the female patients who had a primary goal of improvement in their fertility, only eight obese females with PCOS, were evaluated and included in this study. A comparison was made between them in the conception of case matching to eight patients who were obese and infertile, but were otherwise healthy.
The age of patients in this work spreads from 20 to 35 years, with a mean BMI of 48 (35–60) kg/m2.
Participating patients were divided into the following:
(1) Study Group A consisted of eight obese patients with PCOS. (2) Control Group B consisted of eight obese patients without PCOS, this group matched Group A in age, body weight, and BMI, for the purpose of comparison.
Informed consent was obtained and a consent form was signed by each patient. The research was confirmed by the Ethics Committee of University of Sulaimani, College of Medicine.
All the operations were done by the same bariatric surgical team. All participants were interviewed by the same team, where a questionnaire was administered regarding data on their gynecological and obstetric aspects of life before and after weight-loss operation. Three persons were conducting the interview; one of them was a female senior nurse, to ensure patients felt comfortable in answering the questions, providing explanation to the patients on the reason behind the interview to obtain informed consent.
Each patient was evaluated clinically, with BMI, extra body weight (EBW), and body fat content (BFC) being measured before and on each visit after operation with a digital skin fold caliper. All patients underwent complete evaluation before the operation (including endoscopy and abdominal ultrasonography). Additional investigations were performed according to the risk profile of each individual patient. Patients were followed up 1 week postoperation, 4 weeks postoperation, monthly for 3 months, and then bimonthly for 1 year for each patient after the operation.
Each patient infertility status was evaluated by a gynecological ultrasound, thyroid function tests (T3, T4, thyroid stimulating hormone [TSH]), hormonal assays (serum prolactin, estradiol, testosterone, progesterone, luteinizing hormone (LH), and follicular stimulating hormone, hereon referred to as “FSH”), fasting blood sugar, and serum lipids. Unfortunately, sex hormone binding globulin (hereon referred to as “SHBG”) was not available during the period of this study. Blood works were continued for those who did not become pregnant in the 1-year period of follow-up since operation or had a non-ovulatry menstrual cycle in the 1-year period of follow-up since operation.
At each visit, BMI and EBW loss were recorded in kilograms, besides the time of suspecting of pregnancy, which was confirmed by the human chorionic gonadotropin test (pregnancy test).
Results
A total of eight married females who had PCOS and were infertile with a BMI of 40–60 kg/m2 were included, with an age of 25–35 years. Patients with primary and secondary infertility underwent bariatric surgery.
All clinical (Table 1), blood work (Tables 2 and 3), and imaging (Table 4) results and case-matched comparison expressed (Table 5) were recorded and analyzed.
BMI, body mass index; BFC, body fat content; EBW, extra body weight.
TSH, thyroid stimulating hormone.
Samples for hormonal assay taken fifth or sixth day of menses.
FSH, follicular stimulating hormone; LH, luteinizing hormone; OP, operation.
EWL, extra weight loss.
BMI was in relation to BFC in our patients, as all were females and nonathletes, with extra muscle mass.
The range of EBW was between 44.2 and 70.3 kg, with a mean EBW of 55 kg.
The amount of body weight loss at the time of pregnancy was 18.5–35 kg and mean weight loss was 25.5 kg.
The time needed for pregnancy was 99 to 115 days, with a mean of 99 days after the operations.
All patients had normal thyroid function tests and clinically considered euthyroid.
All patients showed improvement of hormonal status, androgen and FSH declined as early as the third month postsurgery.
In the following 3 months postoperations, all the patients had average menstruation and 75% became pregnant.
Of 42 patients who had a primary goal of improving their fertility, eight patients with PCOS in Group A, and Group B chosen from the remaining 34 patients, were case match in age and BMI. All patients in Group B who did not have PCOS became pregnant during the period of 89 to 118 days, after losing 14.7 to 36.9 kg of their extra weight loss (EWL).
Age of start of obesity in most patients in this group was over 23 years of age, apart from patient number 1 and 3 who were obese from age of 17 years. Both had excess facial hair and improved from the gynecological point of view, but did not become pregnant (Table 6).
All the infertile obese patients in Group B had no facial hair, they became obese after the age of 18 years, and all of them became pregnant during the period of 89 to 118 days after the operation (Table 7).
When the patients became pregnant, EWL was widely different in Group B (SD 7.11), while patients in Group A lost approximately the same amount of EBW (SD 4.27).
It is also noted that the time needed to become pregnant in Group B was longer and widely different compared with Group A (SD 9.84 and 6.12 correspondingly), as shown in Table 8 and Fig. 1).
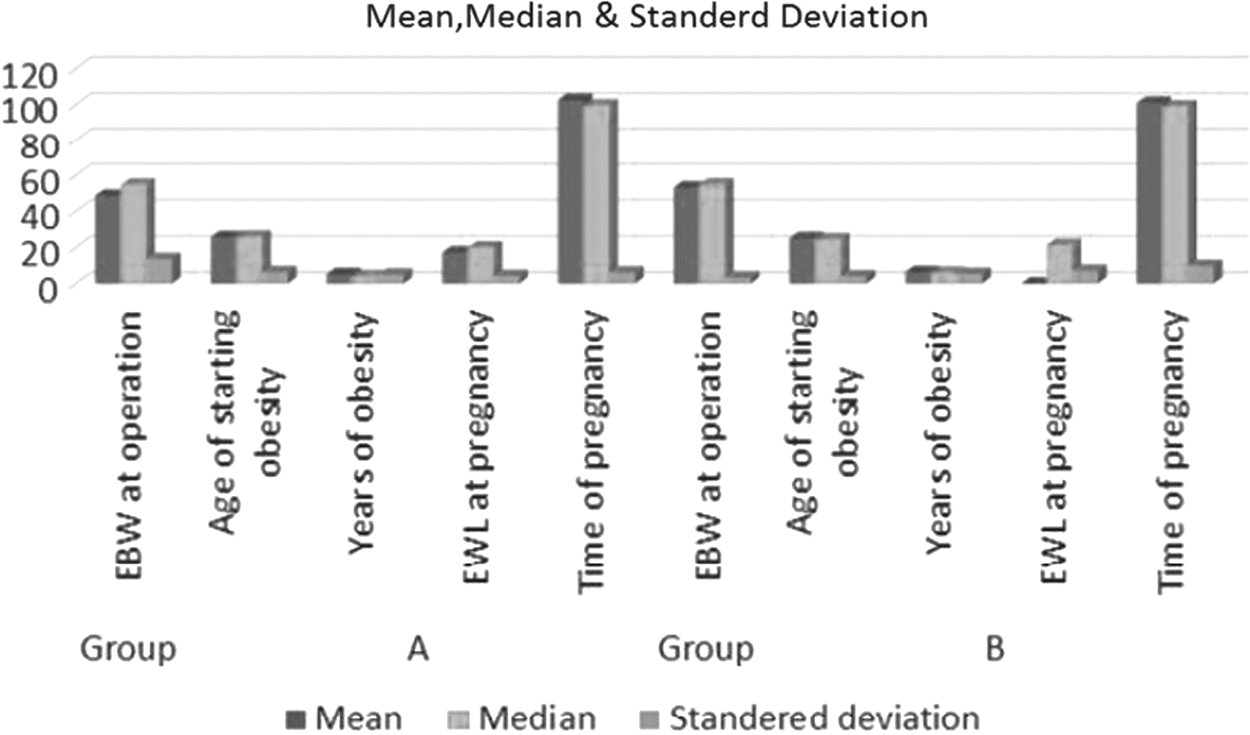
Figure showing the mean, median, and standard deviation of the EBW at operation, age onset, duration of obesity, EWL at pregnancy, and the time needed to become pregnant in patients in both Group A and Group B. EBW, extra body weight; EWL, extra weight loss.
EWL, extra weight loss.
Discussion
Obesity is considered one of the most common causes preventing fertility. An increasing number of females in childbearing age gain high levels of extra weight, 17 which affects menses by disturbing the estrogen metabolism with alterations in the intensity of SHBG and rising of blood insulin.1,16,18
It is affirmed that excrescent insulin is susceptive to rousing formation of steroids and androgen by the ovarian theca cell system, 19 and shares in increased formation of androgens by ovaries.15,19
Obesity has been known as a prevalent feature of the cystic disorders of ovaries, as well as outraging many of the hazards connected with PCOS. 20 In this group, it is probably more important to induce weight loss than in the general population and to prove that it is possible to induce weight loss and maintain this weight loss long term. 21 It is mentioned that towering BMI at the age of 18 years, even at levels lower than those count to be obese, is a risk factor for ulterior failure of conception. 19
Two of the patients in this study have a history of obesity before the age of 18 years. As prolonged obesity (with an early onset) is associated with excessive facial hair, both of these two patients presented facial hirsutism. This may explain why the remaining patients with shorter duration of obesity and with no facial hair respond to early body weight loss, and their gynecological status improved promptly. Unfortunately, neither of the two patients with primary infertility responded clinically, and although there were significant laboratory and imaging differences after the surgery, they still did not become pregnant. Thus, primary infertility in these two females may be another factor in the problem as Linnè found that teenage obese females are at greater risk of not becoming pregnant compared with female teenagers with normal weight. 16 Planning for weight loss must focus on caloric limitation and encouraging physical activity, but benefit can be had from drugs and surgery as add-ons. 15
In this study, those who were selected for surgery were identified on the basis of their failure to lose weight through dieting, physical exercises, and/or drugs. Most of them demonstrated early significant clinical amendment, which reverberates the decline in insulin levels with amelioration in menses. Conception may be consequential on a burst in insulin sensitivity, which affects ovarian function, as significant positive connection to ovulatory leverage is linked to the level of weight loss.14,22
There are scarce reports on the influence of losing weight with respect to ovarian dysfunction; an occasional article clearly demonstrates that losing weight ameliorates both endocrine and metabolic defects and that ovarian function could be eloquently restored. 23
Polycystic disease of the ovaries is common in childbearing females who are overweight or obese.7,13,20,23 Restoration of average menses and amendment of function of ovaries symbolize the primary goal to be carried out in many women with PCOS.24,25
Three-quarters (75%) of participating patients became pregnant as early as 4 months postsurgery or at mean EBW loss of 21.5 kg, demonstrating reversal of their gynecological abnormalities. This does not correlate with literature that claims conception of 29% of participants in a group, of which 80% manifest betterment of menses. Hoeger et al. states that weight loss is the convenient remedy for obese females who have endocrine derangement and defects in ovarian function and failure in conception. 22 In another study by Pasquali et al., ∼80% of patients achieved regular menses, while 60% had ovulations and only 40% of the patients had conception, as shown in Table 9.26,27
In this study, all of the patients showed improvement from a gynecological point of view, all had normal ovulation, and 75% became pregnant. These results do not correlate with the studies of Calhoun and Parquet et al., as the level of pregnancy is higher in this study.
This ambivalence may be untangled in this study, where all patients had POCS, three-quarters of whom had a short history of obesity and obesity started after the age of 18 years. Improvement and cure of their PCOS were noticed as confirmed by imaging shown in Table 4.
In a case-matched comparison between Group A (all patients obese with PCOS) and Group B (all patients were obese and infertile but otherwise healthy), it is noticeable that all patients in Group B became pregnant as early as 3 months postsurgery when they lost the extra weight, as seen in Tables 5 and 8. This can be explained by the fact that considerable loss of extra weight may be a sole factor in remedy of menstrual dysfunction and conception rates in affected females. 7 It is worth mentioning that the patients in Group B had no facial hair, and their obesity started after the age of 18 (as shown in Table 7), although they needed a longer period to become pregnant (Fig. 1). This may clarify the importance of the age of obesity onset and presence of facial hair as obstacles in getting pregnant after improving the following aspects: clinical, biochemical, and ultrasound results. While the extent of weight loss is in favor of improving fertility, the patients in Group B need a little longer to reach significant EWL and fertility compared with the patients in Group A (as shown in Table 8 and Fig. 1).
Conclusion
Significant changes in fertility were recorded in obese females with PCOS after undergoing bariatric surgery as early as 3 months after the operation. Particularly in those having a shorter duration and onset of obesity had been after the age of 18 years.
Footnotes
Acknowledgments
The author thanks all the patients, who took a part in the work, for their cooperation, and also the colleagues in the metabolic and bBariatric Team in Hatwan and Sulaimani Teaching Hospital for their technical help.
Author Disclosure Statement
No competing financial interests exist.