
Abstract
Background:
Reported outcomes after removal of adjustable gastric band (AGB) are very limited, yet, important to direct patient and surgeon decision-making. The aim of this study was to investigate the medium-term weight changes in patients who underwent AGB removal without an additional bariatric procedure.
Methods:
In this retrospective study, we analyzed data of 25 patients who had undergone AGB removal without an additional bariatric surgery (2009–2016).
Results:
The reasons for the AGB removal included gastroesophageal reflux disease (n = 10, 40%), band slippage (n = 5, 20%), band prolapse (n = 5, 20%), band erosion (n = 4, 16%), and planned incisional hernia requiring mesh implantation (n = 1, 4%). At a median follow-up time of 2 years (interquartile range [IQR] 1–4) after laparoscopic AGB removal, the median weight and body mass index changes were +7.3 kg (IQR, −2 and +18) and +1.9 kg/m2 (IQR, −1 and +6), respectively. Forty-eight percent (n = 12) did not gain more than 3 kg of body weight after removal of their gastric band. All patients experienced resolution of their AGB-related symptoms.
Conclusion:
Recognizing that weight regain is not necessarily inevitable for all patients after gastric band removal may assist in decision-making.
Introduction
The laparoscopic adjustable gastric band (LAGB) was one of the most popular bariatric procedure performed 10 years ago. Currently, gastric banding is less frequently performed worldwide when compared with the gastric bypass or sleeve gastrectomy. 1 The demand for gastric banding has decreased due to increased complication rates and disappointing weight loss. O'Brien et al. 2 showed an excess weight loss (EWL) of 47% after LAGB placement (with 81% follow-up at 15 years); however, his revision rate was 50%. In his systematic review of seven long term studies (>10 years), the LAGB was a safe bariatric procedure with the mean EWL of 54% (range 33–60%) and a median revisional surgery rate of 26%. Tammaro et al. 3 reviewed 794 patients who underwent LAGB (with 90% follow-up at 10 years) showed the overall band removal rate with or without replacement to be 38%. The mean time to removal of the band was 148 months (95% confidence interval: 138–167). Carandina et al. 4 showed that out of 301 patients who underwent LAGB placement, band removal was noted in 104 (35%) patients in 10 years. The main reason for band removal was insufficient weight loss or weight regain. Other reasons included food intolerance (28%), slippage or pouch dilatation (12%), intragastric migration (11%), and device dysfunction (7%). Reported outcomes after band removal are very limited, yet, important to direct patient and surgeon decision-making. Aarts et al. 5 and Rohner et al. 6 showed that there was significant weight regain in patients undergoing LAGB removal without a concomitant revisional procedure. In this study, we present the medium-term outcomes of patients who underwent LAGB removal without an additional revisional bariatric procedure.
Method
In this retrospective study approved by our Institutional Review Board, we looked at all patients who had undergone LAGB removal without an additional bariatric surgery from January 2009 to January 2016. There were no patients who underwent band removal alone due to insufficient weight loss in this cohort. All patients were regularly followed by surgeons, dieticians, and physicians after LAGB removal.
All band removal procedures were done laparoscopically. Adhesions between the stomach and liver were taken down using sharp dissection. Adhesions and plicated fundus around the gastric band were taken down and the gastric band was removed. The adhesive capsule formed on the stomach was partially excised and stomach returned to its normal anatomy. A flexible endoscope was routinely passed down the esophagus and stomach to check for leak, bleeding, or obstruction.
Data collected included baseline demographics, medical comorbidities, preoperative parameters, and the main outcome of weight change after LAGB removal. Weight changes (kg) were calculated as weight at last follow-up − weight preband removal, and body mass index (BMI) changes (kg/m2) were calculated as BMI at last follow-up
Results
Out of 109 patients who underwent band removal during the study period, 84 patients had revisional bariatric surgery. Twenty-five patients underwent LAGB removal only during the study period, who constitute the current study cases. The median age was 54 years (IQR 43–64) and 21 (84%) were female. Comorbidities included hypertension (n = 14, 56%), dyslipidemia (n = 6, 24%), diabetes mellitus (n = 6, 24%), and obstructive sleep apnea (n = 5, 20%). The median duration interval between LAGB placement and removal was 48 months (IQR 24–84).
The reasons for the LAGB removal include gastroesophageal reflux disease (GERD) noted on endoscopy (n = 10, 40%), band slippage (n = 5, 20%), band prolapse (n = 5, 20%), band erosion (n = 4, 16%), and incisional hernia requiring major abdominal wall reconstruction and mesh implantation (n = 1, 4%).
The median operative time and estimated blood loss were 56 min (IQR 42–80) and 10 mL (IQR 5–40), respectively. The median length of hospital stay after LGB removal was 1 day (IQR 1–2). There was no intraoperative complication. Two patients had 30-day complications; one patient had an abdominal fluid collection requiring CT-guided drainage and another had a pulmonary embolism. There were no perioperative mortalities.
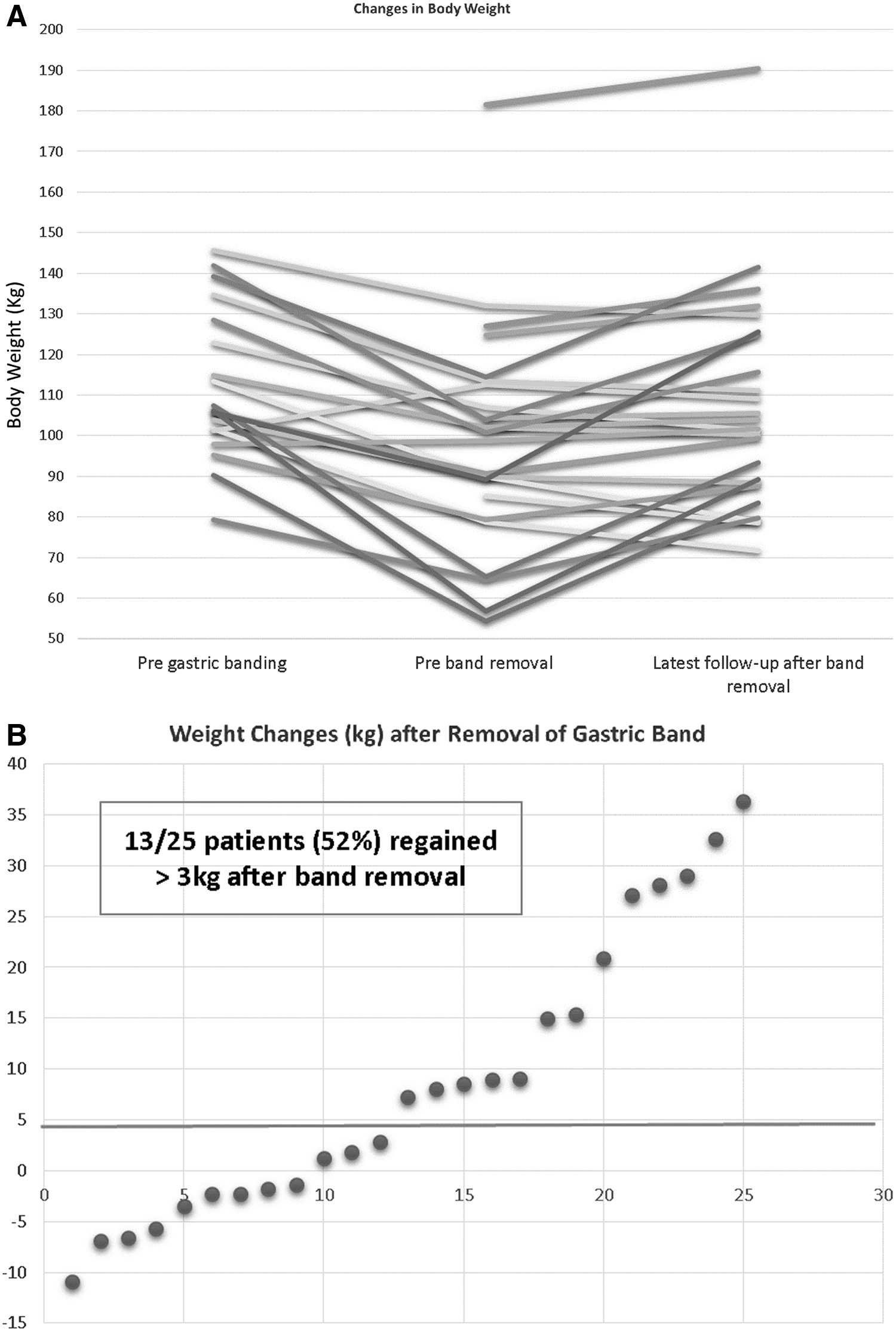
The median follow-up after LAGB removal was 2 years (range 1–6, and IQR 1–4). The median pre-LAGB removal weight and BMI was 100.7 kg (IQR 82.2–113) and 35.4 kg/m2 (IQR 29.2–39.8), respectively. The median increase in weight and BMI at the time of their last follow-up was +7.3 kg and +1.9 kg/m2, respectively (Table 1). Forty-eight percent (n = 12) of these patients did not gain more than 3 kg of body weight after removal of their gastric band (Figure 1). Overall, in five patients, the body weight at the last follow-up point was more than the initial body weights before band placement. All patients experienced resolution of their symptoms during the follow-up period.
Weight and Body Mass Index Changes Following Band Removal
BMI, body mass index; IQR, interquartile range.
Out of 12 patients with minimal weight gain (<3 kg) after gastric band removal, 2 patients had not lost any weight with gastric band. In addition, patients with minimal weight gain (<3 kg) after gastric band removal originally had less weight loss with gastric band compared to patients who significantly gained weight (>3 kg) after band removal (12.4 ± 11.6 kg vs. 28.5 ± 12.7 kg, p = 0.01). However, the mean BMI of two groups was similar at the time of gastric band removal (36.3 ± 4.6 kg/m2 vs. 33.9 ± 10.1 kg/m2, p = 0.4).
Discussion
In our cohort, 56% of the 25 patients had band-related complications and an additional 40% had GERD. At 2 years of follow-up after band removal, the median increase in the body weight and BMI were 7.3 kg and 1.9 kg/m2, respectively. Fifty-two percent of patients gained significant weight after band removal. Specifically, in 20% (n = 5), their weight at the last follow-up exceeded the initial body weight before the band placement. However, 48% of these patients did not gain more than 3 kg of body weight after removal of their gastric band during the median 2-year follow-up period. Not surprisingly, our data indicate that significant weight gain after band removal is more commonly seen in patients who had lost more weight with gastric band.
LAGB placement is still the third most common bariatric procedure in the United States making up 5.7% of all procedures performed in 2015.1,7 The decreasing trend over the past decade has been due to its increased complication long-term rate and poor weight loss profile. Trujillo et al. 8 studied long-term outcome of gastric banding in 73 patients. Only 33 patients had the gastric band in situ at a mean follow-up of 12 years. The reasons for band removal were leakage (n = 16), band slippage (n = 15), and insufficient weight loss (n = 9). The 5- and 10-year rates of patients who still had their gastric band were 82% and 53%, respectively. Himpens et al. 9 and Lanthaler et al. 10 showed the revision rate after LAGB placement to be 60% (with 54% follow-up at 12 years) and 53% (with 80% follow-up at 10 years), respectively. O'Brien et al. 2 showed a similar result with a 50% revision rate at 15 years. However, in his systematic review of the literature on bands in place more than 10 years, the mean EWL after LAGB placement from the pooled data was 54% with only a median revision rate of 26% (range 8–60%).
The bulk of the peer-reviewed literature shows that LAGB has relatively poor weight loss, and that after band removal, an additional bariatric procedure is required to maintain the desired weight loss. Aarts et al. 5 showed that there was significant weight regain after band removal alone (n = 21) compared with patients who had band removal combined with or followed up by a revisional surgery. The median interval between LAGB placement to band removal was 4 years (range 1–12) and the median follow-up after band removal was 3 years (range 1–9). The median percent EWL in patients with band removal, and revisional surgery compared with patients with band removal alone was significantly different (67% vs. −11%, p < 0.001). Similarly, Rohner et al. 6 showed that band removal without additional bariatric surgery resulted in weight regain in 19 out of 21 patients (with a mean follow-up of 63 months). The mean BMI increased to 41 kg/m2 at follow-up compared with 35 kg/m2 at the time of band removal. The average weight regain was 17 kg. In our cohort, however, we find that the changes in body weight between pre- and postgastric band removal were not significant in some patients at least for the first 2 years of follow-up. In fact, 48% of these patients did not regain more than 3 kg from their preband removal weight. Dietary adjustment, behavioral modifications and life style changes in these patients may be sufficient, particularly for those with bands removed due to complications.
This study has limitations especially regarding the small sample size (25 patients) and short duration of follow-up. With longer follow-up, additional weight regain may emerge as shown by others. As a retrospective observational study, the compliance to a dietary regimen and the amount of exercise performed cannot be assessed in our cohort. The body weight and BMI pre-LAGB placement were not available in six patients as their LAGB was not placed at our center. The value of this study, however, lies in its inclusion of only those who underwent band removal without additional revisional bariatric surgery, a cohort not well investigated in the literature.
Conclusion
The findings of this study, which is the largest reported series to date, indicate that almost half of patients did not have significant weight regain after gastric band removal in short- to medium-term follow-up. Recognizing that weight regain is not necessarily inevitable for all patients after gastric band removal may assist in patient and surgeon decision-making regarding band removal and subsequent management. Larger studies with longer follow-up are necessary to better determine weight loss durability after band removal.
Footnotes
Author Disclosure Statement
No competing financial interests exist.