
Abstract
Background:
Laparoscopic Roux-en-Y gastric bypass (LRYGB), a common bariatric surgery, may be associated with different ocular effects. The present study aimed to investigate the effect of bariatric surgery on refractive errors.
Methods:
The clinical study investigated 85 morbidly obese patients, undergoing LRYGB. Ocular examination conducted by one optometrist before and after surgery included measurement of best corrected visual acuity (BCVA) by log minimum angle of resolution (MAR) chart, pupil reactions, slit lamp examination, and visual field determination.
Results:
The mean body mass index of patients significantly reduced from 46.32 ± 6.90 before surgery to 34.20 ± 10.80 after surgery. The optic examination of patients revealed the difference of postoperational mean BCVA OU log MAR with their previous glasses at 0.063. The changes in the refractive error of patients were as follows: 3 patients (3.5%) had −0.25, 1 patient (1.1%) had −0.5, 1 patient (1.1%) had −0.75 myopic shift, and 75 patients had hyperopic shift. Six patients had no change in their refraction status.
Conclusions:
The significant refractive changes, especially hyperopic shift after bariatric surgery, are an important issue and further studies on the underlying mechanisms, especially those that may be related to blood pressure changes, can help physicians and optometrists, on appropriate management.
Introduction
Obesity is a critical health issue with a global annual increase in its prevalence 1 and is associated with major comorbidities, including the metabolic effects of excess adipose tissue, mechanical consequences of excess weight, and psychosocial consequences, which reduces the quality of life and life expectancy of patients. 2 High body mass index (BMI) is also associated with ocular problems, such as age-related maculopathy and cataract at the younger ages,3–5 and morbid obesity (BMI >35 kg/m2) may change the ocular parameters, including retinal nerve fiber layer thickness, retinal ganglion cell, choroidal thickness, and increased intraocular pressure (IOP). 6 Also, hyperglycemic state of the patients is associated with transient refractive errors and tendency toward greater hyperopic changes. 7
After the introduction of bariatric surgery as one of the most effective therapies for morbidly obese patients, 8 several modalities of bariatric surgery have been used to treat these patients, including laparoscopic Roux-en-Y gastric bypass (LRYGB), which significantly decreases excess weight along with resolution of hypertension, dyslipidemia, gastroesophageal reflux, and arthritis. 9 Along with all the advantages of bariatric surgery, it is also associated with several complications. 10 One of the important complications after malabsorptive procedures is nutritional deficiencies, including protein, iron, fat soluble vitamins, vitamin D, B12, iron, folate, and calcium.11,12 On the contrary, nutritional deficiencies are associated with different ocular problems. 13 Therefore, investigating the ocular status of patients after bariatric surgery is of great importance.
Few case reports have established vitamin A deficiency after bariatric surgery with ophthalmic complications.14,15 Optic neuropathy has also been reported due to zinc, copper, and vitamin B12 deficiencies after bariatric surgery.16–18 Also, ocular xerosis and night vision changes are reported as frequent ocular complications following RYBG. 19 The ophthalmic complications related to nutritional deficiencies are preventable by using supplements, but as far as the authors are concerned, no study has investigated the refractory changes after bariatric changes without nutritional deficiencies.
As suggested, hormonal changes of overweight can cause myopic shift, 20 and thus, we hypothesized that the correction of excess weight, hyperglycemia, and hyperlipidemia of morbidly obese patients after bariatric surgery may reduce the obesity-induced myopic changes; the present study aimed to investigate the effect of bariatric surgery on refractive status of patients' eyes.
Materials and Methods
Study design and intervention
In this clinical trial study, obese patients who referred to the Obesity Clinic of Rasoul-e-Akram Medical Center from December 2013 to December 2016 were recruited. This center is a multidisciplinary center, an endorsed member of the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) organization, which manages a great number of obese patients each year since 2008 and registers their pre- and postoperational data in a database.
The study protocol was approved by the Ethics Committee of Iran University of Medical Sciences (code: IRCT201202168588N2). The design and objectives of the study were explained to all participants, and patients signed a written informed consent for participation in the study. All ethical considerations of the Declaration of Helsinki were met during the study.
In this center, morbidly obese patients with BMI ≥35 kg/m2 were candidates of LRYGB, which is performed by one surgical team by a five-port technique for all patients. Liver retraction was conducted by the fifth trocar. The pouch size was considered at 25–35 cm3 by devising retrogastric tunnel at the minor curve, biliopancreatic limb 40 cm, and Roux limb was 100 and 150 cm regarding BMI less or more than 50, respectively. The surgical procedure has been previously published. 21 Distal ileojejunal anastomosis was performed at 50 cm to leave a comfortable length of mesenterium, and gastrojejunostomy was performed using circular end-to-side anastomosis endoluminal staples and hand sewn technique to close the staple insertion site.
All patients were visited by a single optometrist one day before and 6 months after surgery at the Optometry Clinic at Rasoul-e-Akram Medical Center and received ocular examination, which included measurement of best corrected visual acuity (BCVA). For this purpose, the optometrist used refractometer RM 8800 to detect the refractive errors in patients and then measured visual acuity with a standard 6 m Snellen chart. The visual acuity fractions were then changed into logarithm of minimum angle of resolution (log MAR); refraction was measured by ±0.25 steps and varied from 0 to ±7.00. We thus calculated the mean without any round up or down. For example, mo5/10 for visual acuity is equal to MAR = 10/5 = 2 and (log 2 = 0.3), so 0.3 is log MAR of a patient with 5/10 visual acuity using a Snellen chart. If there were any spectacles, the number of lenses was measured by a CL200 lensmeter. Patients with high refractive errors (e.g., caused by keratoconus), diseases of the anterior and posterior chambers, and medical conditions that affect ophthalmic function were excluded from the study. Any condition that could negatively affect the visual acuity measurement and make the person respond incorrectly to the optotype, including patients with motor inability or who required cycloplegic agents, was excluded. Then, other patients were asked to come back 180 days after surgery to be visited based on the abovementioned protocol. Any changes in visual acuity (log MAR) would lead to changes in spectacle mark and refractive changes. A refractive change of >+0.25 D was considered hyperopic shift and >−0.25 D as myopic shift.
Demographic and anthropometric characteristics, medical history, as well as complete blood cell counts, alkaline phosphatase level test (ALK.PH), direct bilirubin (DBIL), thyroid function test (T3RU), renal and liver function tests, blood sugar, lipid profile, and other serum parameters were measured. As routine care, patients receive supplements rich in B vitamins, zinc, vitamins A, D, E, C, K, magnesium, selenium, and other minerals after surgery.
Statistical analysis
Results are presented as mean ± standard deviation for quantitative variables and summarized by frequency (percentage) for categorical variables. Continuous variables were compared using T test or Mann–Whitney U test, whenever the data did not appear to have normal distribution or when the assumption of equal variances was violated across the study groups. For comparing continuous variables in before–after intervention, paired sample T test and Wilcoxon test were used. For statistical analysis, the statistical software SPSS version 21.0 for windows (SPSS, Inc., Chicago, IL) was used. α = 0.05 or less was considered statistically significant.
Results
A total of 85 obese patients completed the protocol of the study with mean age of 38.2 ± 9.25 (range: 17–61) years. Most patients (N = 76, 89.4%) were female, and nine patients (10.6%) were male. As Table 1 shows, mean BMI of patients significantly reduced from 46.32 ± 6.90 before surgery to 34.20 ± 10.80 after surgery (p < 0.001).
Comparison of Serum Parameters of the Studied Patients Before and After Roux-en-Y Gastric Bypass Surgery
BCVA OU, best corrected visual acuity (results of both eyes' refractive examinations); BMI, body mass index; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; SD, standard deviation; SGOT, serum glutamic oxaloacetic transaminase; SGPT, serum glutamic pyruvic transaminase.
The optic examination of patients revealed the difference of postoperational mean BCVA OU Log MAR with their previous glasses at 0.063. The changes in the refractive error of patients were as follows: 3 patients (3.5%) had −0.25, 1 patient (1.1%) had −0.5, and 1 patient (1.1%) had −0.75 myopic shift. Six patients had no change in their refraction status. The rest (N = 74, 87.1%) had hyperopic shift, as follows: 62 patients had +0.25, 10 patients had +0.5, 1 patient +0.75, and 1 had +1.00 hyperopic shift postsurgical, compared with the presurgical state (Fig. 1).
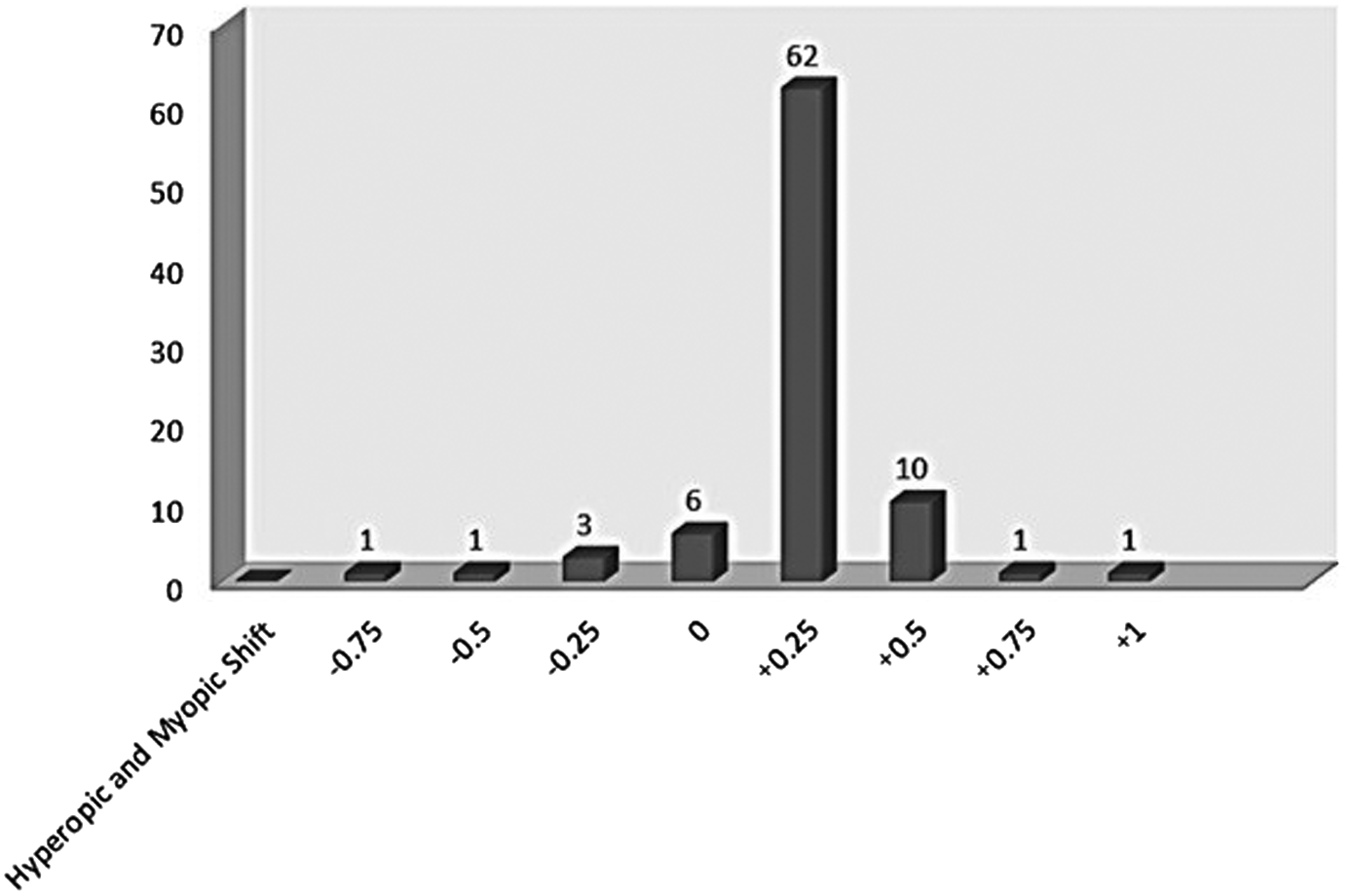
Diagram of hyperopic and myopic shift postsurgical compared with presurgical state.
Serum parameters in two groups of studied patients with hyperopic shift are compared in Table 2. Results showed a significant difference in BMI, ALK.PH, DBIL, total PR, and T3RU between the two hyperopic groups (Hyperopic ≤+0.25 and Hyperopic >+0.25).
Comparison of Serum Parameters in Two Groups of Studied Patients with Hyperopic Shift
BMI, body mass index; BUN, blood urea nitrogen; CR, creatinine; ESR, erythrocyte sedimentation rate; FBS, fast blood sugar; PT, prothrombin time; PTH, parathyroid; PTT, partial thromboplastin; TG, triglyceride.
In the next step, we assessed the correlation between those variables, in which the changes were significant after bariatric surgery and hyperopic shift. Results in Table 3 show a significant correlation between refractive changes and systolic and diastolic blood pressure changes after surgery (p = 0.001), but there was no significant correlation between refractive changes and other indices (Fig. 2).
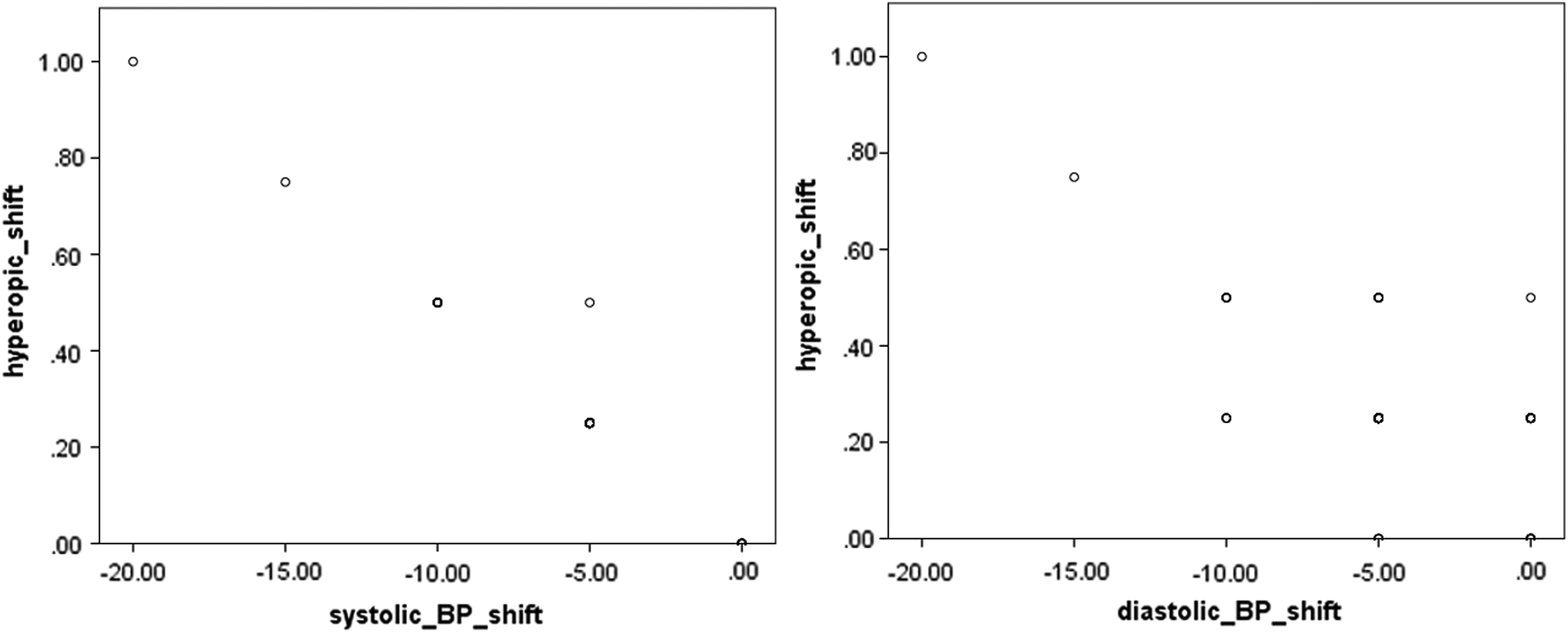
Scatter plots of hyperopic shift with changes in systolic and diastolic blood pressure after surgery.
Testing the Potential Correlations Between Refractive Changes and Changes in the Variables with Significant Difference Before and After Bariatric Surgery
Discussion
The present study investigated the effect of bariatric surgery on refractory errors of patients for the first time and the results of the ophthalmic examination of patients revealed myopic shift in 5 and hyperopic shift in 75 patients. Power analysis of the number of participants in the present study (0.8) showed adequacy of internal validity.
Some of these changes are attributable to the effect of excess fat that the patient had for many years before surgery. The factors that have been proposed as the possible underlying mechanism of ocular diseases in obesity include hyperleptinemia, hypoghrelinemia, and decreased nitric oxide (NO) in obese patients, associated with ocular diseases and increased IOP.6,22 In addition, the increase in the periorbital adipose tissue leads to increased IOP due to decreased episcleral flow. 23 However, this study was on the basis of optometric examinations, and measurement of IOP was one of the limitations in this study that need further research in future studies with ophthalmic approach.
Refractive errors are produced by the mismatch of the axial length of the eye with the focal plane, and refractive errors, especially myopia, have been associated with increased IOP.24–26 Age-related maculopathy has also been associated with obesity 3 and studies have found the association between maculopathy and obesity as well. 27 Thus, we hypothesized that the above-suggested mechanisms play a similar role in causing refractive errors in obese patients. However, as far as the authors are concerned, few studies have focused on the refractive errors in obese patients and the changes after weight loss.
Wong et al. concluded that refractive changes had no appreciable effect on the association of blood pressure and retinal vessel diameters, 28 but they did not evaluate the inverse effect. On the contrary, a study by Klein et al. revealed a significant direct correlation between changes in systemic blood pressures and changes in IOP. 29 Moreover, the results of Mi Jeung Kim's study revealed that higher IOP was significantly correlated with higher systolic blood pressure. 30 Indeed, these findings are in favor of the results of our study. The present study showed that decreasing systolic and diastolic blood pressure after metabolic surgery is in direct correlation with hyperopic shift among obese patients.
Bariatric surgery is called metabolic surgery as well, because it not only decreases weight significantly but also changes several hormonal mechanisms in the body, including ghrelin levels,31,32 reported to exceed the preoperational values 1 year after LRYGB. 33 NO is also reported to increase after metabolic surgery, 34 associated with ocular diseases,6,35 but these studies have not assessed obese patients. The present study was the first to evaluate refractory changes after bariatric surgery, and the mechanisms of this change can be further studied by molecular studies on animal models. Hence, the hypothesized mechanisms attributable to the changes in refractive errors could be the changes in ghrelin and NO and other hormones related to bariatric surgery. Also, as the present study indicated, excess weight and hyperlipidemia significantly decreased after LRYGB, affecting the interstitial fluid and periorbital adipose tissue associated with increased IOP due to decreased episcleral flow. 23
Studies that have reported ophthalmic complications have mainly determined nutritional deficiencies following bariatric surgery as the underlying mechanism.14–18 However, in the present study, the routine supplementation given to patients after surgery could prevent such disorders. As observed in Table 1, serum levels of most vitamins have increased postoperatively and no nutritional deficiencies were observed in our patients and no ocular diseases were observed 6 months postoperatively. In addition, the refractive errors of patients changed significantly in the present study, indicating the favorable effect of LRYGB, not only on excess weight and hyperlipidemic state of the patients but also on the refractive errors, especially according to the fact that myopia is a more prevalent refractive error, compared with hyperopia; the hyperopic shift after bariatric surgery can make the patients satisfied with the scope of decreasing corrective lens degree.
A limitation of the present study was the fact that we could not select a control group from patients who were not undergoing metabolic surgery, as patients in this BMI category require surgery; thus, we selected each patient as his or her own control in a before–after design to see the changes in refractive errors and strengthened the results by considering a number of patients with adequate power analysis. Yet, we could only hypothesize the possible mechanisms underlying this association, and studying the causative relationships requires further investigations.
Moreover, some studies have reported ocular complications many years after bariatric surgery, 36 but in the present study, patients were visited 6 months after surgery. Thus, longer follow-up is required to be able to justify the ocular status of patients following LRYGB. Furthermore, the present study revealed that there was a significant difference in BMI, ALK.PH, DBIL, and T3RU, between the two hyperopic groups (Hyperopic ≤+0.25 and Hyperopic >+0.25).
Conclusion
The significant changes in the refractive errors, especially hyperopic status of patients after bariatric surgery, along with significant reduction in BMI, serum levels of cholesterol, liver function test, and uric acid, suggest the necessity of further studies on the underlying mechanisms of ocular changes and their relationship to the metabolic changes of the patients who underwent bariatric surgery. The correlation between refractive errors and blood pressure changes makes the necessity of the researches in this field even more significant.
Footnotes
Acknowledgment
The authors of the present study sincerely thank the Research Deputy of Iran University of Medical Sciences. Funding: The present study was financially supported by the Research Deputy of Iran University of Medical Sciences.
Ethical Approval
The study protocol was approved by the Ethics Committee of Iran University of Medical Sciences (code: IRCT201202168588N2). The design and objectives of the study were explained to all participants and patients signed a written informed consent for participation in the study. All ethical considerations of the Declaration of Helsinki were met during the study.
Author Disclosure Statement
No competing financial interests exist.