
Abstract
Objective:
To compare safety and efficacy of laparoscopic gastric plication (LGP) and laparoscopic sleeve gastrectomy (LSG) for the treatment of morbid obesity.
Patients and Methods:
This prospective study included 40 morbidly obese adults scheduled for bariatric surgery and divided into two groups; LSG group (n = 20) and LGP group (n = 20). The patients were followed up for 2 years to assess weight, body mass index (BMI), and change in comorbidities. The procedure is considered failed if the BMI was >35 kg/m2 or the percentage of excess weight loss (%EWL) was <50% after 1 year, or weight regain was >10 kg above least weight after surgery. The primary outcome measure was the degree of weight loss and secondary outcome measures were postoperative complications.
Results:
LSG was superior to LGP after 1 year (p < 0.001) and after 2 years (p < 0.001). % EWL was significantly higher in LSG group at 6 months (p = 0.002), 1 year (p < 0.001), and 2 years (p < 0.001). Significantly more failures were recorded in the LGP group (p = 0.006).
Conclusion:
LSG has superior mid-term outcomes for weight loss and other parameters, but the LGP has lower cost with minor early complications and limited severe complications.
Introduction
O
Laparoscopic sleeve gastrectomy (LSG) has gained wide popularity to rank first among the bariatric procedures worldwide. 3 However, complication and reintervention rates of LSG are reported to be 5.6% and 3%, respectively. 4 Bleeding and leakage from the staple line are common postoperative events. 5 Staple-line leak is a severe complication of LSG with a rate between 0% and 5.5%. 6 It leads to severe clinical consequences or even mortality. 7 Also, LSG necessitates high costs because of using staplers. 8
Laparoscopic gastric plication (LGP) is another restrictive technique that was suggested as an alternative to LSG. Its potential advantages were technical ease, preserved stomach and the upper digestive pathway integrity, and lower operative cost. 9
At present, there is continuing debate on the use of LGP. The low cost of this procedure is a tempting advantage in developing countries as Egypt. Therefore, this study aimed to compare the safety and efficacy of two bariatric procedures, LGP and laparoscopic sleeve gastrectomy, for the treatment of morbid obesity. The ultimate goal was to offer an effective and less costly bariatric procedure to patients with limited resources.
Patients and Methods
This prospective study included 40 morbidly obese adult patients scheduled for bariatric surgery in the Departments of Surgery, Beni-Suef University Hospital and Kasr-Al-Aini Hospital, Cairo University during the period from January 2016 to April 2016. All patients had repeated failure of weight reduction after multidisciplinary medical treatment for at least 6 months. They were divided into two groups according to the type of bariatric procedure; LSG group (n = 20) had laparoscopic sleeve gastrectomy, and LGP group (n = 20) had LGP. The type of surgery was decided after full explanation of the procedure and its outcome and potential complications to all patients. The local Ethics Committee approved the study, and all patients provided a written informed consent to participate in the study.
Inclusion criteria were adults (>18 years of age) having a body mass index (BMI) >40 kg/m2 or BMI >35 kg/m2 associated with comorbidities (hypertension, diabetes mellitus, osteoarthritis), documented failure of weight loss attempts under medical treatment for a minimum of 6 months, and good enthusiasm for surgical treatment. Patients with obesity of endocrine origin, high risk for anesthesia, psychological diseases, previous gastric surgery, severe gastroesophageal reflux disease, or Barrett's esophagus were excluded from the study.
The routine preoperative evaluation was done, including respiratory function tests, abdominal ultrasonography, and ECG. Associated comorbidities were confirmed and documented.
Surgical technique
In all patients, after 15 mmHg pneumoperitoneum, five trocars were inserted with sizes of 5, 10, and 12 mm. When the greater curvature is exposed, the gastroepiploic gastric branches, short gastric, and posterior fundic vessels were divided starting at 4 cm proximal to the pyloric ring to the angle of His using the LigaSure device (Autosuture Bariatrics/Covidien). Once the greater curvature devascularization was completed, a 36 French bougie was introduced by the anesthesiologist to the stomach, and the surgeon guided it along the lesser curvature into the pyloric channel and duodenal bulb.
In LSG group
Stapling was performed starting at 4 cm proximal to the pyloric ring along the bougie. The gastric tubulization was performed by dividing the gastric corpus straight to the angle of His applying 4–6 cartridges of 3.8 mm 6 cm Endo GIA stapler. Instillation of saline with Methylene Blue by the anesthesiologist through the bougie after withdrawal of the bougie to the gastroesophageal junction was used to exclude visible leaks of the staple line. The resected specimen was removed through the 12 mm port.
In LGP group
Plication of the stomach is performed starting at 4–6 cm proximal to the pyloric ring using nonabsorbable monofilament polypropylene 2/0. Plication is done continuously in two layers.
Radiological examination with a Gastrografin swallow was performed on the first postoperative day to evaluate the gastric volume and to exclude postoperative leak before discharge from the hospital. Clinical evaluation of the patients was done monthly to assess weight, BMI, any change in comorbidities, and to modify the dietary regimen. An upper Gastrointestinal (GI) endoscopy (and gastric biopsy if needed) was done for assessment of any histopathological changes in the remaining gastric mucosa.
The procedure is considered failed if the BMI was >35 kg/m2 or percentage of excess weight loss (%EWL) was <50% after 1 year, or weight regain was >10 kg above least weight after surgery was recorded.
The primary outcome measure was the degree of weight loss at 6 months, 1 year, and 2 years postoperatively. This was evaluated by the %EWL. The secondary outcome measures were postoperative complications, including nausea, vomiting, leakage, and suture or staple line bleeding.
Statistical methods
Statistical analysis was done using IBM© SPSS© Statistics version 22 (IBM© Corp., Armonk, NY). Numerical data were expressed as a mean and standard deviation. Qualitative data were expressed as frequency and percentage. Chi-square test (Fisher's exact test) was used to examine the relationship between qualitative variables. For quantitative data, comparison between the two groups was done using independent sample t-test or Mann–Whitney test. Comparison of repeated measures was done using ANOVA. All tests were two-tailed. A p-value <0.05 was considered significant.
Results
The two groups were comparable in baseline characteristics (Table 1). A constant significant decrease in weight and consequently BMI was observed in the two groups up to the end of follow-up at 2 years. However, weight and BMI of the LSG group was significantly lower after 1 year (p < 0.001) and after 2 years (p < 0.001) (Table 2). As shown in Figure 1, the %EWL was significantly higher in LSG group at 6 months (p = 0.002), 1 year (p < 0.001), and 2 years (p < 0.001).
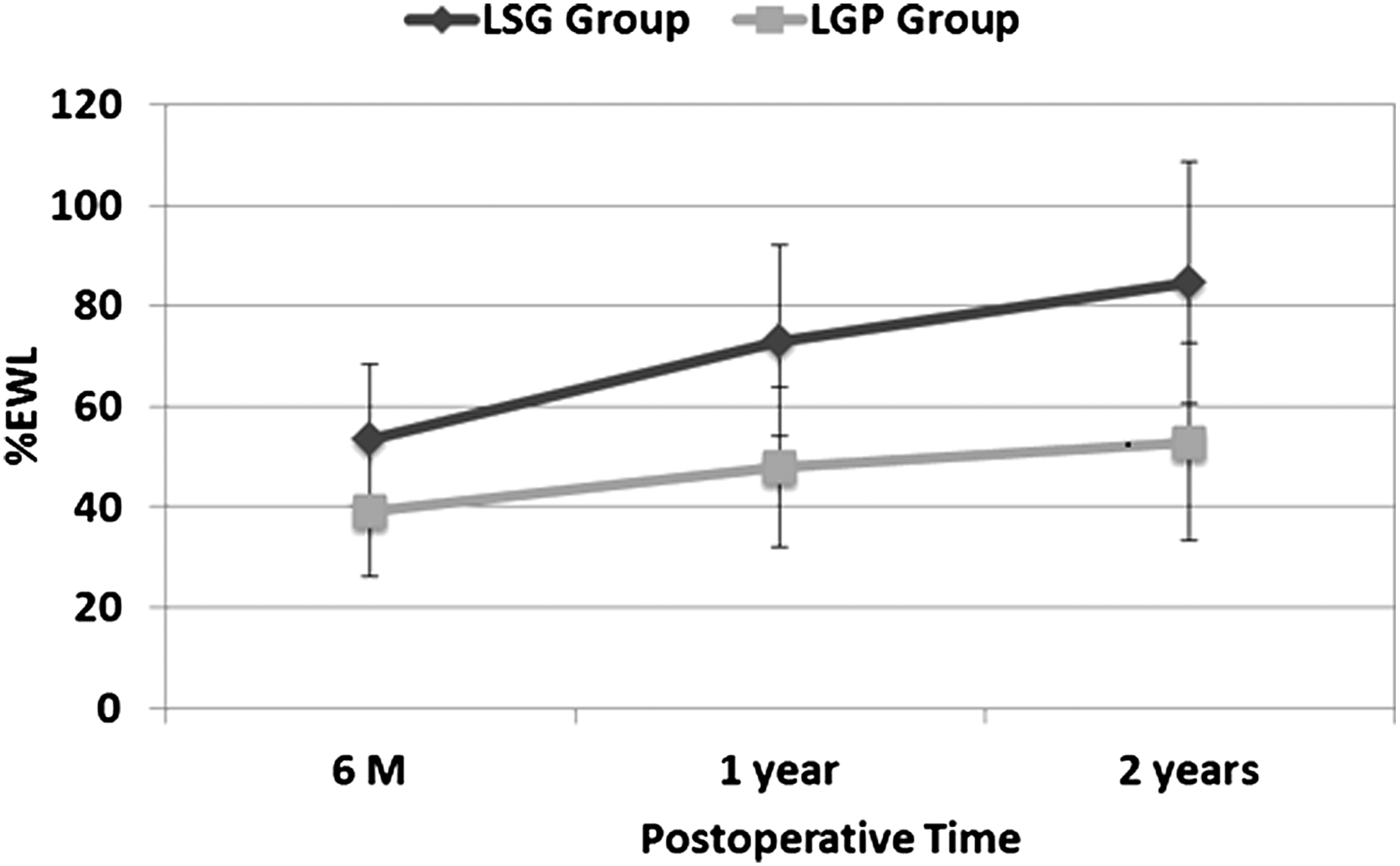
The percentage of excess weight loss during the first 2 postoperative years in the two studied groups.
BMI, body mass index; LGP, laparoscopic gastric plication; LSG, laparoscopic sleeve gastrectomy.
Hospital stay was significantly longer in the LGP group (p < 0.001). Nausea and vomiting occurred more commonly in the LGP group (p = 0.047). Significantly more failures were recorded in the LGP group (p = 0.006).
An unexpected iatrogenic event was recorded in LGP group due to unintentional injury to the liver by the Veress needle, which was treated by compression. Upper GI endoscopy revealed mild reflux esophagitis in two cases of the LSG group and one patient of LGP group, in addition to severe reflux esophagitis in another one. In LSG group, all patients had mild gastritis, expect two who showed severe gastritis (the two patients stopped medications). Two mortalities occurred in LSG group. The first was a 45-year-old female, diabetic, hypertensive, and asthmatic. She was admitted 1 month after discharge with fever, tachycardia, constipation, vomiting, and abdominal distension. She improved on conservative treatment and was discharged. She returned with the same picture after 2 weeks, where laparoscopic exploration revealed intraabdominal sepsis with no definite source. Suction and irrigation were done with the insertion of four intraperitoneal drains. The patient developed disseminated intravascular coagulopathy (DIC) and was admitted to the ICU, and then died. The second was a 45-year-old male, diabetic, and heavy smoker. He died with silent myocardial infarction 2 days after discharge (Table 3).
Discussion
This study demonstrated that LGP provided a gradual and significant decrease in weight and BMI up to 2 years in patients with morbid obesity. But, it was less effective compared with LSG in attaining short- and medium-term weight reduction. The main disadvantage of LGP was the high failure rate (50%) recorded after 1 year. Moreover, it was associated with higher rate of nausea and vomiting and more extended hospital stay compared with LSG. A crucial advantage of LGP was avoidance of extra costs imposed by staplers used in LSG.
Technically, in the current series, application of the linear stapler or gastric plication was started 4 cm from the pylorus to maintain the antrum that plays a vital role in the mechanism of gastric emptying. We believe that this can avoid delayed gastric emptying or gastric atony that could necessitate total gastrectomy.9,10
In this study, we did not detect any case of leakage in the whole studied group. Leakage is a severe complication of LSG; its rate in the current study was 0%. Also, no leakage was recorded in the LGP group, which supports the theoretical advantage of the procedure. In a large series of 800 patients, the rate of complications, including perforation was 0.6%. 11 Other studies reported few complications as well.12–14 A systematic review of seven articles found an overall complication rate of 8%; gastric leaks and perforations were reported in 1.6%. 15
Skrekas et al. 16 presented a series of 135 patients who underwent LGP using a technique similar to the current study. They reported reasonable effectiveness (65% %EWL), short operative time, and an overall complication rate of 8.8% in the form of vomiting, GI bleeding, and leak. Andraos et al. 17 reported short-term results of a series of 120 cases. They described early postoperative complications, including gastric obstruction due to fold invagination or edema, food intolerance, one case of leakage, and another one of gastric fistula.
Nausea and vomiting were the most frequent complications after gastric plication. 15 In the current study, 50% of LGP group developed this complication, which was controlled by prokinetics. Postoperative vomiting was the main cause of prolonged hospital stay in the plication group. Our policy in the postoperative follow-up was to keep patients under observation until complete recovery. Two patients reported continuous vomiting for several weeks after discharge with variable degrees of severity. Edema of the gastric wall always follows LGP, which may be the reason for most cases of postoperative vomiting. 8 Ramos et al. attributed these events to the restriction induced by the invagination of the greater curvature and/or edema caused by venous stasis. This was confirmed by endoscopic findings, where the greater curvature fold gets smaller by time, which may be caused by resolution of the initial edema. 12
Limitation of serious complications in LGP can be considered a forward step toward an ideal bariatric procedure. Another advantage was saving a considerable amount of money (near 14,000 Livre Egyptianne [LE]), which encourages its use in developing countries with limited resources. Despite these vital benefits, the relatively high failure rate is an obstacle in the way of adopting this simple and less costly technique. In the current series, a 50% failure rate was observed which is higher than what was reported by Skrekas et al. 16 (21.5%). In fact, the procedure achieved a reasonable average %EWL of 48.0% ± 15.9% after 1 year. Other investigators underscored this modest effect on weight loss with LGP.6,18 On the contrary, several previous articles reported higher %EWL following LGP compared with the current study.11,12,19
Therefore, we can conclude that LGP is a safe and feasible alternative for treatment of morbid obesity. It is characterized by minor early complications, and limited severe complications, that is, a safety profile similar to the more famed procedure, LSG. LGP appeared to be more efficient as it saves a great deal of money up to 14,000 LE. In areas like Beni-Suef governorate in Egypt, the latter advantage may be the most important given the limited income of the majority of its residents. LGP can be the best solution to treat morbid obesity to improve the lifestyle of these patients within their economic abilities.
Footnotes
Disclosure Statement
No competing financial interests exist.