
Abstract
Background and Objective:
Obesity is a chronic and epidemic disease that negatively affects the quality of life (QoL) and body image. Bariatric surgery (BS) has increased the QoL and positive changes in body image with weight loss. This study was conducted to assess the effects of changing body image and QoL of individuals who have undergone BS because of morbid obesity.
Methods:
This prospective study included 91 consecutive participants with morbid obesity. Data were collected using questionnaire and the Short Form 36 for QoL, body image questionnaire, and at four follow-up times: pre-BS, the first day post-BS, first month, and third month.
Results:
The mean age of the participants was 37.08 years. Pre-BS average body mass index was 48.52, it decreased to 36.20 at the third month post-BS. The average scores of gender and body image were higher in men than those of women; that the body image changed positively as a result of weight loss at the third month, and accordingly, the QoL increased. In the linear regression analysis, body image and QoL were found to be significantly related to physical functioning (β = 0.366, p = 0.000), role limitations because of physical health problems (β = 0.322, p = 0.002), and role limitations because of emotional problems (β = 0.404, p = 0.000).
Conclusions:
The results of this study showed that the BS changed the body image of the individuals positively, and this change in the body image created a positive impact on the QoL in early time after BS.
Introduction
Obesity is a serious and preventable health problem that has become a worldwide epidemic. Each year, 2.8 million people die as a result of being overweight or obese.1,2 It is reported that worldwide obesity has nearly tripled since 1975. According to World Health Organization report in 2016, >1.9 billion adults, 18 years and older, were overweight, and of these, >650 million were obese. Most of the world's population lives in countries where overweight and obesity kills more people than underweight. 2 In Turkey, the rate of obesity increased by 4.7% from 2008 to 2014, making it the country with the third highest prevalence of obesity in the world. 3
Obesity is associated with a significant number of medical and psychological health problems. These problems are closely related to an increased prevalence of noncommunicable comorbidities, including type 2 diabetes 4 ; hyperlipidemia; hypertension; heart disease; sleep apnoea5,6; musculoskeletal disorders, especially osteoarthritis, a highly disabling degenerative disease of the joints; and some cancers, including endometrial, breast, ovarian, prostate, liver, gallbladder, kidney, and colon, 1 which contribute to a decrease in life expectancy of 10 years or more. Therefore, obesity could be considered as a “spectrum” of disease, rather than an entity on its own. A study by Kuk et al. 2 found that the incidence of comorbidities and the mortality rate in morbidly obese patients was 1.7 times higher than that of normal-weight patients.
Both obesity and its associated comorbidities are the result of limited physical functioning (PF), poor self-esteem, and body dissatisfaction, leading to higher rates of depression and, consequently, decreased quality of life (QoL).7–9 Moreover, body image dissatisfaction is common in the obese population. 10 Today, the contour of the body is a common focus of attention; therefore, body image is affected negatively in the obese population.11,12 Body image is defined as how individuals observe or identify themselves when they look in the mirror or what they imagine or experience about their own physical appearance, including weight, height, body shape, assumptions, generalizations, and memories. A study conducted by Hamurcu et al. 13 showed that lower self-esteem and poorer body image are seen in obese persons compared with normal-weight persons.
To prevent obesity and associated comorbidities, for patients who have not successfully achieved lifestyle modifications such as diet, exercise, eating behavior modification or pharmacotherapy for weight loss, 14 bariatric surgery (BS) is the only treatment modality shown to provide consistent, sustained, long-term weight loss, decrease or reverse obesity-related comorbidities,15,16 and improve QoL and body image. Moreover, the mortality and morbidity rates with BS are very low. Therefore, BS is superior to other therapies as a management strategy for morbid obesity. 17 Some studies have determined that BS increases individuals' QoL18–23 and that positive changes in body image occur with weight loss.24–27 A study conducted by Nickel et al. 28 found that patients with morbid obesity have a significantly lower QoL and body image compared with the general population.
In general, there are many studies in the literature that involve changes in the QoL and body image of individuals after 6 months, 1 year, and 2 years in BS.8,18,20,21,27,33,36,40,41,45 However, both in Turkey and in world literature, no study seems to have emerged to indicate changes in the early period after BS. For this reason, in this study, we aimed to determine the effect of a change in body image on the QoL of individuals who have undergone BS because of morbid obesity, before BS, and on the first day, first month, and third month after BS.
Materials and Methods
Study design
A descriptive, prospective study was conducted in the general surgery clinic and general surgery policlinic of a university hospital in the Central Anatolia region of Turkey. In this hospital, BS was introduced in May 2015. The study population included 122 individuals who underwent BS in the general surgery clinic between 2016 and 2017. Therefore, during the planning of the study, BS had not yet been performed for 1 year in the institution. For this reason, the number of samples was determined taking into consideration the material aspect of basic component analysis. Thirteen individuals were excluded because they did not agree to participate in the study. However, 18 individuals did not want to continue the study for various reasons, the study was completed with a total of 91 patients. The inclusion criteria were age ≥18 years, being conscious, absence of orientation problems, ability to communicate, and consent to participate in the study. Data were collected using a questionnaire developed by the researchers to include demographic information, the Short Form 36 (SF-36), and the body image scale (BIS) through face-to-face interviews. The purpose of the study was explained to the participants and written informed consent was obtained. Each interview continued for ∼35–45 min.
Data collection and definitions
Three data collection tools were used in the study: (1) a questionnaire developed by researchers, (2) the SF-36, and (3) the BIS. Form data were collected pre-BS, on the first day post-BS, and in the first and third month post-BS. Forms were administered to the patients pre-BS and post-BS on the first day in the clinic room. The participants were invited to the polyclinic by phone for routine checks at the first and third month post-BS. The follow-up time was decided on the basis of knowledge of the literature and the observations and experiences of the researchers. There was no evaluation of body image and QoL on the first day post-BS in the literature, and in one study, body image and QoL were evaluated only in the third month post-BS. Although follow-up was performed at 6, 12, and 24 months post-BS in the literature, in this study, follow-up times were performed on the first day, and first and third month post-BS.
Before data collection, approval from the ethics committees of the university where the study was conducted and written permission from the institutional authority of the general surgery department were obtained.
Instruments
(1) Questionnaire form
The form was composed of 12 closed-ended questions selected from the literature by the investigators. They included the individuals' age, gender, marital status, weight, height, body mass index (BMI), duration of obesity before surgery, operation type, time of operation, postoperative problems, postoperative regret, and regular participation in postoperative physical activity.
(2) The Short Form 36
Developed by Rand Corporation in 1992, the SF-36 is a generic scale that provides wide-angle measurement within the life quality scales. The SF-36 includes one multi-item scale measuring each of the eight health concepts: PF (10 items), role limitations because of physical health problems (RP) (4 items), bodily pain (BP) (2 items), social functioning (SF) (2 items), general mental health (MH) (5 items), role limitations because of emotional problems (RE) (3 items), vitality (VT) (energy/fatigue) (4 items), and general health perceptions (GH) (5 items). 29 The SF-36 items and scales were constructed for scoring using the Likert method of summated ratings, excluding the fourth and fifth items, which are answered in yes/no format. For some of the Likert-type questions, inverse scoring was used. Instead of giving a single total score, the scale gives a total score for each subscale. The subscales assess health between 0 and 100 points, 0 indicating poor health status and 100, good health status. The SF-36 is divided into eight subscales to generate two summary scores. The physical health component summary score (PCS) consists of PF, RP, BP, and GH. The mental health component summary score (MCS) consists of RE, VT, MH, and SF. The reliability and validity of the Turkish version of the SF-36 was assessed by Koçyiğit et al. 30 in the Turkish version, the Cronbach's α coefficient was calculated for each subdimension and was between 0.73 and 0.76. In this study, Cronbach's α coefficient was found to be between 0.74 and 0.98.
(3) The body image scale
The BIS used in the study was developed by Secord and Jourand in 1953. The BIS consists of 40 items related to the substance or function of a body part or organ. Respondents use a 5-point scale, on which “1” represents “never” and “5” represents “always” to indicate the extent to which each item describes them. The total score on the scale ranges from 40 to 200. The higher the score on the BIS, the better the individual's body image. The cut-off score of the BIS is 135, and those who score below 135 are defined as the low-body image group. 31 The reliability and validity of the Turkish version of the BIS were assessed by Hovardaoğlu in 1989. 32 In the Turkish version of the BIS, the Cronbach's α coefficient was found to be 0.91. In this study, Cronbach's α coefficient was found to be 0.99.
Statistical analyses
Statistical analyses were performed using IBM Statistical Package for the Social Sciences (SPSS, version 22.0). Descriptive statistics (e.g., mean, standard deviation [SD], and frequency distributions) were generated for all variables. Demographic differences between treatment groups were tested using independent t-tests or Mann–Whitney U tests, as appropriate, for continuous variables and the Kruskal–Wallis H test for discontinuous variables. Student's t-tests were conducted to compare body image and QoL scores. Two-factor analysis of variance for repeated measures was used to determine the linear relationship between two variables. The Pearson product–moment correlation and the Durbin–Watson test were used to determine if there was a relationship between dependent variables. Finally, we carried out simple linear regression analyses for the two outcome variables, namely the SF-36 and BIS. The level of significance for all analyses was set at p < 0.05.
Results
A total sample of 91 (64 women [70.3%]; 27 men, [29.7%]) participants were assessed. Their mean age was 37.08 years (SD = 90; range: 19–58). The other demographic characteristics are given in Table 1.
Characteristics of Participants (N = 91)
BS, bariatric surgery.
There was no statistically significant difference in body image and QoL scores according to age, marital status, education status, family history of obesity, presence of obesity for several years before surgery, type of surgery, problems in post-BS, regret after surgery, and exercise participation post-BS. However, both body image and QoL scores in men were higher than in women at all follow-up times. Individuals with chronic disease had lower body image scores in pre-BS and on the first day post-BS, but their QoL scores were not statistically significantly different at any of the follow-up time points.
As given in Figure 1, as postoperative time progressed, body image, MCS, PCS, and BMI levels improved. The greatest change in PCS and on body image was mostly seen at the third month post-BS, and the least change was determined on the post-BS first day. In addition, BMI declined over time.
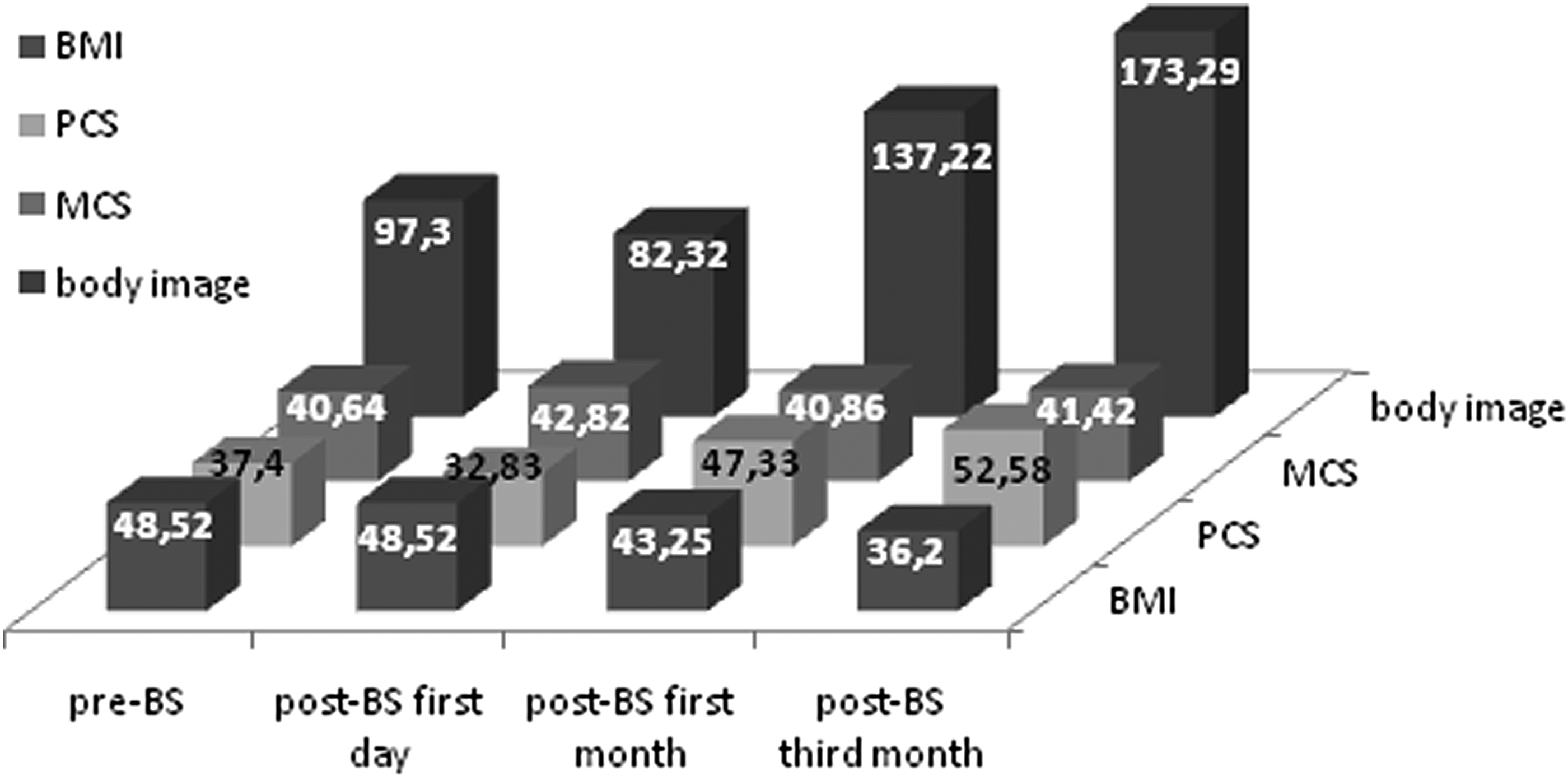
Relationship between participants body image, mental health component (MCS), physical health component (PCS), and body mass index (BMI) scores (N = 91). BS, bariatric surgery.
Table 2 provides the mean values of BMI, body image, and QoL scores before surgery at the various follow-up time points. As given in Table 2, there was a significant relationship between BMI and follow-up times. In addition, there was a statistically significant difference between the body image scores at the various follow-up times. On the post-BS first day, individuals' body image scores were decreased, but at the post-BS third month, they reached the highest level. There was a statistically significant between all subscales of the SF-36 and follow-up times, except the social function. In other words, there were positive changes in all sub-dimensions of quality of life except social function and body image.
Mean Values of Body Mass Index, Body Image, and Quality of Life Scores at the Following Times
BMI, body mass index; BP, bodily pain; GH, general health perceptions; MH, general mental health; PF, physical functioning; RE,: role limitations because of emotional problems; RP, role limitations because of physical health problems; SD, standard deviation; SF, social functioning; SF-36, Short Form 36; VT, vitality.
Bold indicates significant difference at p < 0.05.
Table 3 provides the results of simple linear regression analysis of the participants' body image and QoL. Body image and QoL were found to be significantly related to PF (β = 0.366, p = 0.000), RP (β = 0.322, p = 0.002), and RE (β = 0.404, p = 0.000). In addition, a negative relationship was found for BP (β = −0.264, p = 0.011). In other words, it was found that there was an increase in physical function, physical and emotional role difficulty and decrease in pain levels. These data included short-term follow-up, and explained that patients had difficulty in playing roles.
Simple Linear Regression Analysis Between Body Image and Quality of Life of Participants (N = 91)
SE, standard error.
Bold indicates significant difference at p < 0.05.
Discussion
BS is an effective treatment modality for morbid obesity because of its positive effects on body image and QoL, causing significant weight loss. This is the only study that found a positive effect of BS on both body image and QoL in the early period. Neven et al. 33 reported a significant improvement in body image over time post-BS, evaluated at 1–3 weeks, 6 months, and 1 year post-BS to examine the effects on participants' on body image. This study found a positive change in body image post-BS, and it was determined that the greatest change was at the post-BS third month. This result can be interpreted as a positive change in body image as a result of rapid weight loss in the 3-month post-BS period. Recently, a study conducted by Lindekilde et al. 41 to determine the effects of BS on body image found significant differences in recovery variables such as general body image, appearance evaluation, orientation, and body satisfaction between the pre-BS and post-BS third month time points. In concordance with our study, other studies33–38 found positive changes in body image after BS. In some studies conducted on this subject, the effects of BS on QoL or body image were evaluated 3, 12, and 24 months after BS. In this study, both body image and QoL were assessed on the post-BS first day. It is known that patients prefer BS to increase body image and QoL, and reduce comorbidity. For this reason, body image and QoL were evaluated on the post-BS first day to determine whether there were still positive thoughts related to BS. A positive impact on body image on the post-BS first day was not found. This result is interpretable as regret arose from deterioration in comfort as a result of postoperative pain, drains, and catheters.
In this study, it was determined that QoL improved significantly post-BS and this improvement was the highest in the post-BS third month. The focus of BS is on QoL rather than on weight loss, providing a patient-centered perspective.39–41 A study by Major et al. 20 found an improvement in patients' QoL post-BS. Similarly, Hachem and Brennan 39 showed that the QoL of patients followed up for 2 years post-BS increased significantly. Other studies evaluating QoL post-BS42–48 found increases in patients' QoL. It can be said that weight loss after BS reduces illness and improves the QoL by facilitating the activities of daily living and roles of individuals. It is known that both body image and QoL are lower in obese patients than in the general population. In a study conducted by Nickel et al. 28 to determine the effect of BS on body image and QoL, they found that QoL and body image improved significantly in the post-BS sixth month and remained stable for 24 months. In another study, from pre-BS to the post-BS 6, 12, and 24 months, it was found that body image and QoL improved with weight loss. 37 Similarly, in this study, it was found that the average of both body image and QoL scores increased from pre-BS to post-BS. In addition, in this study, linear regression analysis identified a relationship between body image and PF, RP, and RE of QoL.
In previous studies, body image was found to decrease with increasing BMI.49,50 Palmeira et al. 51 investigated the change in body image in 144 women with a mean BMI of 31.1 kg/m2 who were receiving nonsurgical obesity treatment. A significant difference was found between pretreatment and posttreatment body image: after 12 months, body image changed positively with the decline in BMI. In this study, there was a significant decrease in BMI and the average body image score increased from pre-BS to the post-BS third month. The results obtained from this study can be interpreted as follows: weight loss and decreasing BMI scores improve both body image and QoL through a positive change that occurs in the physical image.
Conclusions
In conclusion, it was determined that both QoL and body image improved with time after BS. This improvement was independent of age, marital status, education status, family history of obesity, presence of obesity for several years before surgery, and type of surgery. But there are statistically significant differences in terms of gender in favor of men. QOL and body image improved significantly within third month after BS. As the BMI decreased, MCS and PCS increased. Body image and QoL were found to be significantly related to PF, RP, and RE. In addition, a negative relationship was found for BP.
Limitations
The first author of this study is the first BS case in the institution. Therefore, this study is the first of its kind to be conducted in this institution. In addition, the follow-up period is short, and the number of samples is small.
In this study, phone number of the first author was provided to enable patients to be reached at any point if they had problems during the follow-up. The results demonstrated that most patients had a great need for knowledge. For this reason, it is important that patients receive counseling from nurse practitioners in this area. In addition, it was determined that patients wanted to meet someone who had undergone BS during the interviews. It is therefore recommended that a group of individuals be formed who have undergone BS under the guidance of an expert nurse in the institution. As weight loss after BS occurs over time, it may be advisable to perform studies to monitor body image and QoL with more people for longer periods of time. In the direction of all the results, it is important to determine the experience of patients who undergo BS.
Footnotes
Acknowledgments
Thanks to the volunteers who agreed to participate in this study.
Author Disclosure Statement
No competing financial interests exist.