
Abstract
Aim:
To analyze the value of serum myoglobin as an indicator of early acute kidney injury (AKI) after bariatric surgery.
Methods:
The medical records of 365 patients who underwent surgical bariatric procedures at our institution between December 2003 and December 2014 were analyzed. Preoperative creatinine, postoperative creatinine, and myoglobin levels were evaluated with regard to the occurrence of AKI following bariatric procedures. AKI is defined according to the KDIGO (Kidney Disease: Improving Global Outcomes) guideline.
Results:
Thirty patients (8.2%) developed AKI. Two of those patients developed AKI stage II, 1 patient AKI stage III, and 27 patients AKI stage I. AKI correlated with an elevated myoglobin levels in 28 of the 30 cases on the same day of the procedure, but only correlated with 24 of the 30 patients on the first postoperative day. Myoglobin levels were false positive in 79.8% of patients with measurements on the day of intervention and were also false-positive elevated in 65% of cases on the first postinterventional day. Hence, the determination of myoglobin levels is not superior to the determination of serum creatinine elevation for the detection of AKI after bariatric intervention.
Conclusions:
Measurement of serum myoglobin has no additional value for the detection of AKI after bariatric procedures compared with routine perioperative measurement of serum creatinine levels.
Introduction
The most effective treatment for morbid obesity is bariatric surgery. As the number of bariatric interventions is constantly increasing worldwide, a growing number and variety of postoperative complications can be observed. 1
One potentially severe early postoperative complication after bariatric procedures is rhabdomyolysis (RML). It is a condition in which skeletal muscle is broken down, releasing muscle enzymes and electrolytes from inside the cells. Generally, RML is rare, but it is well documented in obesity surgery. 1 Risk factors for causing RML are systemic metabolic conditions, such as ischemia and acidosis, as well as compartment syndrome and prolonged immobilization. In obese patients, the effect of gravity on the patient's supine body on the surgical table for the duration of the procedure can cause damage to muscle sarcolemma. The consequence is the leakage of intracellular contents into the circulatory system.2,3 These intracellular contents include electrolytes, myoglobin, and other proteins, such as creatine kinase, aldolase, lactate dehydrogenase, alanine aminotransferase, and aspartate aminotransferase.
The clinical outcome of RML is unknown. In most cases, asymptomatic elevation of serum muscle enzyme levels (such as creatinine kinase or myoglobin) is observed, but sometimes life-threatening conditions such as muscle necrosis, acute renal failure, electrolyte imbalance, and cardiac complications can occur. 1
The incidence of acute kidney injury (AKI) in RML is difficult to determine because of the varying definitions and clinical scenarios of this condition. The incidence of AKI ranges from 7% to 10% for all cases of RML in the United States. The exact number of patients who develop renal failure after RML is unclear but seems to be low. 3 Most of the studies investigating RML and AKI focus on RML as a consequence of drug and alcohol abuse, trauma, genetic defects, or metabolic or electrolytic disorders. Clinical trials concerning RML after surgery, in general, and especially after bariatric procedures, are rare. Due to the lack of larger studies on the subject, there is a void in exact data on incidence, morbidity, and mortality of acute kidney disorders in RML after bariatric surgery.
However, it is important to detect the signs of RML and AKI after bariatric surgeries early on. According to the data in previous studies,1–4 a monitoring system for the early detection of RML was established at our institution in 2003. It functions by measuring serum myoglobin levels in the first hours and days after every bariatric procedure performed.
The aim of this present study was to analyze the value of the serum myoglobin as an early indicator of AKI in the postoperative course after bariatric procedures.
Materials and Methods
Subjects
Between December 2003 and December 2014, 365 consecutive patients who underwent laparoscopic bariatric procedures at the Department of Surgery, University Hospital Mannheim, were included in this retrospective study. Bariatric surgery performed at our institution during the aforementioned time period included only laparoscopic procedures. Those procedures consisted of Roux-en-Y gastric bypass (RYGB), gastric sleeve (GS), biliopancreatic diversion with duodenal switch gastric banding, and gastric pouch reduction (remodeling). Of all the operations, 344 were RYGB and GS and thus constituted the most frequent procedures.
Inclusion criteria
Body mass index ≥30 kg/m2, combined with one or more comorbidities (diabetes, art. hypertension, sleep apnea, and others)
Informed consent to the operation
No history of psychopathological disorders, active drug dependence, bulimia nervosa, liver cirrhosis, or a lack of compliance
No pregnancy
Included in the study were 266 female patients and 99 male patients. According to the retrospective data, 356 patients had values for the preoperative serum creatinine, and 351 of them had at least 1 postoperative creatinine value. The myoglobin titer was measured on the day of the operation, after the procedure by 326 patients. There were 299 postoperative myoglobin values recorded on day 1 after the operation, 97 values on day 2, 37 on day 3, and 26 on day 4.
Definition of AKI
AKI was defined according to the clinical practice guideline: Kidney Disease: Improving Global Outcomes (KDIGO) (Fig. 1). 5
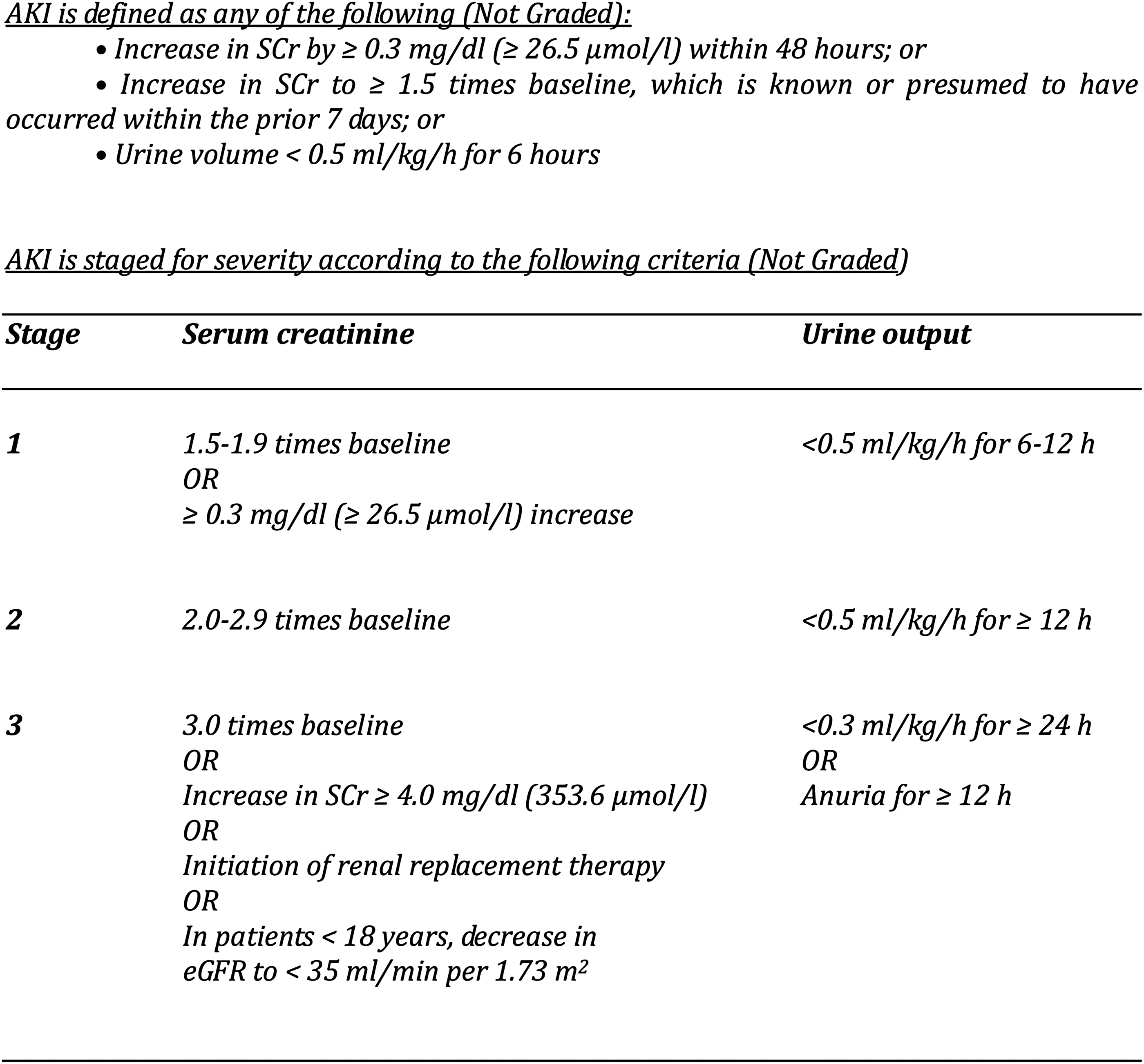
Definition of AKI according to clinical practice guideline: Kidney Disease: Improving Global Outcomes (KDIGO). AKI, acute kidney injury.
Statistical analysis
Statistical analysis was performed using the SAS software, release 9.3® (SAS Institute, Cary, NC). To compare two groups, the (chi-squared) χ2 test, two-sample t-test, or the Mann–Whitney U test were used. The Wilcoxon test for two paired samples was performed to investigate differences between two different time points. Furthermore, logistic regression analysis was performed to test myoglobin and creatinine as diagnostic markers. The test according to De Long has been applied for comparing the areas under the receiver operating characteristic (ROC) curves (AUC).
Results
Employing the KDIGO criteria (creatinine elevation of at least 0.3 mg/dL above the preoperative value), 30 patients (8.2%) developed AKI in the postinterventional course. None of those patients developed severe kidney failure. None of those patients required postoperative functional kidney replacement procedures (hemodialysis).
Two female patients developed a stage II AKI (twofold increase in baseline creatinine observed) and one female patient suffered from stage III AKI. Figures 2 and 3 show the perioperative changes of serum creatinine and myoglobin concentrations of those three patients.
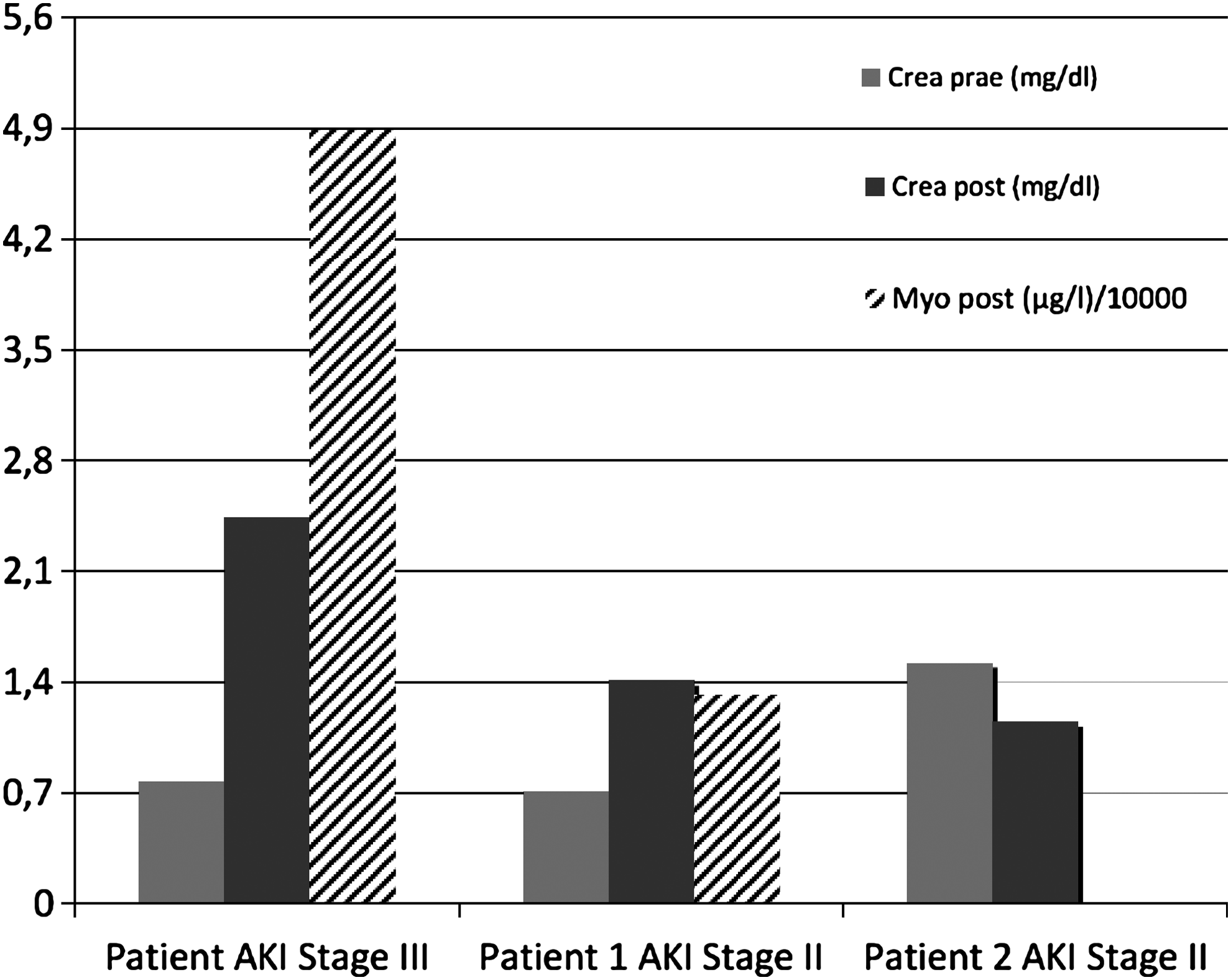
The serum concentrations of creatinine and myoglobin of the three patients with stage II and III AKI on day 1 after the operation.
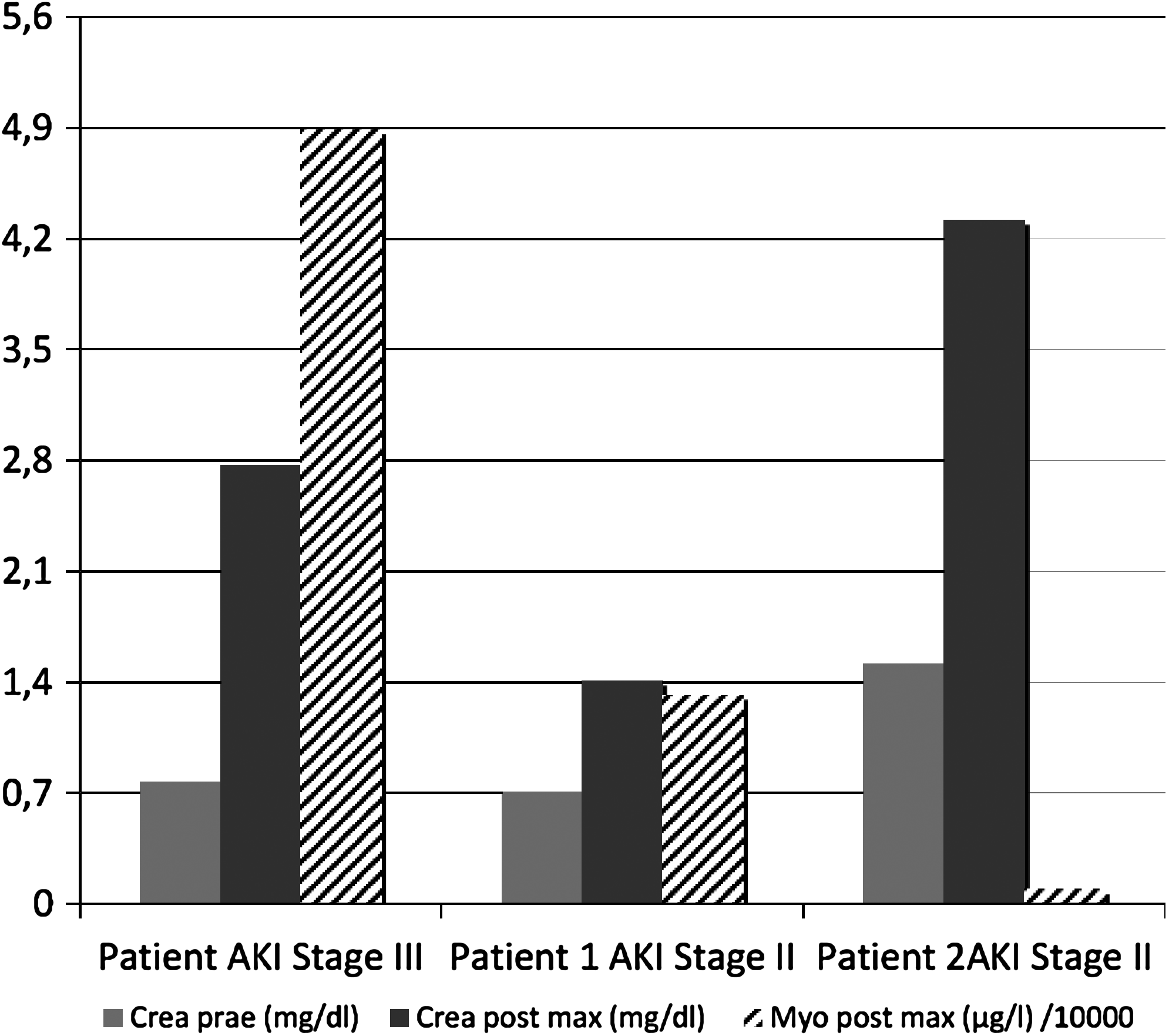
The highest postoperative serum concentrations of creatinine and myoglobin of the three patients with stage II and III AKI.
Of the 99 male patients, 17 developed AKI (17.1%) compared with 13 of the 266 (4.8%) female patients. The mean age of patients with AKI was significantly higher (44.7 ± 11.9 years vs. 40.3 ± 11.3 years; p = 0.0417).
According to the definition, all the 30 patients with AKI had a creatinine increase of at least 0.3 mg/dL. Applying the reference value for myoglobin (70 μg/L), 28 of the 30 patients (93.3%) with AKI also showed an increase of the serum myoglobin concentration on the day of the operation (hours after the procedure). On day 1 after the operation, only 24 patients showed persistent myoglobin concentrations higher than 70 μg/L, and 6 of the 30 patients with AKI (20%) had myoglobin levels under 70 μg/L. All the 30 patients with AKI had a determination of myoglobin levels on the day of the operation and also on day 1 after the operation.
In the group of 30 patients with AKI, myoglobin levels decreased from the day of the operation to the day after the operation (median values were 231.5 and 167.5, respectively; p = 0.0428). In these patients, the postoperative creatinine levels were significantly higher than the preoperative values (median values were 0.975 vs. 1.460, p < 0.0001). The median values on day 2 and day 3 were higher compared with the day of the procedure. Because of the retrospective setting of our study, there was only few myoglobin level available from day 2 and day 3 after the operation. For this reason, the statistical analyzability of those data is limited.
Of the patients who did not develop AKI after the procedure, the myoglobin levels were documented in 237 cases directly after the operation (day 0). On day 1 after the operation, myoglobin levels were available in most cases. For days 2, 3, and 4 after the operation, myoglobin concentrations were measured in 51, 16, and 8 cases, respectively. On the day of the operation, 79.8% of patients had myoglobin levels above the reference value (false positives in relation to creatinine elevation). At day 1 after the operation, there were 65%, and at day 2, 62%, false-positive elevated serum levels for myoglobin in comparison to serum creatinine levels.
Along the groups of the standard laparoscopic procedures, such as RYGB, GS, and the duodenal switch, there was no significant difference in the percentage of patients who developed AKI. All the 30 patients with AKI have had 1 of those 3 interventions. Figure 4 shows the distribution of AKI in every of those three groups.
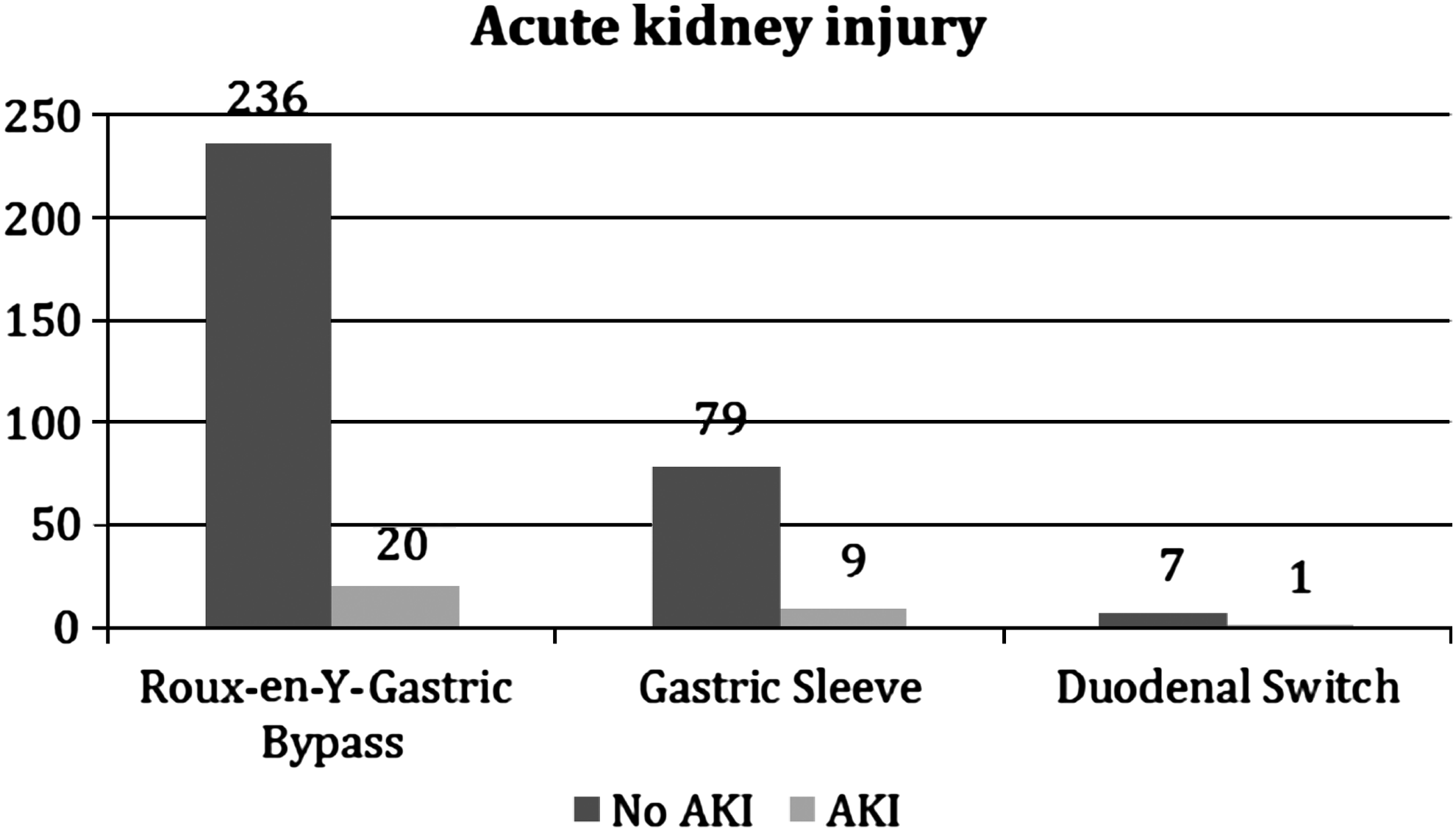
The absolute and the percentage distribution of AKI in the groups of patients, who underwent RYGB, gastric sleeve, and duodenal switch procedures. RYGB, Roux-en-Y gastric bypass.
In patients who developed AKI, the duration of surgery was significantly longer compared with patients without AKI (median 198 min vs. 160 min; p = 0.0038). Alternatively, there seemed to be no relevant difference in the type of procedure performed for AKI versus non-AKI patients.
Logistic regression analysis revealed that postoperative elevation of serum myoglobin levels (AUC = 0.677) did not show superior sensitivity with regard to the occurrence of AKI compared with the elevation of serum creatinine levels (AUC = 0.610; p = 0.4034) (Figs. 5 and 6).
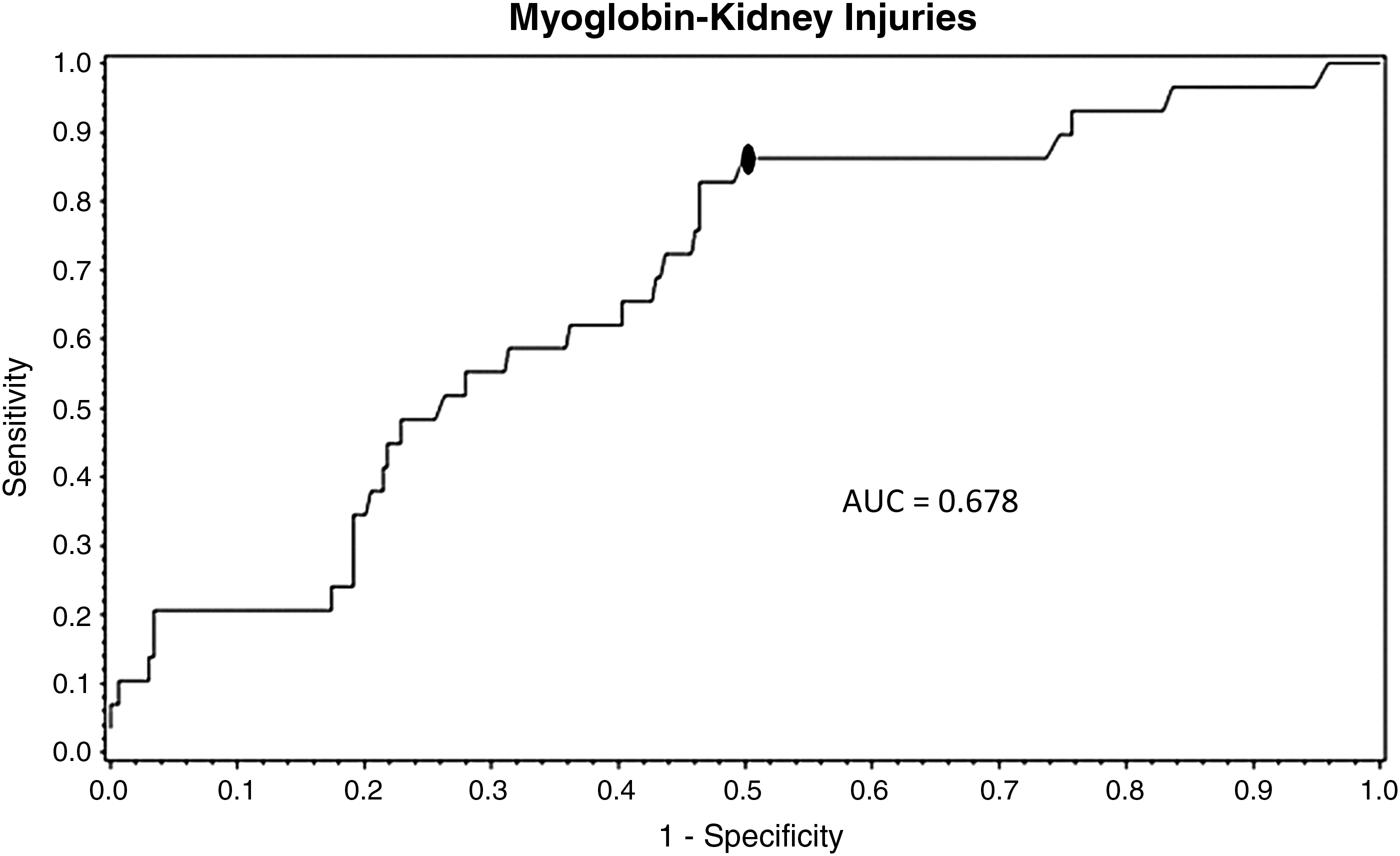
ROC for myoglobin as a predictor for AKI (sensitivity and specificity). ROC, receiver operating characteristic.
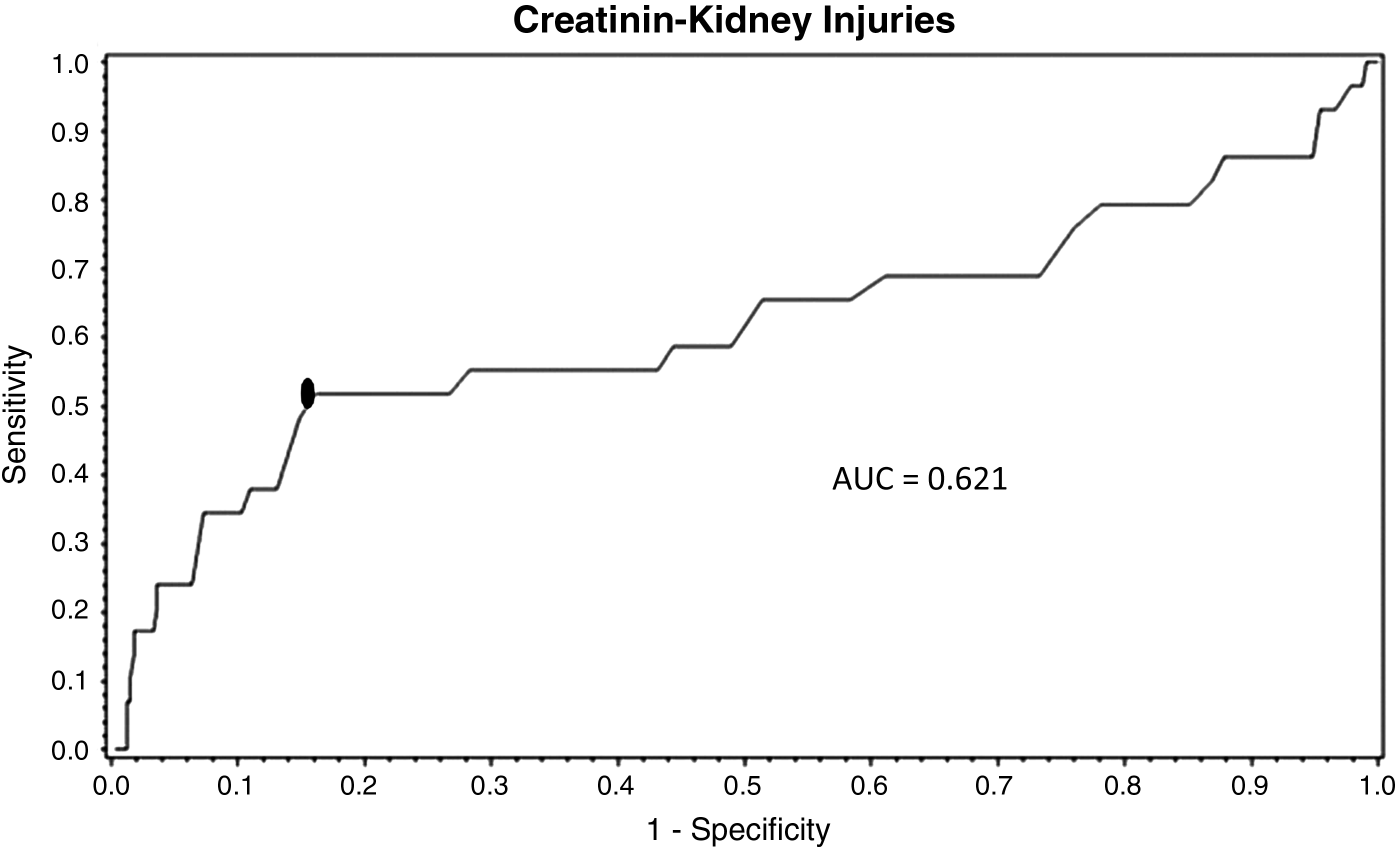
ROC for creatinine as a predictor for AKI (sensitivity and specificity).
Discussion
Postoperative AKI is a serious complication after bariatric surgery. Thakar et al. reviewed 504 patients undergoing RYGB and found that 42 patients (8.5%) developed a significant kidney injury. 6 Both RML and nephrolithiasis are known to be common factors in postbariatric surgery AKI. Our patient cohort shows a similar rate of AKI compared with the literature (8.2%), even if our patients underwent not only RYGB but also GS and other interventions. The rate of higher stage AKI in the Thakar study is low, compared with that in our data.
RML is the main reason for postbariatric AKI. In the literature (prospective trials), there are reports of rates from 22% to 77.3% of RML after bariatric surgery.7–15 The reported range can be explained by differing definitions used for RML. In some studies, RML is understood as any increase in myoglobin levels after a procedure, in other studies, only high levels of myoglobin with relevant kidney disorders were considered. In our opinion, it is important to differentiate between true perioperative RML (sarcolemic injury within myocytes, accompanied by kidney disorders) and asymptomatic hypermyoglobinemia without impairment of patients' postinterventional outcome.
To delimit RML with significant kidney injury to asymptomatic hypermyoglobinemia, we compared the predicting power of myoglobin levels after bariatric procedures. To the best of our knowledge, a comparison between these two routine laboratory parameters has not yet been established in bariatric surgery. In our cohort, no patient with AKI showed an elevation of myoglobin levels without an elevation of creatinine levels. Of the 30 patients with AKI, 93.3% of the patients on day 0 and 80% on day 1 had elevated myoglobin values. Furthermore, myoglobin was not capable of indicating AKI in a few cases during the first 48 h after the surgery (false-negative values). Almost 80% of the patients on day 0 and 65% of the patients on day 1 had false-positive elevated values of myoglobin with no AKI at any time after the surgery.
The findings in our study are compatible with the statements of Bosch et al. that myoglobin is subject to a rapid, but unpredictable, metabolism, probably due to the partial segregation through the liver or spleen. Therefore, measurement of serum myoglobin has a low sensitivity for the diagnosis of RML. However, AKI associated with RML often leads to a more rapid increase in plasma creatinine than other forms of AKI. 3
In the logistic regression analysis, both curves (ROC) for myoglobin and creatinine do not show significant differences in predicting the development of AKI. Therefore, myoglobin does not seem to be a superior predictor for AKI compared with creatinine. In clinical practice, the routine measurement of creatinine may be sufficient for detecting AKI after bariatric procedures.
In previous studies, operation time in bariatric surgery has been proposed to be a major risk factor for the development of RML.10,12 De Oliveira et al. noted a statistically significant difference between the surgery length, in minutes, in patients with RML (269.1 min) and those without RML (199 min; p = 0.009). 10 In our study, the duration of surgery was significantly longer for patients who had developed AKI, with a median length of 198 min versus 160 min in the patients who did not develop AKI (p = 0.0038). This concordant finding supports the hypothesis that pressure on the body's posterior muscles during surgery is a major factor in the development of RML after bariatric surgery. It should be considered that the length of operation time in earlier studies is appreciably longer than the expected operating time in bariatric centers for laparoscopic RYGB procedures today. 4 Because our study initiates in 2003, when our facility had only just begun conducting bariatric surgeries, the length of time for surgeries at the beginning of this study is long compared with the operation duration today. This considerable improvement in operating time reflects the learning curves for both the operating methodology and the surgical teams involved. Even operating times over 500 min for GS or RYGB procedures did not necessarily show a development of severe RML with kidney disorders. This fact shows once again, according to the understanding of Bosch et al., 3 that the metabolism of myoglobin is unpredictable and the hypothesis of damage to muscle sarcolemma during bariatric procedures is only one aspect and not a direct cause of the complex genesis of RML and AKI as a rare complication of this condition. There is not a straight proportional correlation between the duration of a bariatric procedure and the occurrence of RML and AKI.
In summary, there is a certain correlation between longer operating times and RML, but even a very long procedure duration does not necessarily lead to RML with the development of AKI after bariatric procedures. This is also reflected in the generally low incidence of RML.
As regard to the varying bariatric procedures, no difference in the risk of acquiring AKI was found. When observing even the most complex bariatric procedures, with longer operation duration (e.g., the duodenal switch), there was no association with a higher risk of AKI. However, the retrospective nature of our study, as well as the number of patients involved, does not offer a fully conclusive assumption about this correlation.
Limitations of the Study
An obvious limitation of our study is its retrospective design. Observing the data retrospectively did not allow us to have the same number of values for myoglobin and creatinine before and after the surgery, as were the number of patients.
Some of our patients, with high myoglobin values in the first hours and days after their procedure, were treated with nonstandardized intravenous fluid substitution. This aspect may have had an influence on the individual myoglobin or creatinine titer trends of some of the patients.
With 365 procedures in a period of more than 10 years, we represent the early time of our “growing” center, which has today significantly more than 100 patients per year. On the one side, this fact limits the power of our statement, but on the other side, it shows clearly longer operating times than usual nowadays, which seems to be important for this problem.
Our data acquisition has happened over a long period of time with a low number of cases and very long operating times at the beginning. Long operating times lead more often to RML and AKI. 16 On the one side, this constellation limits the power of our statement, but on the other side, it is beneficial to verify the reliability of myoglobin in terms of predicting AKI.
Conclusion
Myoglobin is a pathogenic factor in RML, a condition that can occur after bariatric procedures, and can cause AKI or even kidney failure. This clinical constellation is typically uncommon and cannot be detected early or reliably via routine measurements of myoglobin, due to the rapid and unpredictable metabolism of myoglobin. Hence, myoglobin is not a superior predictor of AKI compared with the usual clinical monitoring of creatinine after bariatric surgery.
Ethical Approval
This study protocol was reviewed and approved by the local institutional ethics committee. The study was performed according to the Declaration of Helsinki.
Statement of Informed Consent
Informed consent was obtained from all individuals (or “participants”) involved in this study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was created by the Department of Surgery (University Hospital Mannheim) and was not funded by external organizations.