
Abstract
Introduction:
The aim of the study was to adapt the Moorehead–Ardelt Quality of Life Questionnaire II (MA-II) into Turkish and validate it in bariatric patients.
Methods:
Special tools are needed to assess the impact of increasing worldwide obesity on quality of life. MA-II is a widely used tool to assess quality of life in obese patients. The scale adaptation standards of the World Health Organization were applied for translation and adaptation of MA-II. To test the validity, factor analysis, concurrent and predictive validity and to evaluate the correlation between MA-II and Short Form 36 Quality of Life Questionnaire (SF-36), the Pearson correlation coefficient was used. The reliability of MA-II was evaluated using internal consistency, item analysis, and test–retest methods.
Results:
The study was carried out with 185 adult patients undergoing planned bariatric surgery. MA-II confirmed the original factor structure with six items, and the factor loadings of items varied between 0.61 and 0.80. The Cronbach alpha coefficient of MA-II was 0.83, and the internal consistency of scale was found to be high. There was a statistically significant relationship between SF-36 and scale items. Furthermore, there was a statistically significant negative correlation between MA-II and body mass index.
Conclusion:
The Turkish version of MA-II is a valid and reliable tool for bariatric patients.
Introduction
Obesity takes part in the top five global risks in terms of mortality. 1 According to the data of the World Health Organization (WHO), in 2016, 650 million people are facing obesity. 2 Totally 19.6% of the population, which is 80 million people, are obese in Turkey. 3 It has been reported that obesity causes mortality in 3.4 million individuals, shortens the life expectancy by 4%, and increases the burden of disease by 4% worldwide. 4 Since obesity threatens the whole world, the treatment options of obesity have gained great importance. Nowadays, the most effective treatment of obesity is surgery.5,6 Bariatric surgery has been shown to be more effective than other methods of changing %total weight loss in reducing morbidity and mortality rates, increasing life expectancy, and improving the quality of life (class I, level A evidence).7,8
To improve the success rate and quality of life of patients after bariatric surgery, individuals must adjust to long-term lifestyle changes. 9 The patient's inability to adapt to lifestyle changes after surgery affects their life quality negatively by allowing the patient not to lose weight, as a result of which they develop various physical or psychosocial problems. 10 Herein, the evaluation of the quality of life begins to gain great importance. There is a need for a valid and reliable measurement tool in different languages and specific to the cultures of the area to embody the impact of bariatric surgery on the quality of life.
The Bariatric Analysis and Reporting Outcome System (BAROS) is an internationally used tool for assessing the results of bariatric surgery. This tool measures changes in body mass index (BMI) before and after bariatric surgery, surgical complications, comorbid diseases, and quality of life. The Moorehead–Ardelt Quality of Life Questionnaire (MA) was developed in 1998 to measure the quality of life of BAROS in all obese individuals. 11 The MA-II was obtained by revising the scale in 2003, with the recommendations of the surgical committee members in the reporting system, and by declaring the reliability and validity of the tool in English. 12 MA-II is recognized internationally. It has been increasingly used in many parts of the world. The strengths of the scale are that it is short, understandable, minimizes time loss, and each item supports the subject and decreases the bias that may arise from the interviewer. The scales, however, should be appropriate for their own language and culture in order to be fully understood. In Turkey, there is not a measurement tool that measures the quality of life after bariatric surgery. It is thought that the adaptation of MA-II into Turkish would cover the gap in the field. Therefore, the aim of the study was to adapt MA-II into Turkish and validate it in bariatric surgery patients.
Materials and Methods
Study design
This methodological study was conducted in bariatric surgery clinics of one private and two university hospitals. The purposive sampling method was used in the study. The study was carried out with patients who applied for bariatric surgery and those in the 3–12 months period after bariatric surgery. The pre- and postoperative groups consisted of different individuals. Participations—who were aged between 18 and 65 years, were volunteers, and had no disabilities in self-expression—were either patients being prepared for bariatric surgery (preoperative group) or invited after 3–12 months (postoperative group) of undergoing a bariatric surgery.13–15
Process of translation and adaptation
In adapting this methodological study to Turkish, the adaptation and translation procedures proposed by the WHO were followed. The recommendations of WHO consist of four stages, such as forward translation, expert panel back translation, pre-testing and cognitive interviewing, and giving the final version to the scale. Instead of exact translation, it is recommended to follow a path that ensures protecting the conceptual structure, reaching the widest audience, avoiding the technical terms/unspoken vocabulary groups, and discussing the incomprehensible or inadequate statements about translation in the expert panel. Within the pilot application, testing the scale on targeted individual group and finalizing the characteristics of the scale according to the recommendations are essential 16
In our study, first of all, the scale was translated from English to Turkish by a health care professional whose native language is Turkish and who has a good comprehension of both languages, cultures, and terminology. Second, inadequate or incoherent expressions in the language of translation were reviewed, and arrangements were made in the panel of experts with a health professional, advisor, translator, and translator under oath. Third, the back-translation was carried out by an independent translator who had no idea about the scale but had a good comprehension of the two languages and cultures. After the pre-testing with 15 patients and cognitive interviewing, the scale was finalized.
After the adaptation process of the MA-II, 12 experts were interviewed for content validity. The Turkish form of the scale was evaluated in terms of whether it served the stated purpose and its suitability to the Turkish culture. Content Validity Index (CVI) was used for consistency of expert scores. The research was approved by all institutions where the research was conducted. Ethics committee permission was obtained. Permission was obtained via e-mail for using MA-II and Short Form 36 Quality of Life Questionnaire (SF-36). Written informed consent was obtained from all participants.
Data collection tools
Data in this study were collected by “Moorehead–Ardelt Quality of Life Questionnaire II,” “SF-36,” and standard questions covering age, gender, marital status, and BMI (kg/m2).12,17 MA-II consists of six items, which are self-esteem (Q1), physical functioning (Q2), social relationships (Q3), working ability (Q4), sexuality (Q5), and eating behavior (Q6). Each item has a 10-point Likert-type measurement and is equally burdened. The total score of MA-II (from −3 to +3) was obtained by collecting the scores of each item, and higher scores indicated that the quality of life was well perceived. The original language of the scale is English. It has been adapted and validated in eight languages, including Czech, German, Italian, Spanish, Taiwan, Greek, Portuguese, and Korean.13–15,18,19
SF-36 is a scale that can be applied to all age groups for evaluating the quality of life. The scale consists of 36 items and eight subdimensions. These subdimensions are the physical function, social function, physical role limitations, emotional role limitations, mental health, vitality, bodily pain, and general health.17,20
Statistical analysis
The mean scores of the scales were used to evaluate the validity of MA-II in Turkish; factor analysis and known group comparison were used for evaluating content and construct validity. Concurrent and predictive validity analyzes were used for criterion validity. In assessing the validity of the content, CVI was evaluated; in assessing the validity of construct, confirmatory, explanatory factor analysis, and in the comparison of the known group, the MA-II total score between the pre- and postoperative groups was evaluated by t-test. The criterion validity was evaluated by Pearson correlation analysis between MA-II and SF-36, and the predictive validity was evaluated by multivariate linear regression analysis between MA-II total score and demographic variable.
Test–retest method, internal consistency, and item analysis were used to evaluate the reliability of the scale. Pearson correlation for the test–retest method and item analysis and Cronbach alpha coefficient for the internal consistency were applied.
Results
Patients
The study was carried out with 185 patients (60 preoperative, 125 postoperative) who met the inclusion criteria between February and July 2017. Descriptive and clinical characteristics of the patients who participated in the study are shown in Table 1.
Study Population Characteristics, Scores of Moorehead–Ardelt Quality of Life Questionnaire II, and Short Form 36 Quality of Life Questionnaire
p < 0.01.
BMI, body mass index; MA-II, Moorehead–Ardelt Quality of Life Questionnaire II; MCS, mental component summary; PCS, physical component summary; SD, standard deviation; SF-36, Short Form 36 Quality of Life Questionnaire.
Validity analysis of MA-II
After the translation was completed, the scale was evaluated by 12 experts in terms of language/expression suitability and content suitability. On behalf of evaluating language/expression suitability, Item-Level Content Validity Index (I-CVI = 0.91) and Scale-Level Content Validity Index (S-CVI = 0.93) were calculated; with regard to the content suitability, I-CVI was 0.91 and S-CVI was 0.96.
Structural validity of Turkish version of MA-II was tested. Accordingly, the scale consists of a single-factor structure and six items. It was seen that the standardized coefficient of the scale was 0.53–0.75; error variances of the scale changed between 0.43 and 0.72 (Table 2 and Fig. 1). All these results revealed that MA-II confirmed the original factor structure.
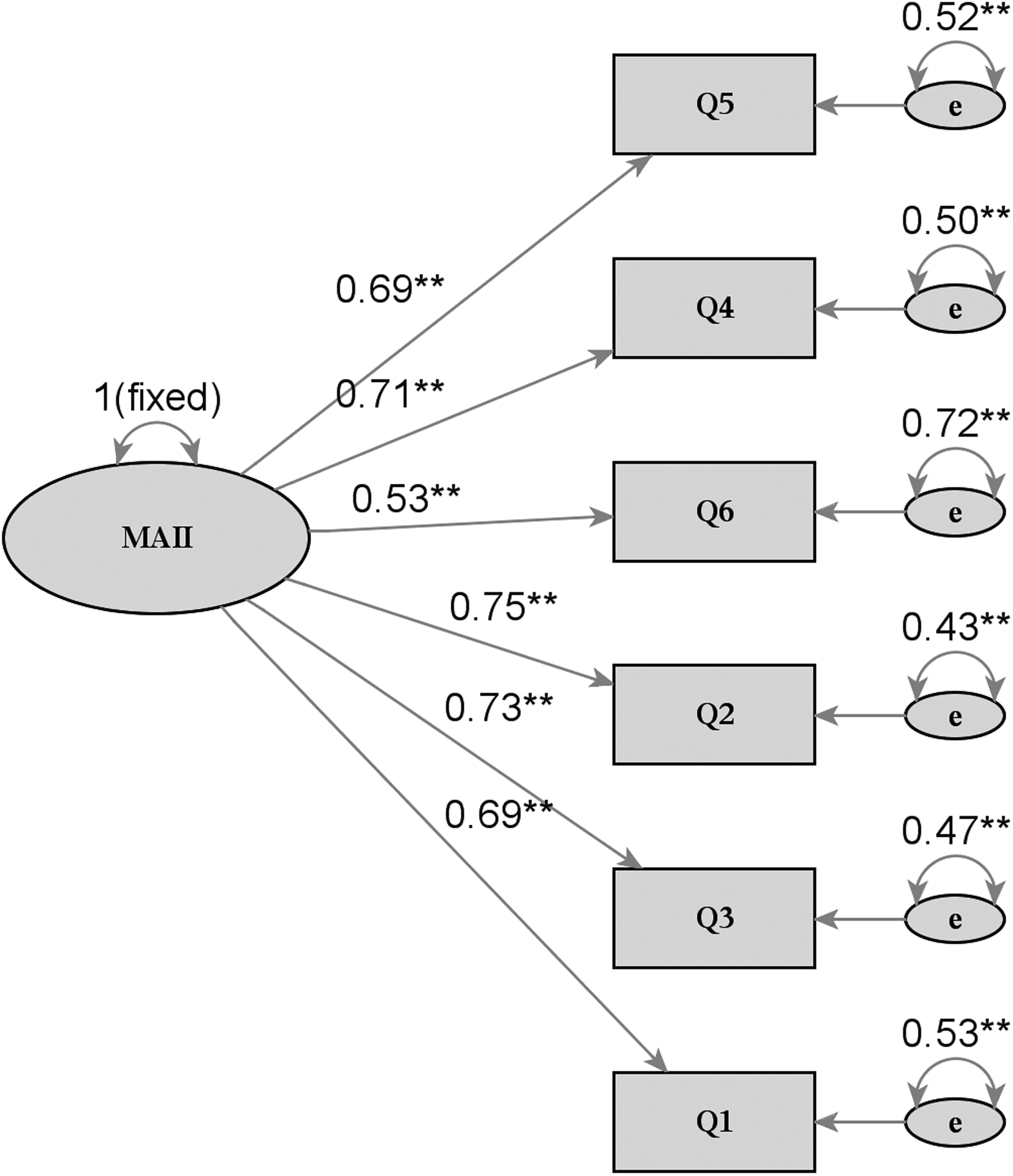
Turkish version of MA-II: confirmatory factor analysis structural model. MA-II, Moorehead–Ardelt Quality of Life Questionnaire II.
Confirmatory Factor Analysis of Moorehead–Ardelt Quality of Life Questionnaire II (N = 185)
Before explanatory factor analysis, since KMO coefficient was found to be 0.86 (>0.50) and Barlett's test was found to be statistically significant (χ 2 = 344.254; p = 0.00), the sample was concluded to be suitable for factor analysis. The factor loadings of scale items ranged from 0.61 to 0.80, and it was determined that the scale explained 55.63% of the variance desired.
Pre- and postoperative MA-II total scale scores were compared with those of the known groups. In the analysis, the postoperative MA-II scores of the patients were higher than the preoperative values. In addition, there was a statistically significant difference between the pre- and postoperative groups and MA-II total scores (p = 0.000) (Table 3). For the concurrent validity of MA-II, the correlation with SF-36 was examined, and the results are shown in Table 4.
Known Group Comparison of Moorehead–Ardelt Quality of Life Questionnaire II (n = 185)
Correlation Between Moorehead–Ardelt Quality of Life Questionnaire II and the Short Form 36 Quality of Life Questionnaire Health Survey
p < 0.01; bp < 0.05.
In the investigation of the predictive validity of MA-II, age was excluded from the model as a result of regression analysis, and statistically significant effects were found between MA-II total score and surgical status, gender, BMI (Table 5). In addition, there was a negative and moderate degree of correlation between BMI and MA-II total score (r = −0.457, p = 0.0001), and this relation was found to be statistically significant (Fig. 2).

Scatter plot for BMI against MA-II total sore. BMI, body mass index.
Multivariate Linear Regression Model For Moorehead–Ardelt Quality of Life Questionnaire II Total Score
Linear regression model of MA-II total score (dependent variable) using surgical status (post- and preoperative), gender (female and male), and BMI (continuous variable) as independent predictors.
Reliability analysis of MA-II
While Cronbach's alpha coefficient for all patients was 0.83, it was found to be 0.77 for the patients in the pre- and postoperative periods. For item analysis, a high degree of correlation (0.651–0.804) was found between the item scores and the total score correlations. MA-II was re-administered to 73 patients 2–4 weeks after the application of questionnaire and test–retest reliability was verified. As a result, r = 0.655 was found and the correlation was found to be statistically significant (p = 0.000).
Discussion
It is clear that obesity leads to negative consequences in the health status of individuals and deteriorations in the quality of life.21,22 The effect of obesity on the quality of life can be evaluated with a disease-specific, reliable, and validated scale. Determining the quality of life and evaluating the effects of bariatric surgery is an important parameter in the fight against obesity. It is also useful in establishing the guidelines for clinical pathways and in deciding on health policies. 23 Quality of life, however, is influenced by changing situations as well as by subjective, psychological, economic, and cultural factors. Because of these reasons, quality of life is very difficult to define and measure. 24 Therefore, the instrument should be appropriate to the language and culture of the target population.
There are a variety of tools to assess the quality of life of obese patients. MA-II is short and easy to understand and apply. Supporting each item with relevant symbols will help reduce the bias that may arise. Some studies showed that the impact of weight on quality of life-lite questionnaire (IWQOL-Lite) is preferred in the literature in recent years, but the scale is especially suitable for measuring the quality of life of persons with extreme obesity. However, MA-II is a suitable scale for obesity before and after bariatric surgery.25,26
One of the most important stages of scale adaptation is the provision of language validity. To adapt the scale into Turkish according to WHO levels, forward translation, expert panel, backward translation, and pilot test steps were applied. In the Greek, Czech, German, Italian, and Spanish versions where the validity of the scale has been tested, pilot test was not performed, while in Taiwan, Czech, German, Italian, and Spanish, it is seen that there was no backward translation.13,14,19
In the data collection process, it is seen that the sexuality question of MA-II was not answered by sexually inactive individuals. The validity and reliability study of the Czech, Italian, German, and Spanish versions of the scale also reported the same problem. 14 The reason why the sexuality question was not answered by some individuals in our country is that the age of onset of sexuality is late, that monogamy is at the forefront, and that individuals whose spouses are deceased or who are divorced may not be sexually active.
The MA was originally developed within the scope of the development of BAROS, but it was decided to have five items (self-esteem, physical activity, social life, working status, and sexuality) without going through a factor analysis method. 11 With the addition of nutrition perception to the scale by Moorehead et al. in 2003, the scoring was revised. The MA-II was published as a single-factor, six-item scale and can be applied to the pre- and postoperative groups. 12 This structure of the scale was also confirmed in the Turkish version by factor analysis.
To determine whether the MA-II total score was different in the pre- and postoperative periods, a known group comparison was implemented. As a result, it was seen that the quality of life of patients increased after the operation, and it was confirmed that the operation had a positive effect on the quality of life (Table 3). The findings highly correlated with the literature.27–30
It was seen that the subdimensions of physical function and general health perception of MA-II and SF-36 had moderate or high positive correlations with all languages in which validity and reliability was evaluated. Social function was moderately positively, statistically significantly correlated in all languages except Czech and Spanish; role limitations due to physical problems were weakly or moderately positively statistically significantly correlated in other languages than English; role limitations due to emotional problems were weakly or moderately positively statistically significantly correlated in all languages other than Spanish. In addition, mental health was weakly or moderately positively statistically significantly correlated in languages other than Italian; energy was weakly, moderately, and highly positively statistically significantly correlated in all languages except Italian; pain showed a moderate negative correlation in Turkish and English, whereas in other languages there was a weak or moderate positively statistically significant correlation. Negative correlation with pain emphasizes the negative impact of pain on the quality of life.12–15,19
It was found that the patients' pre- and postoperative status, gender, and their postoperative BMI had significant effects on the MA-II score, and this effect was statistically significant. A negative moderate correlation was found between BMI and scale scores. In other words, the higher the BMI of patients, the lower their quality of life. In all languages of the scale, including Korean, Portuguese, Greek, Taiwan, Czech, German, Italian, and Spanish, the increase in BMI correlated negatively with the MA-II score.13–15,18,19
In the literature, while the lowest Cronbach alpha coefficient of MA-II was found to be for Korean with 0.76, the highest was seen for German with 0.88.14,15 It was seen that the adaptation and validation of the scale was reliable in all languages. In this study, the Cronbach alpha coefficient of the Turkish MA-II was found to be 0.83. In this context, the Turkish version of MA-II is a highly reliable tool. The Cronbach alpha coefficient was assumed to be low in Korea because the sixth item of the scale (The way I approach food is: I live to eat/I eat to live) caused negative emotions in morbidly obese patients. It is stated that due to the attitude of the Korean people toward obese individuals, social pressure, and discrimination, these individuals did not eat especially in public places. It is emphasized that the approach to food should be carefully investigated and evaluated because of the differentiation of the culture. 15
The item–total score correlation in MA-II was found to be positive and high. The lowest correlation in the scale (0.651) was for the sixth item (The way I approach food is: I live to eat/I eat to live), while the highest correlation (0.804) was determined for the second item (I enjoy physical activities: Not at all/Very Much). In the Korean version of the scale, item–total score correlations were calculated between 0.432 and 0.833. 15
Conclusions
As a result, the scale is a valid and reliable instrument in Turkish, suitable for both pre- and postoperative patients. The MA-II can be applied before and after at least 3 months of bariatric surgery. It is suggested that the scale should be used by health professionals to determine the areas that affect the quality of life of individuals before and after bariatric surgery, to record their quality of life, and to integrate the scale into the patient follow-up form in the clinic. Patients after bariatric surgery experience many changes in many aspects, including physical and psychological deviations. The MA-II is disease-specific and more sensitive to changes in patients' experiences. Therefore, it plays a vital role in the follow-up of changes in patients' life and in the concretization of bariatric surgery results in terms of quality of life. Although there are many tools with which the quality of life can be measured, the MA-II is one of the most widely used tools due to its sensitivity to change and suitability for clinical practices. The fact that the short, single-page scale plays an important role in terms of cost-effectiveness and time management, the inclusion of the figures and easy understanding are fundamental in terms of eliminating intercultural variations.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval for this study was granted by the Akdeniz University Faculty of Medicine Ethics Committee for Non-Interventional Clinical Research (70904504/397).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Acknowledgments
This article was based on the master's degree thesis of the first author under the supervision of the second author. We are grateful to all the individuals who participated in our research. The authors would like to thank Elisabeth Ardelt-Gattinger who allowed the Turkish version of the MA-II, and Mehmet Ziya Fırat (Prof. Dr.) who provided statistical expertise. In addition, this research was supported by the Akdeniz University Scientific Research Projects Coordination Unit with the project number of TYL-2016-1971.
Authors' Contributions
F.C. and D.A. were responsible for the study conception and design. D.A. performed data collection. F.C. and D.A. and the statistician provided data analysis. F.C. and D.A. were responsible for drafting the article. F.C. supervised the study.
Author Disclosure Statement
The authors declare that they have no conflict of interest.