
Abstract
Introduction:
Roux-en-Y gastric bypass (RYGB) is the gold standard bariatric procedure for morbid obesity. Most patients who undergo this procedure in the United Kingdom are females, commonly of childbearing age. The resultant rapid weight loss is associated with improved ovulatory function and patients commonly regain fertility postoperatively. This study reports published cases of intussusception during pregnancy as a complication that can occur following RYGB.
Materials and Methods:
A complete literature search was performed using PubMed/Medline using the keywords “pregnancy,” “intussusception,” and “gastric bypass.” Further works were added following a manual search of references contained within the relevant identified articles. Patients who had undergone an open or laparoscopic RYGB and later developed small bowel intussusception during pregnancy were included.
Results:
Thirteen females with a mean age of 30.4 years were identified across 11 case reports. Intussusception occurred at a median of 4 (range 1–14) years following surgery. All patients presented with abdominal discomfort, with 85% experiencing vomiting also. CT and MRI scans confirmed intussusception in all seven cases in which they were used. In contrast, ultrasound was diagnostic in only one of five patients. The remaining five cases were diagnosed intraoperatively. Ten patients ultimately required resection of the affected portion of small bowel, while only three were successfully managed with reduction alone. No maternal mortalities occurred across these cases. One infant died following postoperative delivery.
Conclusion:
Intussusception is a rare, but serious, complication following RYGB. Presenting symptoms are often vague and nonspecific. A high index of clinical suspicion is, as such, required. It is not yet clear whether pregnancy represents an independent risk factor for intussusception.
Introduction
Laparoscopic Roux-en-Y gastric bypass (RYGB) is considered the gold standard bariatric procedure for morbidly obese patients. Over 75% of patients who undergo this procedure in the United Kingdom are females, commonly of childbearing age. 1 Obesity is not only a considerable risk factor for maternal and neonatal morbidity but is also known to decrease chances of conception. 2 The resultant rapid weight loss associated with bariatric surgery is often associated with improved ovulatory function and patients commonly regain fertility postoperatively.3,4 Furthermore, bariatric surgery is known to generally lead to favorable outcomes during pregnancy; however, specific nutritional and surgical complications can occur. 5 In particular, malabsorptive bariatric surgeries have been linked to an increased risk of fetal growth restriction.6–9 This has, in part, led to guidelines advising patients to avoid becoming pregnant for 12–18 months following bariatric procedures, 10 thus avoiding the time period of most rapid weight loss. The optimal timing of conception following bariatric surgery is not yet known.4,11–13
A number of pregnant patients have experienced complications that have been linked to prior bariatric procedures. In addition to those attributed to nutritional deficiencies, a range of surgical complications has also been observed in this patient cohort. These include cases of small bowel obstruction, most commonly secondary to internal hernias.13,14 Intussusception has also been described as a rare complication following RYGB, with a reported incidence of 0.1–0.3%. 15
In this article, we will review the published literature describing intussusception following RYGB in pregnant patients and discuss the current understanding of this rare, but serious, complication.
Materials and Methods
Methodology
A complete literature search was performed using PubMed/Medline using the keywords “pregnancy,” “intussusception,” and “gastric bypass.” Further works were added following a manual search of references contained within the relevant identified articles. We included literature published in both English and French (Fig. 1).
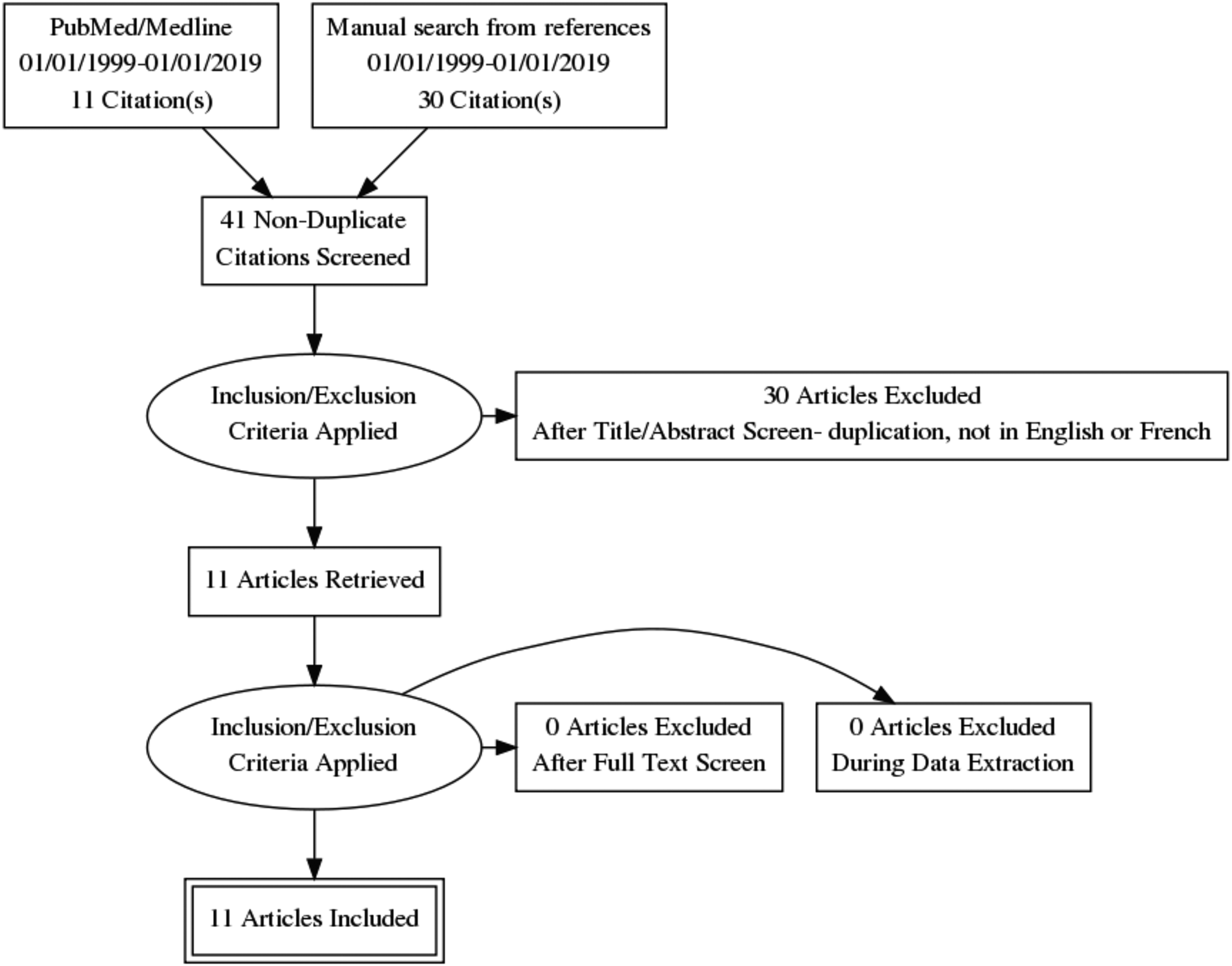
Literature search result flow diagram.
Patients were included who had undergone an open or laparoscopic RYGB and later developed small bowel intussusception during pregnancy. While many had imaging performed beforehand, in all cases, intussusception was confirmed during surgical exploration.
Some reports were written with an obstetric or radiological focus and, as such, do not provide readers will all of the pertinent information. In all cases where complete data were not available, means, ranges, and percentages are calculated from the patients where details are known.
This review focuses on characteristics of these patients and the weight lost between RYGB and intussusception (Table 1). We evaluate how this complication presents and the diagnostic and treatment modalities utilized.
Summary of Cases Within the Existing Literature
Presented as weeks. All other measures of time presented in years.
Median age reported between two cases.
RYGB, Roux-en-Y gastric bypass.
Results
Patients
A total of 13 females were identified across 11 case reports.2–12 The mean age at presentation was 30.4 (range 24–37) years. Ten patients had previously undergone laparoscopic RYGB. In three cases, it was not stated whether this had been performed laparoscopically or by open surgery. 15 Intussusception occurred at a median of 4 years following surgery. This ranged from 1 to 14 years. Four case reports described the weight loss following surgery.17,18,20,22 Across this group, patients had lost a mean of 48.3 kg in weight and 17.5 kg/m2 in body–mass index following surgery. This represents 79.4% of excess weight lost on average.
Presentation
All 13 patients presented with abdominal pain as their main symptom. Of these, 85% also experienced vomiting, with the remainder complaining of nausea. In two patients, hematemesis was a presenting feature.17,20 The duration of symptoms varied from hours to >1 week, with one patient having previous similar admissions intermittently throughout her pregnancy. 20 Examination findings were most commonly of vague upper abdominal tenderness, without peritonism, and minimal distension. In one case, a palpable mass was noted in the left upper quadrant. 21
Diagnosis
Results of blood tests were inconsistently contained within the published literature. In those where this information was available, 40% were noted to have no derangement of blood markers,3,16 while two patients had leukocytosis.17,19 One case noted elevated C-reactive protein and plasma lipase, leading to initial misdiagnosis of acute pancreatitis. 22 Ultrasound was used as the first-line investigation in six cases, but yielded the correct diagnosis in only one patient. 17 Three of these patients went on to have subsequent MRI scans and one had an additional CT scan. All of these confirmed intussusception.16,20,22,23 Three patients went straight to CT scan, all cases leading to the correct diagnosis.14,15,19 The remaining five patients were diagnosed intraoperatively.3,18,20,21
Treatment
Laparoscopic reduction of the intussusception was performed in three patients,3,15,18 but one had evidence of ischemia and perforation at the intussusception point requiring resection. 18 One patient had adhesionolysis, suturing of the bilio-pancreatic and common limbs, and resection of the jejunal remnant, thought to be a lead point of the intussusception, alongside this. 3 Attempt at laparoscopic resection was unsuccessful in one case and the patient went on to require laparotomy and resection of the affected segment of bowel. 14
Open reduction through a minilaparotomy was successful in one case, 23 while the remaining open cases required small bowel resection.16,17,19,20,22 Before surgery, one patient gave birth following induced labor, 19 while another had an urgent cesarean section before laparotomy. 17 In one case of a twin pregnancy, one baby died following delivery 7 days postop from subsequent necrotizing enterocolitis. 20
Discussion
RYGB is a frequently performed procedure in the treatment of morbid obesity. Obstructive small bowel obstruction is a recognized postoperative complication with an incidence of up to 4.5%. 14 Intussusception is far rarer and is responsible for only a very small proportion of these cases. Previous works have also noted that this almost exclusively occurs in females and is particularly associated with those who have undergone particularly rapid weight loss. 24 Pregnant patients represent an important subgroup within the limited existing literature, but one that requires important consideration. It is not uncommon for pregnant patients to present with nausea and vomiting, abdominal pain, or sensation of increasing abdominal distension. A high index of clinical suspicion is often required to stay vigilant to this as a differential diagnosis.
RYGB results in significant improvement in fertility of young obese females with improved regulation of menstrual cycle and reversal of comorbidity. As a result of this, SBO secondary to intussusception in the pregnant or postpartum patient is a recognized complication, but one which can be difficult to diagnose due to overlapping symptomatology of nausea, hyperemesis, and vague abdominal pain and the contraindication of CT scanning. In our study, the median time for developing intussusception was X weeks pregnant, suggesting (in keeping with previous studies) that the majority of cases occur in late pregnancy and in the third trimester, perhaps, we postulate, due to the gravidity of the uterus displacing the small bowel and rendering it more susceptible to invagination.22–23
In our study, the average time between RYGB and the appearance of symptoms in the nonpregnant population is variable, generally between 1 and 3 years after surgery. All intussusceptions were retrograde. Previous studies have shown that females were more likely to develop intussusception post-RYGB than males. The majority of patients were also young and in previous studies had a median age of 35.5 years, 20 and there is a suggestion that excessive weight loss may cause thinning of the mesentery and thus the bowel may be less resistant to invagination and thus more prone to intussusception. The etiology for developing intussusception after gastric bypass is probably multifactorial.
A widely accepted view in the literature, 21 which has been replicated in rat models, is the belief that the Roux limb disrupts natural pacemaker cells of the duodenum and allows for ectopic pacemaker cell formation in alimentary and bilio-pancreatic limbs, creating dysmotility and aberrant peristalsis, thus predisposing to intussusception. It could well be that a combination of aberrant or ectopic pacemaker activity with resultant dysmotility segments as well as a thin mesentery could result in intussusception. It is difficult to explain, however, how pregnancy could be a risk factor in this etiological process. The gravid uterus could displace the small bowel, affecting its position and motility. There has also been a long-held view of the suture line being a lead point causing intussusception, but it is difficult to see how pregnancy can relate to this.
The majority of patients presented with vague abdominal symptomatology, including diffuse abdominal pain, nausea, and vomiting. Since both physical examination and initial laboratory investigations were nonspecific and did not relay the appropriate information on the severity of the underlying pathology to surgeons, we argued that the onus of diagnosing intussusception was dependent on further radiological investigations. We found that CT scan or diagnostic laparoscopy/laparotomy was the diagnostic study of choice in majority of patients studied. However, in deciding how to operate, there is room for discussion. Some authors have suggested that simple reduction without resection is safe, while others have opted to proceed with resection of the bowel to prevent reoccurrence. We found in our research that the majority of patients required small bowel resection and revision of the anastomosis.
Complications associated with RYGB are notoriously difficult to diagnose and can be a potential pitfall especially in the pregnant and postpartum patient. It is important that all patients post bariatric surgery are thought to have low index of suspicion when presenting with vague abdominal symptoms for small bowel obstruction. The importance of anatomy-altering surgery such as RYGB in development of pre- and postpartum complications should be recognized by obstetricians and midwives, as well as general surgeons. Contraceptive advice and counseling should also be provided.
From the existing literature, it is not yet well established whether pregnancy represents an independent risk factor for development of post-RYGB intussusception. Further cohort and prospective studies on risk factors associated with development of intussusception would be useful to better manage pregnant women post bariatric surgery from a surgical and obstetric perspective.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.