
Abstract
Background:
We estimated the surgical effects of laparoscopic adjustable gastric banding (LAGB) in a sample of primary band patients in comparison to patients who needed band replacement due to band malfunction.
Methods:
An historical cohort study, composed of patients who underwent LAGB in surgery ward A, Soroka University Medical Center, which compared primary to revisional band patients. We used a set of questionnaires, including demographics data, health condition, and a quality-of-life evaluation (Bariatric Analysis and Reporting Outcome System [BAROS]).
Results:
Our study included 343 patients, of whom 97 were revisional surgery to replace the band due to mechanical reasons and 217 had a primary band operation. There was no significant difference between the groups regarding demographics or weight, apart from gender. The total BAROS score was significantly different between the groups, significantly better for good/excellent results among the band replacements.
Conclusions:
Our results have shown that band replacement has a similar complication rate to primary surgery. The results of band replacement are very similar to primary band surgery and even show a larger reduction in excess weight over time. We believe that LAGB contributes to the improvement of comorbidities in patients who have undergone band replacement, at least as in the general population.
Introduction
Obesity is considered a chronic disease that is increasingly common in adults, adolescents, and children and is now considered a global epidemic. Studies show that health expenditure is significantly higher for people who are overweight and obese.1,2 The risk of hypertension and diabetes increases with increased body mass index (BMI) (adjusted odds ratios [ORs] 2.6–4.8 for hypertension and 1.6–5.1 for diabetes) in people with normal BMI. Surgery is the only proven long-lasting treatment for obesity and its associated comorbidities. Several studies have shown that bariatric surgery is effective in reducing underlying obesity-related diseases, while there are other benefits such as reducing monthly drug costs and several sick days, and improving quality of life. 3 One of the surgical treatments for obesity is the use of an adjustable band or laparoscopic adjustable gastric band (LAGB). This procedure is purely restrictive, is technically simple, and has a low life-threatening complication rate. It allows for changes in the amount of restriction according to the patient's request. 4 The process is reversible and requires continuous knowledge and education by the physician/surgeon of the patient for effective weight loss, reduction and avoidance of weight gain, quality of life at the time the patient eats, and avoidance of complications associated with vomiting of food and drink. 4 Over the years, the band has undergone a number of modifications in its structure and strength, done by the manufacturers to provide a safer and more comfortable band placement during the operation, better band resistance for repeated fluid injections, and better durability over time.
At the Soroka Medical Center, we have seen a number of mechanical problems in the band that required intervention and were in direct proportion to the number of patients and the time that elapsed from the surgery, some of which were nonoperative, including a change in lifestyle, a change in fluid volume within the band, and some necessitated surgical intervention for removal and/or replacement of the band. We believe that the issue of LAGB's mechanical durability over time has not been adequately studied, including problems related to the band itself and whether this is a risk factor for surgical failure.
Thus, the aim of the current study was to review the various mechanical problems of the band that necessitated surgical replacement of the band, while comparing the surgical outcome of patients undergoing this intervention with patients who did not undergo such intervention. We must admit that this leaves other reasons for band replacement/removal not attended in the current study, such as patient intolerance (which was assessed in a previous article of ours 5 ), erosion, or band infection (these reasons are now being investigated by our research team).
The mechanical problems included the following:
Leakage of fluid from the band (both from the balloon and from the connecting tube) Tear in the band's locking mechanism Disconnection of the tube from the port.
In each of these problems, it is possible to identify signs and symptoms during the follow-up period, for example, patient complains that the restriction on eating ability has suddenly disappeared, the appearance of a constant increase in weight that cannot be reversed by reopening the band.
Materials and Methods
Study design
This is a retrospective cohort study performed in Soroka University Medical Center (SUMC), Beer-Sheva, Israel, approved by the local Institutional Review Board (IRB) (0100-11-SOR). Inclusion criteria were as follows: (1) patients who underwent LAGB (ICD-9 code 44.95) in the Department of Surgery A, SUMC, during the period 1/1996–12/2012. (2) Participants satisfied the accepted indications for bariatric surgery, including BMI >40 or BMI >35 with obesity-related comorbidities.2,6,7 (3) The patient had to remove the band due to a medical indication and underwent surgery to remove the band at Surgical Department A. (4) Patients who can consciously agree to participate in the trial.
Exclusion criteria were as follows: (1) patients who were unreachable by telephone or did not consent to participate. (2) Patients being followed-up by a few surgeons. (3) Patients suffering from severe and terminal illnesses (advanced malignancy, etc.).
The LAGB procedure was done by experienced surgeons in the accepted manner. 2 Type of band used was Swedish low-pressure/high-volume band (Swedish LAGB).
Data collection
Following approval from the local IRB Committee, the data were collected from a computerized database, including demographic data, preoperative BMI, short- and long-term complications due to surgery, and (if needed) repeated surgeries. In addition, there was a long-term evaluation of a follow-up period of at least 2 years that was conducted by telephone questioning. Long-term data were collected via a structured telephone interview that included minimum and current weight, current comorbidities, smoking status, physical activity, complications and reoperations, the Bariatric Analysis and Reporting Outcome System (BAROS) questionnaire, quality of life, and patient satisfaction.
Surgical outcome as reflected by weight loss, change in comorbidities, quality of life, and complication rate was assessed per the BAROS questionnaire, which is a standardized questionnaire for assessing weight loss and quality of life.8,9 Quality of life for BAROS scoring was evaluated using the Moorehead-Ardelt Quality of Life Questionnaire (Supplementary Fig. S1), with additional questions regarding approach toward food from the Moorehead-Ardelt Quality of Life Questionnaire II. 10 Another questionnaire designed for evaluating patients' overall satisfaction from the procedure and its consequences was also used (Supplementary Data). The data were coded into an anonymous database and stored in accordance with the local IRB protocol.
We divided the patients in two groups: The study group (revision group) consisted of all patients who underwent a band replacement due to medically indicated reasons. The control group consisted of a randomized sample of patients aged 18–65 years selected using the SPSS random assignment function.
Statistical analysis
Data analysis was performed using SPSS 23.0 (SPSS, Chicago, IL) software. We used the following descriptive and analytical statistics: independent samples t-test, one-way analysis of variance (ANOVA), and Scheffe comparisons. The comparison of groups was conducted using Pearson's chi-squared test for categorical variables and Fisher's exact test for dichotomous variables when applicable. Comparison of quantitative variables was done using parametric (t-test) and a-parametric tests (Mann–Whitney test). Differences were considered statistically significant at p < 0.05.
Statistical power
Statistical power was calculated by the comparative function in Winpepi software; 343 subjects were recruited for the current study, of whom 97 were in the study group (i.e., those who underwent a medically indicated band replacement), using the database in Surgical Department A to randomize subjects during these periods, With OR = 3, with an estimated complication rate of 0.1, the power of the study was 87% without continuity correction or 83% after continuity correction.
Results
The study involved 343 subjects, with 271/343 of the participants being women (79%), and 300/343 of the participants were born in Israel (88%). A total of 55 patients (16.2%) had a band slippage, and 126/343 (36.6%) needed further surgery after the band placement.
Of those who needed another surgery after the primary band, 18 (14.3%) had suffered from band slippage, 57 needed band replacement (45.2%), 29 had their band removed (23%), 18 had their band removed and a new one inserted at a later date (14.3%), and 4 had their band removed and had another bariatric procedure (3.2%). When looking at patients who removed their band (due to any reason), we have seen that 19 (27.1%) removed their band due to slippage, 11 due to band malfunction, 5 due to prolonged abdominal pain (7.1%), 10 due to band intolerance (14.3%), and 25 due to other reasons (37.5%). The band was replaced in 97/344 of the patients in the study period (28.2%), and the reasons for this were—34 (35.1%) due to band slippage, 13 (13.4%) due to a tear of the band, 36 (37.1%) due to band leakage, and 14 (14.4%) due to other reasons. This is depicted in Figure 1.
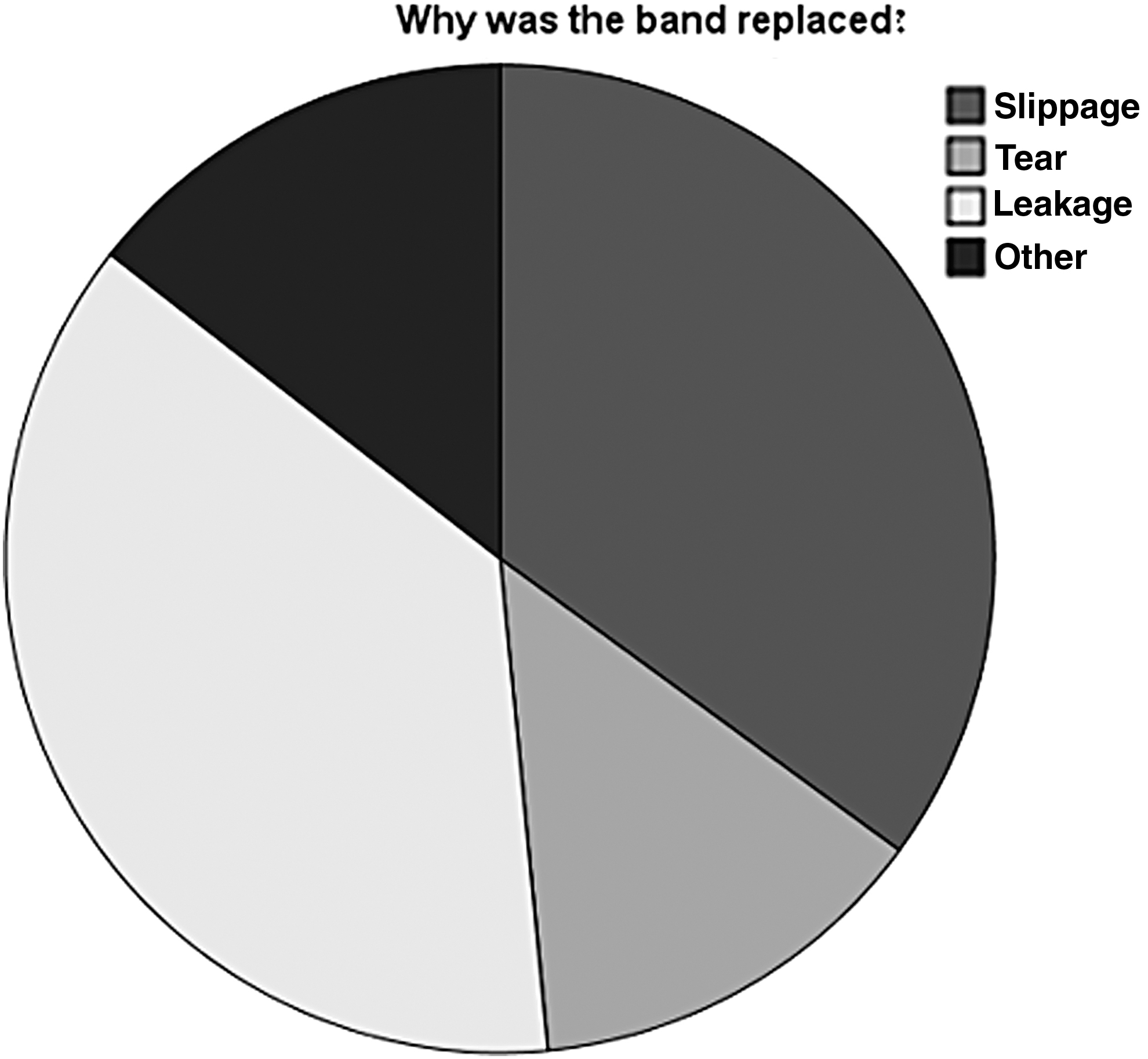
Band replacement reasons.
We divided our subjects to two main groups—those who had their band replaced due to maintenance issues (also called the cases) and the general population who had laparoscopic gastric banding (LGB) performed as their primary operation (also called control group).
Table 1 depicts the basic demographic data of the cases versus the control group, and as shown, there were no significant differences between the groups.
Demographic Data of the Band Replacement Group Versus the Control Group
Table 2 shows the comparison of the anthropometric data between the groups, and as shown, all variables are similar except for the minimum weight attained and all its derivates (e.g., lowest BMI attained), which was in favor for those who had replaced their band (p < 0.001).
Anthropometric Data of the Subjects
BMI, body mass index; EBW, excess body weight; IBW, ideal body weight.
Table 3 is the comparison of comorbidities in patients who had their band replaced due to maintenance issues, in comparison to the general population. No differences were found between the case and control groups, except for the difference in the previous surgery rate, which was higher in the cases, and in bone density diseases where the rate was higher in the cases group.
Comorbidities Before LGB Demographics
CPAP, continuous positive airway pressure; DM II, diabetes melitus type 2; GERD, gastroesophageal reflux disease; HTN, hypertension; LGB, lap gastric band; OSA, obstructive sleep apnea; s.c., sub cutaneous.
Table 4 depicts the postoperative results, and as seen, there were no differences between groups except the time of effective usage of the band, which was longer in those who replaced the band due to maintenance issues.
Postoperative Data
The BAROS questionnaire has five subsets that account for excess weight loss, medical improvement after surgery, quality of life, complication, need for a reoperation, and a total score. The quality-of-life subset had no significant differences between the groups.
Similar results were seen in the medical improvement subset (which was similar for all comorbidities except for diabetes, which was slightly better controlled in the band removals for maintenance, p = 0.027).
When talking about postoperative complications, the short-term complications are presented in Table 5, with no significant differences between the groups.
Early Postoperative Complications
When looking at long-term complications, there was a significant difference between the groups (p < 0.001), which is not surprising because band replacement necessitates reoperation, which is considered a complication. Thus, we did a subgroup analysis looking only at patients who had another operation, as depicted in Table 6.
Late Postoperative Complications, Indication for Reoperation
When looking at the excess weight loss subset of the BAROS, there was no difference between the groups (p = 0.441).
Table 7 depicts the total BAROS score, and as can be seen, there was a significant difference between the groups, in favor of the control group (p < 0.001). While the rate of failure is higher among the cases group, the rate of patients with a fair score and higher was higher among the cases group.
A Comparison of BAROS Total Scores
BAROS, Bariatric Analysis and Reporting Outcome System.
We also asked our patients if they are satisfied with the band, and whether it fulfilled their expectations in the long term and found no significant difference between the groups (p = 0.274 and p = 0.339, respectively).
Discussion
Our study examined LAGB subjects who removed the band due to medical indications (i.e., band tear, leakage, or slippage) and compared them to band patients who, during the study, did not remove it or replace it due to a defect that required replacement. Our study included 343 patients, of whom 97 were in the cases group (recurrent surgery to replace the band due to medical indication) and 217 in the control group (only one surgery was performed).
The success of the LAGB was assessed by several measures: weight loss and excess weight loss over time, influence on the prevalence and severity of obesity and metabolic syndrome, the prevalence of early complications and later known complications associated with surgery, and subjective satisfaction of the patients.
Finally, an evaluation was made for the success of the operation using the BAROS questionnaire, which is the accepted one in the field of bariatric surgery. For each of the parameters, the effect was assessed on patients who underwent resurgery or replaced the band compared with those who underwent surgery only once.
Examination of the baseline variables showed that there was no significant difference between the groups, apart from gender; it was found that there were more women who replaced the band. In examining anthropometric data, no difference was found in most of the variables, except for the minimum weight and its derivatives (minimum BMI and excess weight loss [EWL] to a minimum weight). Another significant difference found between the groups was the total time with the band: it was 4.8 years without replacing versus 8.1 years on average among band replacements. Comparing baseline comorbidities, no difference was found between band replacements and primary operation patients, except for previous surgeries (once again in the case of a replacement patient, it is not surprising) and osteopenia.
The total BAROS score was significantly different between the groups, with the median value being significantly lower among the band replacements. When looking at the different subsets of BAROS, we can see that weight loss according to BAROS did not show any difference between the groups, and in postoperative outcomes from a health perspective, there was no difference between the groups except diabetes.
Examination of the complications showed that there was no difference between the groups in early complications and the chance of band removal. But there was a difference in the rate of later complications; it is important to remember that changing a band for any reason is considered a late complication, so it is not surprising that the rate is higher in this group. The nature of reoperations was different in the compared groups. In the cases group, most of the reoperations were for replacement of the band due to medically indicated reasons (over two-thirds of the cases). In most control patients, the reasons were removal (not medically indicated) and other bariatric surgery (over 80% of cases). In terms of the subjective evaluation of the subjects, there was no significant difference between the groups in any variable, that is, the operation was perceived by them in a similar manner.
So, if we summarize our results—there was no real difference between revisional band patients who had their band replaced and primary band patients, when looking at both objective and subjective measures. The question is whether our results are in accordance with what the research in the area has shown us? Arapis et al. 11 monitored 18 years of band patients and found that the rate of early complications was very low, whereas the later complications were more than 50%.
Our study had similar short-term complications, but long-term complications were lower. This could be due to the fact that the duration of our patients' follow-up was shorter than that of Arapis et al., but the fact that the trends are similar is encouraging. Arapis et al. found that about 42% of the bands were removed due to intolerance, weight gain, or other complications (mainly band slippage). In our study, a much lower rate (23%) was seen and this could have been due to the shorter follow-up time.
However, there may also be a more prosaic reason—the nature of follow-up. Arapis et al. reported fewer than 1000 subjects included in the study, with follow-up as needed.
In our clinics, there is a long-term follow-up of LAGB patients for a decade or more, with close follow-up and more than 10,000 patients, which means that it may not have been the follow-up time per se, but due to the nature of how that follow-up was conducted.
On the contrary, Arapis' patients had an EWL reduction of 41% even 15 years after the original surgery. In our study, EWL was higher (>50% in both groups) than could be explained by the longer follow-up in Arapis, or, as noted earlier, in the quality of follow-up and its frequency is significantly higher among our patients.
Arapis et al. argued that despite a high initial success rate, given the high complication rate, the LAGB is not a problem-free operation. On the contrary, the reversibility of the operation and the minor complications make it relatively efficient and safe, especially for patients with high motivation and those who are able to have frequent follow-up. This sentence seems to sum up our understanding of the band patients, especially those who have undergone band replacement—they are patients who need more frequent follow-up, as well as a balance that is slightly more difficult due to expectations and habits created by using the old band. An addition that aids us in the understanding of the complexity of LAGB patients and management comes from Lazzati and his colleagues, 12 who examined more than 50,000 patients and found a removal rate of 40% similar to that of Arapis et al. 11
They found that women and patients with more severe obesity tended to remove the band. Lazzati and his colleagues talked about a removal rate of 5–6% of the patients per year, and that the rate of those requiring conversion surgery (whether removal and other bariatric surgery or band replacement) was 70%, and therefore concluded that the band is not a long-term procedure.
It seems that despite a similar study design, our conclusion is significantly different—because it involves a similar follow-up time, and a surprisingly different rate of complications, it seems that the initial claim that the frequency and quality of follow-up of band patients is the main issue. Once a patient with a band has difficulty using it and undergoes another bariatric surgery, instead of trying to train and preserve the band, it is clear that the removal rate will be significantly higher, followed by the conclusion that this is not a long-lasting solution. However, our data show that if there is effective and frequent monitoring, as well as willingness to continue to use the band with this mechanical failure (band malfunction), the results are much better and there is the possibility that this treatment will succeed without the need to perform surgeries that are inherently more dangerous, certainly when the alternatives (such as sleeve or bypass) carry not only higher morbidity but also mortality. It seems that the bariatric surgeon's arsenal should have more than one type of surgery, and that an understanding of the effectiveness of the LAGB for the appropriate patient (especially with the right motivation to be monitored and titrated as needed) can produce far better results. Kodner and Hartman 13 reached a similar conclusion and they argue that the treatment of LAGB complications is not the immediate extraction of the band in any case, but that there is a regular and logical system of follow-up and treatment of the complications to achieve optimal results with the band. Similarly, Egan et al. 14 reviewed the literature on the subject of band complications, specifically slippage and band malfunction (e.g., rupture) and found considerable disagreement in the literature over the very definition of these complications, each surgeon can define the complications and therefore the treatment.
This lack of uniformity seems to lead to an inability to come to a conclusion about the correct treatment of band dysfunction and explain the significant difference between the results of our study and the results of Lazzati and his colleagues, where the rate of complications and removal of the band was almost double. In this respect, the study from O'Brien et al. 15 examined more than 3000 subjects for more than a decade. As in our study, there was no known operative mortality, for both the primary and the revisional surgery. At the end of the study, EWL% was similar to that seen in our study (47%), regardless of whether the patient was operated on once or required surgical revision, similar to the findings that were found in our study.
Our study added to the fact that we examined the surgical outcome at the subjective level using a BAROS questionnaire and showed that patients requiring revisional band surgery were at increased risk of a poorer surgical outcome, highlighting the importance of frequent, continuous, and high-quality follow-up.
As with any study, the current study has a few limitations. First, the sample of patients was not ideal. The revision group was smaller in size (accounting for only 33% of patients in the study). Another flaw of this study is that the control group was characterized by a shorter follow-up and this might have influenced the results of comparison between groups.
Conclusions
Our study has shown that LAGB allows for a good weight loss, and that it is a means of success for long-term weight loss, that has a low incidence of immediate complications, even among patients requiring a revisional operation.
Our results have shown that band replacement has a similar complication rate to primary surgery, which is considered lower than other bariatric procedures. We have found that the results of band replacement are very similar to primary band surgery and even show a larger reduction in excess weight over time, but there is room for closer monitoring because after band replacement some patients might suffer from a higher pattern of failure. We feel that our study added in that we examined the surgical outcome at the subjective level using the BAROS questionnaire, and have seen that patients requiring band replacement surgery were at increased risk of poor surgical outcome, highlighting the importance of frequent, continuous, and high-quality follow-up.
We believe that LAGB contributes to the improvement of comorbidities due to a substantial weight loss in patients who have undergone band replacement, at least as in the general population. In light of the health benefits of long-term weight loss, which are reflected in a decrease in morbidity compared to the low complication rate of band replacement and a higher percentage of complications in other bariatric surgery, we believe that band replacement surgery plays a major role in maintaining long-term weight loss in morbidly obese patients who opt for this procedure.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.