
Abstract
Objective:
The aim of the study was to evaluate hormone level, nutrition status, and energy expenditure of patients with laparoscopic sleeve gastrectomy (LSG).
Materials and Methods:
Twenty female patients, who underwent a LSG operation, were subjected to testing. The body analysis and biochemical parameters of these patients were determined before and after the surgery. The patients' appetite status and food consumption were monitored during the follow-up.
Results:
The percentage of fat in the body, weight, and body mass index (BMI) of the patients decreased (p < 0.05). Physical activity level and total energy expenditure (TEE) increased in the postoperative period (p < 0.05). The patients' appetite score decreased in the first postoperative month (p < 0.05). Total values of energy, carbohydrate, and fat consumption of patients decreased (p < 0.05). Fasting blood glucose and triglyceride level decreased in the follow-up period (p < 0.05). In the postoperative period, the levels of thyroid stimulating hormone (TSH) and ghrelin hormone decreased compared to the preoperative period (p < 0.05). There was no correlation between the change in ghrelin hormone and TSH level among the follow-ups and body weight, BMI, and weight loss (p > 0.05).
Conclusion:
While there is no clear correlation of weight loss to TSH and ghrelin expressions, hormonal changes and TEE remain very dynamic in the early months after surgery. This study prospectively characterizes such changes.
Introduction
Obesity is one of the most important public health problems of developed and developing countries, is observed in all age groups, and has severe negative effects on the mortality and morbidity rates. A body mass index (BMI) of >40 kg/m2 is described as morbid obesity, which affects quality of life in individuals negatively, shortens life expectancy, and takes the place near the top among preventable causes of death especially in developed countries. 1 In recent years, due to an increase in morbid obesity prevalence, in the level of awareness of society about obesity, and improvement in surgical procedures, an increase has been observed in the prevalence of the request for bariatric surgical methods. The aim of applying the bariatric surgery, which is an effective treatment method for morbid obesity, is to provide weight loss for patients and increase their life qualities. 2
As laparoscopic sleeve gastrectomy (LSG) surgery procedures included in the restrictive methods are easier and have more satisfying early period results, they have started to become a safe and effective method and have seen an increase in application frequency. In this method, weight loss observed after surgical intervention is associated with restrictions in food intake and changes in energy expenditure and hormone levels. 3 It has been stated that changes in the ghrelin hormone, which is mainly secreted from the stomach fundus and plays an important role in the regulation of food intake, are effective in changes of appetite and weight loss after LSG. 4 While it is expected that the ghrelin hormone decreases due to the stomach fundus excision after LSG, the results of the studies conducted on this subject are different.5–7 In addition, it has been reported that LSG operations affect thyroid hormone kinetics. 8 In previous studies, it has been reported that thyroid stimulating hormone (TSH) levels decrease after LSG. However, no correlation has been found between this decrease and weight loss.8,9
Concerning energy expedition, it has been reported that there is a decrease in the total and resting energy expenditure and an increase in the energy expended with physical activity after bariatric surgery. 10 However, there is also study indicating that physical activity level (PAL) does not change after surgical intervention. 11 In addition, it has been reported that the appetite and taste of the individuals also change after bariatric surgeries and it is predicted that the food intake of the individuals decreases together with the decreasing appetite. 12
This study was designed and conducted to assess the energy expenditure, hormone levels, and changes in the nutrition status after LSG. No study was found in the literature assessing the mentioned parameters together.
Materials and Methods
This prospective analytic study was conducted with 20 female patients who underwent LSG in Kayseri Erciyes University Medical Faculty Hospitals. Individuals who were aged between 18 and 65 years, had BMI of ≥40 kg/m2 and/or BMI of ≥35 kg/m2, and comorbid disease were included in the study. The patients who would not be able to come for after the surgical intervention checkups as they resided in another location were excluded from the study. Before the study, permission from Erciyes University Medical Faculty hospitals, as well as ethics committee approval (dated 18.03.2016 and decision no 2016/192), were obtained. In addition, all the participants were informed about the study and then their written and verbal consents were obtained. Twenty three patients who underwent LSG between November 2016 and April 2017 were included. During the study, three patients did not come for checkups and they were excluded from the study. In the statistical analysis done at the end of the study, the sample power of the research was found to be 99%.
The information on the demographic and health status of the individuals was obtained using a questionnaire. The body analysis of the individuals was performed using a TANITA BC 418 device; the waist, hip, and neck circumferences were measured by the researcher in accordance with the method. The Mifflin–St Jeor equation was used in calculating the metabolism rate of obese people in the estimation of resting metabolism rate, and the PALs were determined using a 24-h physical activity record. The biochemical data of the patients were recorded retrospectively from the patient files. “The Simplified Nutritional Appetite Questionnaire (SNAQ)” was used in determining the appetite score of the individuals, and the 3-day food consumption records were obtained to assess the food consumption of the patients. The types and amounts of the daily consumed food were determined based on the food consumption record and values of energy; macro and micro nutritional elements were calculated using the Nutrition Information Systems (BeBiS) program prepared for Turkish nutrition. To determine the plasma total ghrelin levels of the patients, blood samples were drawn into ethylenediaminetetraacetic acid (EDTA) tubes. To prevent ghrelin breakdown in the blood samples, 1 mg/mL of Pefabloc® SC, a protease inhibitor, was added. The blood samples were centrifuged at 2000–3000 × g for 15 min at +4°C, and the plasma was separated and put into 1 mg Eppendorf tubes. Four microgram HCl was added into the tubes in accordance with the kit procedure used for ghrelin analysis. The samples were put into deep freeze (−20°C) to keep until the analysis day. Ghrelin analysis was performed with immune-enzymatic (ELISA) method using a commercial ELISA Kit. For plasma ghrelin analysis in accordance with the ELISA method, “Cusabio Human Ghrelin (GHRL) ELISA Kit CSB-E13398h kit” was used. The individuals were called for checkup again in the first, second, and third month after surgical intervention. In the follow-up meetings, complications after surgery were evaluated in addition to procedures performed before surgery, and the nutrition supports used after surgery were examined.
The data obtained in the study were analyzed using SPSS (Statistical Package for Social Sciences) for Windows 25.0. The frequency and percentage values for the data obtained from the patients were interpreted and evaluated using mean and standard deviation. The suitability of the data with the normal distribution was tested with Shapiro–Wilk test. The difference between the mean values of the qualitative variables was analyzed according to analysis of variance (ANOVA) statistics for repeated measures. The change of the postoperative complications of the patients based on follow-up times was analyzed according to Cochran's Q test. The correlation between the variables was analyzed by correlation analysis. In all the tests, the value of p < 0.05 was accepted as statistically significant.
Results
This study was conducted with 20 women undergoing LSG, and the average age of the patients was 57.00 ± 40.15 (min–max = 18–57 years). In the postoperative follow-ups of the patients, a significant decrease was determined in body weight, BMI, body fat percentage and amount, body fat-free tissue mass, total body water, waist, hip, and neck circumference measurements (p < 0.05) (Table 1).
Evaluation of Anthropometric Measurements and Body Composition of Patients
 ± SS
± SSDifferent letters indicate differences between groups.
p < 0.05.
BMI, body mass index; preop, preoperation; postop, postoperation.
While the resting metabolism rate (RMR) of the patients decreased during the follow-up, the PAL and total energy expenditure (TEE) increased (p < 0.05). It was determined that the patients spent more time for walking in the postoperative period (p < 0.05) (Table 2).
Evaluation of Resting Metabolic Rate, Physical Activity Level, Physical Activity Duration, and Total Energy Expenditure of Patients
Different letters indicate differences between groups.
p < 0.05.
Table 3 shows the mean values of biochemical findings of the patients in the four follow-ups. The fasting glucose (FG) of the patients decreased significantly during the follow-up, and this decrease was correlated with the weight loss percentage (r = −0.472; p < 0.05). In addition, it was observed that while serum triglyceride, aspartate aminotransferase, and alanine aminotransferase levels decreased, serum albumin, vitamin B12, magnesium (Mg), potassium (K), calcium (Ca), and phosphorus (P) levels increased (p < 0.05) (Table 3). The serum TSH level of the patients decreased in the first and second months after surgery (p < 0.05), and an increase was observed in the third month after surgery compared to the second month but this difference was not significant (p > 0.05) (Fig. 1). The plasma ghrelin levels of the patients decreased during the follow-up, and the difference between mean values of the four follow-ups was found to be significant (p < 0.05). The plasma ghrelin level was 1123.66 ± 660.01 pg/mL in the period before surgery, and it was measured as 259.93 ± 96.27 pg/mL with a decrease of 77% in the third month after surgery (Fig. 2). In the present study, a negative significant correlation was determined between the plasma ghrelin levels and total protein and animal protein intake with diet (r = −0.569; p < 0.05).

Changes in serum TSH levels of patients during follow-up. There was a 31.8% decrease in serum TSH level in the first postoperative month. In the second postoperative month, serum TSH level decreased by 4.9%. In the third postoperative month, serum TSH levels increased by 1.49%. At the end of the third month after surgery, serum TSH level decreased by 34.2%. TSH, thyroid stimulating hormone.

Changes in plasma ghrelin levels of patients during follow-up. There was a 51.3% decrease in plasma ghrelin level in the first postoperative month. Plasma ghrelin level decreased by 30% in the second month after surgery and decreased by 32% in the third month after surgery. There was 77% decrease in plasma ghrelin levels during the follow-up.
Evaluation of Biochemical Parameters of Patients
Different letters indicate differences between groups.
p < 0.05.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TSH, thyroid stimulating hormone.
While the appetite score of the patients decreased in the first month after surgery (p < 0.05), the increase observed after the first month was not found to be significant (p > 0.05) (Fig. 3). It was determined that total energy, carbohydrate, and dietary fiber intake of the patients through diet decreased in the period after surgery. While protein and fat intake through diet decreased in the period after surgery, the rates of the energy coming from protein and fat increased (p < 0.05). In the micronutrition intake, it was determined that vitamin E, thiamine, riboflavin, niacin, folic acid, and vitamin B6 intake through diet and Na, K, Mg, P, and Zn intakes decreased in the postoperative period compared to the preoperative period (p < 0.05) (Table 4).
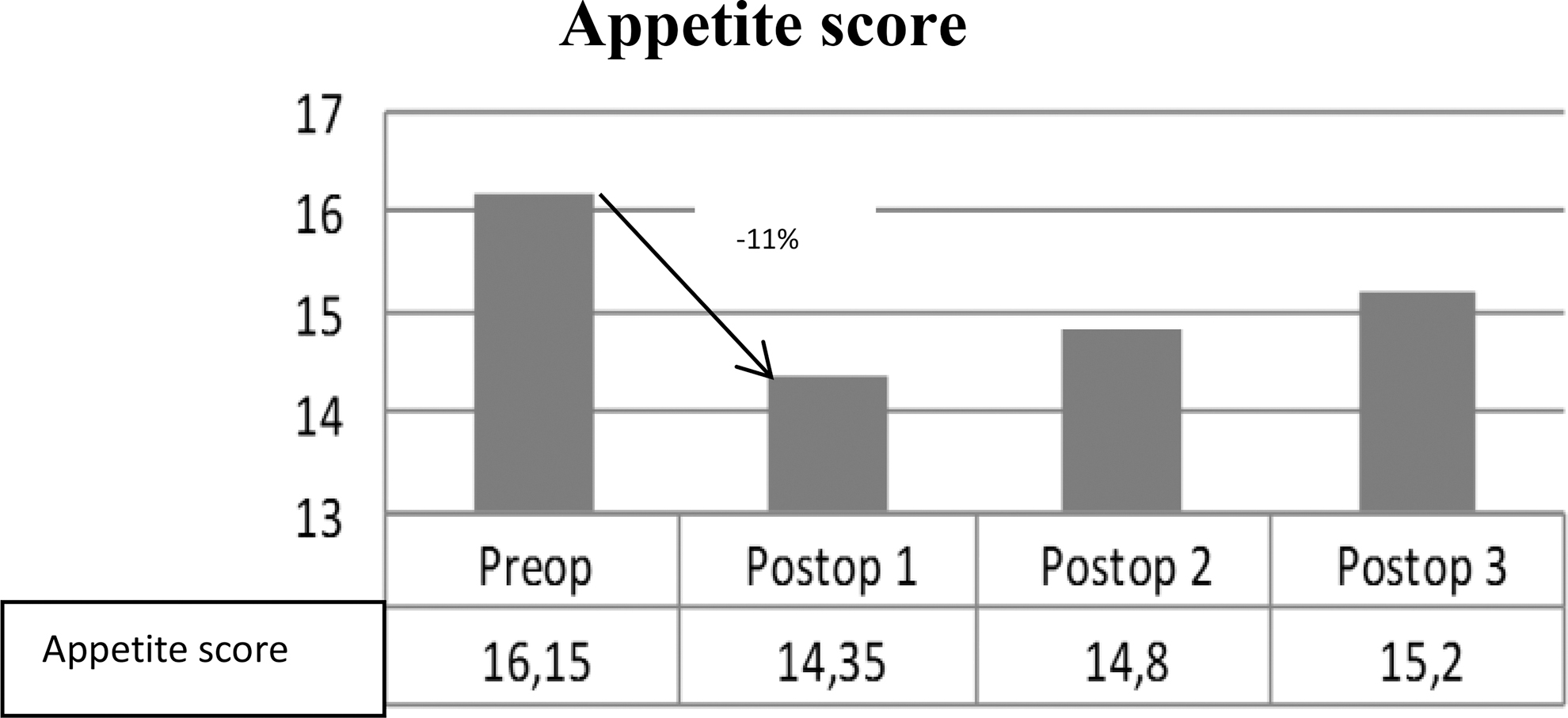
Changes in the appetite scores of patients during follow-up. There was a 11% decrease in the appetite scores in the first postoperative month.
Evaluation of the Intake of Energy, Macro, and Micro Nutrients of Patients' Diet
Different letters indicate differences between groups.
p < 0.05.
When the complications experienced by the patients after surgery were examined, 30% of the patients had the complaint of nausea, 10% had the complaint of vomiting, 15% had the complaint of diarrhea, and 70% had the complaint of constipation in the first month after surgery. Seventy five percent of the patients stated that they had fatigue and weakness in the postoperative first month. The fatigue and weakness complaint decreased in the postoperative second (30%) and postoperative third month (30%) compared to the preoperative first month (75%) (p < 0.05). While hair loss increased in the postoperative third month compared to the postoperative first and second months (p < 0.05), 70% of the patients stated that they had hair loss in the postoperative third month (Table 5).
Evaluation of Postoperative Complications
p < 0.05.
Discussion and Conclusion
Bariatric surgeries are suggested as the only and the most effective way providing weight loss in morbid obesity for the long term. 2 In the present study, the weight loss percentage was determined as 9.56 ± 2.41% in the postoperative first month and 17.63 ± 3.86% in the postoperative third month (p < 0.05). The patients lost 11 kg in average in the postoperative first month, and the change in the BMI values of the patients at the end of the third month was determined as 8 U (Table 1). In a previous study, it was reported that patients lost 13 kg in average in the postoperative first month. 13 In their study, Schneider et al., 14 determined that weight loss was 64% in the postoperative 17th month. It was observed that the results of the present study are parallel with the results conducted in similar follow-up periods. In studies in which the patients are followed for a longer period, it has been observed that the weight loss percentages increase due to increasing follow-up periods.13,14 Fat-free tissue mass loss may be observed after sleeve gastrectomy, and these results are associated with unwanted clinical results and mortality. 15 Similar to the study by Belfiore et al., 16 it was observed in the present study that there were decreases in the fat-free tissue mass measurements of the patients (p < 0.05). It has been emphasized that preserving fat-free tissue mass has great importance upon providing adequate weight loss in these patients, and the importance of the adequate protein intake and regular exercises for the sustainability of the fat-free tissue mass after surgery has been emphasized. 15
It has been reported that while the PAL of the patients after surgery increases, there is a decrease in the total energy expedition. It has been suggested that the resting energy expenditure decreases depending on the loss in the fat-free body mass. 10 In the present study, an increase was observed in the PAL values and TEE of the patients (p < 0.05) (Table 2). A related study demonstrated that there is an increase in the PAL after surgery. 17 However, there are also studies indicating that the PALs of the patients do not change after surgery.11,18 The studies have emphasized that increasing the PALs after surgery is important to provide the long-term weight loss and for improvement in clinical results.17,18 In the present study, the RMRs of the patients were determined using a Mifflin–St Jeor formula. In this context, the RMRs of the patients decreased together with their body weights. The indirect calorimeter method accepted as the golden standard in RMR measurement could not be used due to the inadequacy of the study budget.
It has been reported that recovery is provided in the metabolic parameters together with weight loss in patients after sleeve gastrectomy. 19 In this study, a decrease was determined in the FG as the weight loss percentage of the patients increased (r = −0.472; p < 0.05). In addition, a decrease was observed in the triglyceride measurements during the follow-up (p < 0.05) (Table 3). In several studies,19,20 positive changes have been reported in glycemic control and lipid profile after surgery. Despite the recovery in the metabolic parameters after surgery in these patients, several nutritional deficiencies such as vitamin D, folate, vitamin B12, Fe, Se, Zn, and Cu are frequently observed.21,22 In contrast to literature data,21,22 in this study, it was observed that there were increases in serum B12, Mg, K, Ca, and P levels after surgery (p < 0.05). In the present study, in the period after surgery, 85% of the patients stated that they used injectable vitamin B12 monthly, 10% of them stated that they used a vitamin B complex and mineral support, and 10% stated that they used vitamin D support (Data are not shown). It was thought that the increase of the serum vitamin and mineral levels in the patients after surgery was related to the vitamin and mineral supports they used.
It has been reported that the sleeve gastrectomy operations provided a decrease in serum TSH levels, and they had positive effects on hypothyroidism. 8 In the present study, it was determined that TSH levels decreased in the postoperative first and second months (Fig. 1), and no correlation was determined between this decrease and weight loss, similar to the studies6,9 in literature (r = 0.097, p = 0.684). The studies were conducted to assess the short- and long-term effects of LSG on the ghrelin levels, which have revealed that there were significant decreases in the ghrelin levels after LSG and this situation was associated with the protection of the gastric fundus.3,6 Also in this study, the plasma total ghrelin levels decreased during the follow-up (p < 0.05) (Fig. 2). A similar study reported that the change in the ghrelin levels was associated with appetite, food intake, and weight loss. 23 However, it was reported in another study that the decrease in ghrelin levels did not affect the clinical results of the patients and their anthropometric measurements for the 1-year follow-up. 7 In the present study, it was observed that while there was no correlation between ghrelin and weight loss, appetite score, total energy with diet, carbohydrate, and fat intake (p > 0.05), there was correlation only between ghrelin and the protein intake with diet (p < 0.05). It has been suggested that the weight loss of the patients accelerates together with the diet, including high protein. 24 In the present study, in accordance with this result, it was considered that ghrelin may be effective on the weight loss by providing an increase in the protein intake. In addition, the appetite and taste of the patients change after LSG, and there are decreases in food intake. 12 In the present study, the appetite score of the patients decreased in the postoperative first month compared to the preoperative period (p < 0.05, Fig. 3). The present study revealed decreases in the energy, macro, and micro nutritional elements with diet in the postoperative period (Table 4). The protein intake of the patients decreased in the postoperative period, but the protein energy percentage increased (p < 0.05). These data were similar to the study of Moizé et al. 25 The fact that the contribution of protein to energy is high shows that patients prefer a protein source, in food consumption. It is considered that this choice may be beneficial for the protection of the fat-free tissue mass.
It is known that the bariatric surgery procedures provide successful results in the treatment of the morbid obesity. It is required that these individuals are examined in terms of long-term complications of the surgery. 26 In the present study, similar to the studies in literature,26,27 the patients stated that they had various complications such as nausea/vomiting, reflux, diarrhea, constipation, and hair loss during the follow-up (Table 5). These results revealed the need to assess patients based on the complications observed after surgery and to take precautions related to these complications.
Consequently, positive changes were observed in the anthropometric measurements and biochemical parameters of the patients after LSG. The PAL values of the patients and, thus, the total energy expeditions increased. This demonstrated the need to motivate patients to perform physical activity in the postoperative period and support them in this issue. The decreases in plasma ghrelin and serum TSH level had no correlation with weight loss and food intake. It is considered that this situation may be affected by many factors and that studies with longer follow-up periods need to be conducted to understand this effect better.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Erciyes University Scientific Research Projects Unit with project code TDK-2016-6749.