
Abstract
Background:
Obesity is associated with lower life expectancy and many comorbid diseases, including arterial hypertension, hyperlipidemia, and type 2 diabetes mellitus (T2DM), which is defined as metabolic syndrome (MetS). The aim of this study was to investigate the effects of laparoscopic sleeve gastrectomy (LSG) on parameters of MetS in obese patients 2 years after surgery.
Methods:
Between March 2013 and June 2019 1333 patients, who underwent LSG, were enrolled in this study; patients fulfilling the following conditions were considered eligible for LSG: body mass index (BMI) ≥40 kg/m2 or BMI >35 kg/m2 with comorbidities or BMI between 30 and 35 kg/m2 with T2DM or MetS. The patients were followed up by outpatient visits that were scheduled at 1st, 3rd, 6th, and 12th months postoperatively and annually thereafter.
Results:
One thousand three hundred and thirty-three patients underwent LSG. The mean age was 40.93 ± 10.86; 954 (71.5%) patients were female. After 2 years of surgery there was a significant improvement in glucose, glycosylated hemoglobin (HbA1c), insulin, the homeostasis model assessment insulin resistance, triglycerides, and high-density lipoprotein cholesterol (p < 0.0001) with no significant reduction in serum total cholesterol (p = 0.392) and low-density lipoprotein cholesterol (p = 0.692) levels.
Conclusions:
LSG is an effective treatment for MetS and obesity related comorbidities.
Introduction
The incidence of obesity is increasing throughout the world. It is believed that more than 1 billion adults are obese or overweight. Obesity is associated with lower life expectancy and many comorbid diseases, including arterial hypertension, hyperlipidemia, and type 2 diabetes mellitus (T2DM), which is defined as metabolic syndrome (MetS).1–3 The prevalence rate of MetS is more than 50% in morbidly obese patients 4 and associated with an increased risk of many diseases such as cardiovascular disease (CVD) and stroke, as well as increased burden of health care costs.5–7 For diagnosis of MetS, at least three of the following criteria must be present: Abdominal obesity (>102 cm in men, >88 cm in women), a level of triglycerides (TG) more than 150 mg/dL, high-density lipoprotein (HDL) cholesterol levels (<40 mg/dL men, <50 mg/dL women), a high systolic or diastolic blood pressure more than 130 and 85 mmHg, respectively, and a raised fasting glucose level of ≥100 mg/dL. It has been suggested that weight loss can effectively improve MetS. There are several options for weight loss such as diet, increasing physical activity, and bariatric surgery (BS). However, nonsurgical methods may take longer time and may be insufficient in individuals with hormonal disorders or metabolic diseases.8,9
BS has been shown to be effective in achieving and maintaining weight loss and reducing the risk of obesity related comorbidities. 10 Laparoscopic sleeve gastrectomy (LSG) is frequently the first-choice surgery because it is associated with lower risk and it is an easy technique to carry out. LSG is not only a restrictive procedure but also changes gastrointestinal hormone levels such as serum ghrelin, peptide YY (PYY), and glucagon-like-peptide-1 (GLP-1).11,12 The aim of this study was to investigate the effects of LSG on parameters of MetS in obese patients 2 years after surgery.
Materials and Methods
This study was approved by the ethics review committee of our hospital. The need for informed consent was waived because of the retrospective nature of the study. The study was conducted according to the principles of the Declaration of Helsinki. The medical records of our Bariatric Center of Excellence were reviewed retrospectively to identify all consecutive patients with morbid obesity who underwent LSG between March 2013 and June 2019. All patients were considered fit for BS based on the guidelines of American Association for Clinical Endocrinologists, The Obesity Society, and the American Society for Metabolic and Bariatric Surgery. 13
Patients fulfilling the following conditions were considered eligible for LSG: BMI (body mass index) ≥40 kg/m2 or BMI >35 kg/m2 with comorbidities or BMI between 30 and 35 kg/m2 with T2DM or MetS. All patients were evaluated by a multidisciplinary team consisting of a cardiologist, an endocrinologist, a dietetic, a psychologist, and the pulmonologist before surgery. Medical imaging was also performed (chest X-ray, abdominal ultrasonography, and gastroscopy if it is necessary). Blood analysis was performed preoperatively. Demographic data, BMI, blood levels of insulin, TG, total cholesterol (TC), HDL, serum low-density lipoprotein (LDL) cholesterol, glycosylated hemoglobin (HbA1c), glucose, and the homeostasis model assessment insulin resistance (HOMA-IR) were recorded. Percentage of excess weight loss (EWL%) was also calculated. The ideal body weight was deemed equal to a BMI of 25.
The patients were followed up by outpatient visits that were scheduled at 1st, 3rd, 6th, and 12th months postoperatively and annually thereafter. The surgical technique has been reported in our article previously. 14
Complete remission for diabetes is defined as HbA1c <6 and glucose <100 mg/dL, and partial remission is defined as HbA1c value between 6 and 6.5 and glucose between 100 and 125 mg/dL without medication.
Complete remission for hypertension is defined as blood pressure <120/80 mmHg and no medication is used. Partial remission for hypertension is systolic blood pressure in the range of 120–140 mmHg and diastolic blood pressure in the range of 80–89 mmHg without medication.
Complete remission for hyperlipidemia is defined as TC <200 mg/dL, HDL >40 mg/dL, LDL <160 mg/dL, and TG <150 mg/dL without medication. A decrease in the number or dose of lipid lowering drugs with normal blood values is considered as partial remission.
Statistical analysis
The analysis was conducted using Statistical Package for the Social Sciences 22.0 (SPSS, Chicago, IL). The distribution of the variables was tested by Kolmogorov–Smirnov test. Continuous variables with a normal distribution were expressed as mean and standard deviation values. Variables with non-normal distribution were expressed as median values with range. In the analysis of quantitative independent variables, Mann–Whitney U test was used. Wilcoxon test was used to assess the differences between dependent quantitative variables. Correlation between two variables was evaluated by Spearman correlation test. The results were evaluated in 95% confidence interval, and p < 0.05 was considered statistically significant.
Results
Between March 2013 and June 2019, 1400 patients underwent different types of BS, and 1333 patients who underwent LSG were enrolled in this study. The mean age was 40.93 ± 10.86; 954 (71.5%) patients were female. The baseline characteristics are summarized as shown in Table 1. The most common comorbid diseases were arterial hypertension in 399 patients (29.9%), hyperlipidemia in 465 patients (34.9%), diabetes in 336 patients (25.2%), sleep apnea syndrome in 317 patients (23.8%), and insulin resistance (IR) in 666 patients (50%). Remission rates are given in Table 2.
Demographic Characteristics and Preoperative Values
BMI, body mass index; HbA1c, glycosylated hemoglobin; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment insulin resistance; LDL, low-density lipoprotein; LSG, laparoscopic sleeve gastrectomy; SD, standard deviation; TC, total cholesterol; TG, triglycerides.
Comorbidities and Remission Rates
During a 2-year period, we observed a significant increase in the EWL%. The EWL% at the 1st, 3rd, 6th, 12th, and 24th months was 29.75 ± 11.47, 55.32 ± 18.34, 77.72 ± 23.40, 93.06 ± 25.13, and 90.72 ± 25.52, respectively. EWL% change was significantly higher at 1st, 3rd, 6th, and 12th months (p < 0.0001). EWL% was not significant between the 12th and 24th months (p = 0.71) (Fig. 1).
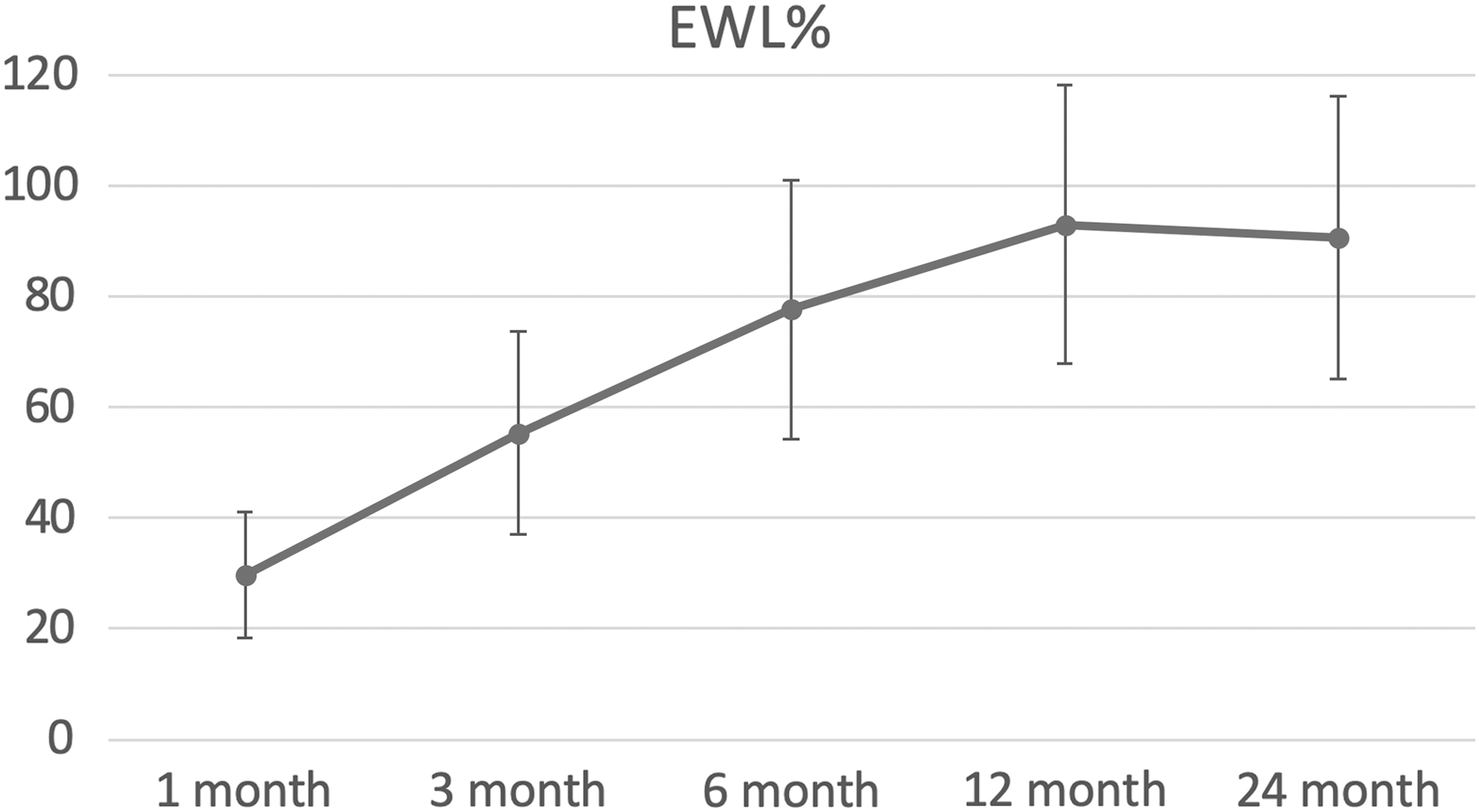
EWL% during study. EWL%, percentage of excess weight loss.
Compared to the preoperative levels, the mean fasting glucose levels decreased after 3 months (92.81 ± 19.16, p < 0.0001), 6 months (90.31 ± 13.04, p < 0.0001), 12 months (89.98 ± 18.13, p < 0.0001), and 24 months (87.13 ± 11.68, p < 0.0001). There was no significant difference concerning blood glucose levels between 12 and 24 months (p = 0.271).
The HbA1c levels decreased from 6.18 ± 14.36 to 5.44 ± 2.80 (p < 0.0001) after 3 months, to 5.31 ± 1.50 (p < 0.0001) after 6 months, to 5.47 ± 3.82 (p < 0.0001) after 12 months, and to 5.21 ± 0.35 (p < 0.0001) after 24 months. The fasting insulin level was significantly decreased compared to the preoperative level of 24.77 ± 15.80. It decreased to approximately one-third of the preoperative level at 3 months (9.85 ± 6.07, p < 0.001), and it decreased even further at 6 months (8.23 ± 5.02, p < 0.001), at 12 months (6.74 ± 5.20, p < 0.001), and 24 months (7.33 ± 4.54, p < 0.0001) after surgery.
A downward trend was also observed in the HOMA-IR level, which was rapid at the 3rd month (2.27 ± 1.5, p < 0.001) and slower at the 6th (1.88 ± 1.25, p < 0.001) and 12th (1.52 ± 1.18, p < 0.001) months.
We detected a significant decrease in TC and LDL levels at 3 months (204.66 vs. 191.74, p < 0.0001 and 136.90 vs. 131.99, p < 0.01, respectively); after 3 months, both the TC and LDL levels increased to preoperative levels.
The TG levels showed a consistent decrease at 3 (113.32 ± 41.10, p < 0.0001), 6 (101.24 ± 40.59, p < 0.0001), 12 (88.04 ± 38.85, p < 0.0001), and 24 (83.40 ± 34.47, p < 0.0001) months.
The change in the HDL level at the 3rd month (47.22 ± 14.03) was not statistically significant (p = 0.185); however, after 6 (52.74 ± 14.63, p < 0.0001), 12 (58.80 ± 14.21, p < 0.0001), and 24 (62.98 ± 15.43) months, greater changes were observed (Table 3).
Changes in Variables and p-Values
Statistically significant.
Changes of biochemical parameters for 2 years were calculated and correlated with age, BMI, and EWL%. Negative correlations were found between preoperative BMI and change in TC or LDL levels (r = −0.200, p = 0.014; r = −0.221, p = 0.006, respectively). Positive correlations were found between preoperative BMI and changes of glucose, HbA1c, insulin, or HOMA-IR (r = 0.243, p = 0.002; r = 0.321, p < 0.001; r = 0.377, p = 0.001; r = 0.305, p = 0.008, respectively). Positive correlation was found between mean age of patients and change of glucose (r = 0.219, p = 0.007) and negative correlation between age of patients and EWL% (r = −0.228, p < 0.001). Change of TC and LDL levels was positively correlated with EWL% (r = 0.307, p < 0.001; r = 0.379, p < 0.001).
Discussion
Obesity and its related comorbidities are increasing worldwide and becoming a global epidemic. It is thought that obesity currently affects at least 400 million adults, and 30% of the U.S. population will have a BMI >30 kg/m2 in 2030.15,16 Moreover, it is responsible for many comorbid diseases such as arterial hypertension, T2DM, dyslipidemia, CVD, obstructive sleep apnea syndrome, hepatic steatosis, depressive syndromes, and osteoarthritis. 17 The effectiveness and permanence of BS in weight loss and treatment of obesity related comorbidities have been proven. 10 LSG is one of the most popular bariatric surgical treatment modalities for obesity and comorbidities worldwide. Moreover, it is the most commonly performed BS in the United States and in the Asia-Pacific region. 18
In LSG, 70–80% of the stomach along the greater curvature is surgically removed. The effect of the procedure consisted of a reduced volume of consumed food and loss of appetite due to decreased secretion of ghrelin and reduced nerve signaling. 11 The latter two effects are attributed to hormonal changes after surgery.11,12 LSG reduces ghrelin and increases incretins such as GLP-1 and GIP, which act together, and both enhance glucose-dependent insulin production at the pancreatic β-cells. In diabetic individuals, the secretion of GLP-1 and response to GIP are blunted. Therefore, it is estimated that LSG itself may be effective in remission of T2DM as much as gastric bypass (GB) procedure. And the effects may be attributed to hormonal changes, which are provided by LSG. In addition to this, a recent meta-analysis has shown that LSG and GB are both effective on T2DM resolution. 19 This study has shown that LSG has accomplished complete and partial remissions in DM in 81% and 18%, respectively. In only 1% of the patients, we did not see any remission. Therefore, we believe that LSG may be effective in treating T2DM, which is secondary to obesity. In contrast, LSG effectively decreases glucose, insulin, and HbA1c levels; in accordance with improvement of glucose metabolism IR is also improved.10,20
One of the common comorbidities of obesity is a deranged lipid profile and it is associated with CVD. Hence, improvement in hyperlipidemia may prevent CVD, and LSG may be effective in treating and preventing the disease. Our findings have shown that complete or partial remission of hyperlipidemia can be achieved in 93.3% of the patients after LSG. Likewise, a 1-year study showed improvement and remission rates of hyperlipidemia of about 50–78%, and 2-year study showed 66–87% improvement and remission, respectively.21–25 Moreover, low HDL and high TG levels are common risk factors for CVD. In general, malabsorptive methods improve all values of lipid profile, while restrictive methods are known to increase HDL and decrease TG. However, some authors have also shown that restrictive methods may make moderate changes in TC levels.21,22,26–29 In our series, we saw statistically significant decrease in TG and increase in HDL after 2 years follow-up, but we did not see any change in TC and LDL levels. Apart from the levels of lipid profile, the ratio of lipid parameters is also important. Praveen Raj et al. 30 reported that TC/HDL ratio is associated with an increased risk of CVD, and this ratio is decreased after LSG (p = 0.002). Buchwald et al. found in their meta-analysis that improvement of dyslipidemia after BS was 70%, and they have seen maximum improvement after malabsorptive procedures. 10 Similarly, Pontiroli et al. showed that malabsorptive procedures are more effective than restrictive procedures in reducing cholesterol levels. 31
Evidence suggests that weight loss can effectively improve MetS and its components. BS is a good treatment option to achieve this goal. 20 It provides not only weight loss but also resolves obesity related comorbidities, T2DM, arterial hypertension, dyslipidemia, and CVD risk.10,32
Today, the most important discussion among bariatric surgeons is the type of surgery, which will provide the most benefit and least harm for the patient. Generally, it is believed that malabsorptive procedures, such as biliopancreatic diversion with duodenal switch, provide more weight loss and improvements of comorbidities than restrictive techniques, but they have higher postoperative complications.33,34 Biliopancreatic diversion with duodenal switch has been reported to provide the highest EWL% and resolution of T2DM with rates as high as 95.1%. 10 Nevertheless, our findings showed that LSG has comparable results concerning resolution of MetS, T2DM, and hypertension in 2-year follow-up. GB was the most common method for many years with high remission rates. 35 The use of LSG has increased due to its low complication rates, short operative time, and ease of use. And preserving endoscopic access and retaining the possibility for a second surgical procedure are the other advantages.36,37
Some comparative trials showed that LSG and GB have similar or near-similar results.20–23,38,39 Moreover, as LSG is surpassing GB in numbers at many centers worldwide, 35 more is being learned about the different aspects of its mechanisms and effects.
A recent meta-analysis showed that GB and LSG induce a comparable glycemic control; besides GB provides higher EWL%, hypertension, and dyslipidemia improvements. 19
Body weight loss after LSG is effective and satisfying for patients and leads to improvement of quality of life. 40 This study has shown that EWL% is significantly increased in the first year after LSG. The EWL% change did not differ significantly between the first and the second year.
Conclusion
Hence, we believe that maximum change after LSG is achieved at the first year and may be a good sign of provision regarding weight loss expected for patient.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest. No competing financial interests exist.
Funding Information
No funding was received for this article.