
Abstract
Introduction:
Little is known of the effects of bariatric surgery on type 1 diabetes mellitus (T1DM). Systemic reviews of various case reports and a number of original articles in the literature show mixed effects of surgery on HbA1c and daily insulin requirements in patients with T1DM. The aim of this study is to assess the impact of bariatric surgery on obesity, obesity-related conditions, and glycemic control in patients with T1DM.
Methods:
We retrospectively reviewed 13 patients with obesity and insulin-dependent diabetes mellitus (T1DM) at four different institutions between 2012 and 2016. The diagnosis was confirmed by the presence of autoantibodies known to be associated with T1DM (GAD 65, insulin antibodies) and/or the absence of C-peptide. The primary end points of the study were glycemic control, as measured by HbA1c and the daily insulin requirement. Secondary end points included mean percentage weight loss and resolution rate of comorbidities.
Results:
Of the 13 patients studied 8 (61.5%) were female with a mean age of 39.6 ± 10.1 (30–56) years, and 5 (38.5%) were male with a mean age of 35.6 ± 13.2 (19–52) years. All subjects had a mean preoperative BMI of 45.8 ± 6.8 (35.4–58.6) kg/m2, mean weight of 125.8 ± 20.7 (93–161) kg, and a mean preoperative HbA1c of 8.3 ± 1.5 (6.6–12.2)%. Mean daily insulin requirement (the sum of the basal and premeal bolus doses), among all patients, was 120.6 ± 58.9 (50–220) units. Ten (76.9%) patients had dyslipidemia, eight (61.5%) patients had hypertension, and five (38.5%) had obstructive sleep apnea. Ten (76.9%) patients underwent a laparoscopic sleeve gastrectomy, two (15.4%) had laparoscopic Roux-en-Y gastric bypasses, and one (7.7%) patient underwent a single anastomosis bypass. There was a significant difference in mean weight loss from baseline to the weight at every interval follow-up (p-value <0.05). A significant difference in mean decrease in HbA1c was found from baseline to 6- and 12-month follow-up (p-value <0.05). There was both a clinically and statistically significant difference in mean daily insulin requirement, between the preoperative and follow-up doses.
Conclusions:
This study demonstrates that bariatric surgery can be an effective adjunct in the management of T1DM, in association with obesity. The results of our investigation revealed sustained improvement in weight, significant short-term improvement in HbA1c, and significant reduction in daily insulin requirements. Larger prospective randomized controlled studies will need to be done to confirm these findings and to evaluate if these improvements are sustained.
Introduction
The safety and efficacy of bariatric surgery has been well established.1–4 Bariatric surgery is also known as metabolic surgery, which is more fitting given the significant improvement, and in some cases complete resolution of patients' obesity-related conditions (i.e., type 2 diabetes mellitus [T2DM], hypertension, dyslipidemia, reflux disease, nonalcoholic fatty liver disease, and sleep apnea).1,4 The degree of weight loss and resolution rates of comorbidities vary based on the type of bariatric surgery done. For example, restrictive and metabolic procedures (i.e., gastric bypass and biliopancreatic diversions) can expect to see 70–80% EWL and a 70–80% remission rate of T2DM, whereas purely restrictive procedures (i.e., sleeve gastrectomy and gastric banding) can expect a 40–50% EWL and ∼50% remission rate of T2DM. The other obesity-related conditions have similar remission rates after surgery.5,6 Studies have shown that patients with T2DM achieve better glycemic control after bariatric surgery than on conventional medical therapy alone.3,5,6 By contrast, little is known of the effects of bariatric surgery on type 1 diabetes mellitus (T1DM). Systemic reviews of various case reports, and a number of original articles in the literature show mixed effects of surgery on HbA1c and daily insulin requirements in patients with T1DM.1–4,7–11 What is evident is the positive effect it has on the degree of weight loss and other obesity-related conditions.1,2,7,11
Recent reports indicate an increase in prevalence of obesity in patients suffering from T1DM. Upward of 12.6% of adolescent patients and 50% of adult patients are overweight or obese, with approximately one-third meeting criteria for metabolic syndrome. 1 Excess body weight can have a significant effect on the course of diabetes. Obesity-associated peripheral insulin resistance could potentially accelerate the rate of T1DM development in those who have a genetic predisposition. Conversely, medical management with exogenous insulin for T1DM in patients with obesity can exacerbate the latter condition because of the innately anabolic effects of this administered hormone.1,3,8
The exact mechanism by which bariatric surgery results in remission and/or resolution of diabetes mellitus is not clearly understood. Recent studies have revealed a fifth islet peptide—ghrelin, which is also present in large amounts in the fundus of the stomach. This peptide is known to be appetite stimulating, with elevated levels appreciated in patients with obesity. Ghrelin has also been shown to block insulin effects on the liver and beta cell response to nutrient and/or hormonal stimuli. Therefore, some credit can be lent to the removal of a significant source of this antagonizing peptide.12–14 The aim of this study is to assess the impact of bariatric surgery on obesity, obesity-related conditions, and glycemic control in patients with T1DM.
Methods
All research was conducted after approval from the Institutional Review Board. We retrospectively reviewed 13 patients with obesity and insulin-dependent diabetes mellitus (T1DM) at four different institutions between 2012 and 2016. Besides young age of onset, the diagnosis of T1DM was confirmed by the presence of autoantibodies known to be associated with this disease process (i.e., glutamic acid decarboxylase [GAD 65] antibody and insulin autoantibodies).
The primary end points of the study were glycemic control, as measured by HbA1c and the daily insulin requirement. Secondary end points included mean percentage weight loss and resolution rate of comorbidities. Comorbidities included hypertension, defined as a measured blood pressure ≥140/90 mmHg, and/or taking one or more antihypertensive medications. Hypertension was considered resolved once medications were no longer needed to keep blood pressure within normal range. Obstructive sleep apnea (OSA), defined as the need for consistent use of a continuous positive airway pressure mask. Sleep apnea was considered resolved if mask use was no longer needed. Dyslipidemia, defined as measurable hypercholesterolemia and/or hypertriglyceridemia. We analyzed data preoperatively, at 6, 12, 18, and 24 months follow-up. Data were reported as mean ± standard deviation (range). We assessed for significant differences in mean outcomes measured between preoperative measurements and subsequent data measured at 6, 12, 18, and 24 months follow-up using paired t-tests to generate a two-tailed p-value. Statistical significance was defined as a p-value <0.05. Calculations were performed with LaTeX.
Results
Of the 13 patients studied 8 (61.5%) were female with a mean age of 39.6 ± 10.1 (30–56) years, and 5 (38.5%) were male with a mean age of 35.6 ± 13.2 (19–52) years. All subjects had a mean preoperative BMI of 45.8 ± 6.8 (35.4–58.6) kg/m2, mean weight of 125.8 ± 20.7 (93–161) kg, and a mean preoperative HbA1c of 8.3 ± 1.5 (6.6–12.2)%. Mean daily insulin requirement (the sum of the basal and premeal bolus doses), among all subjects, was 120.6 ± 58.9 (50–220) units. Ten (76.9%) patients had dyslipidemia, eight (61.5%) patients had hypertension, and five (38.5%) had OSA. The mean preoperative low-density lipoprotein level (LDL), high-density lipoprotein level (HDL), and triglyceride level were 137.3 ± 36.2 (68–190), 42.8 ± 10.2 (33–70), and 146.5 ± 52.5 (55–213), respectively. Ten (76.9%) patients underwent a laparoscopic sleeve gastrectomy (LSG), two (15.4%) had laparoscopic Roux-en-Y gastric bypasses (LRYGB), and one (7.7%) patient underwent a single anastomosis bypass. The number of patients to follow-up was 12 (92.3%), 7 (53.8%), 4 (30.7%), and 2 (15.4%) at 6, 12, 18, and 24 months, respectively. Patient demographics are detailed in Table 1.
Demographics and Baseline Data
LRYGB, laparoscopic Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy; n, sample size.
Table 2 details the outcomes data preoperatively and at 6, 12, 18, and 24 months. There was a decrease in weight of 26.9%, 35.5%, 38.4%, and 39% at 6, 12, 18, and 24 months, respectively. There was a significant difference in mean weight loss from baseline to the weight at every interval follow-up (p-value <0.05). There was a significant difference in mean decrease in HbA1c from baseline to 6- and 12-month follow-up (p-value <0.05), but no significance was found at 18- or 24-month follow-up (p-value >0.05).
Outcomes Data
HDL, high-density lipoprotein level; LDL, low-density lipoprotein level.
Three (37.5%) patients with hypertension saw improvements in their blood pressure, two (40%) patients with OSA saw resolution or improvement in their condition, and five (50%) patients with dyslipidemia saw improvements in their cholesterol and triglyceride levels. Relative to the preoperative measure, there was only a significant difference in mean LDL level at 12-month follow-up; otherwise, no significant difference was appreciated. When compared with the preoperative measure, there was only a significant difference in mean HDL level at 6- and 12-month follow-up; otherwise, no significant difference was appreciated. Finally, there was no significant difference found between mean pre- and postoperative triglyceride level, at any interval follow-up time.
Among the patients who had follow-up data all but one had decrease in daily insulin requirements. The mean daily insulin requirement at follow-up was 23.1 ± 19.2 (0–60) units. There was both a clinically and statistically significant difference in mean daily insulin requirement, between the preoperative and follow-up (Fig. 1). Finally, four (30.8%) patients experienced a postoperative episode of diabetic ketoacidosis (DKA), with three patients experiencing DKA within 30 days postoperatively, and one patient experiencing an episode of DKA at ∼7 months postoperatively.
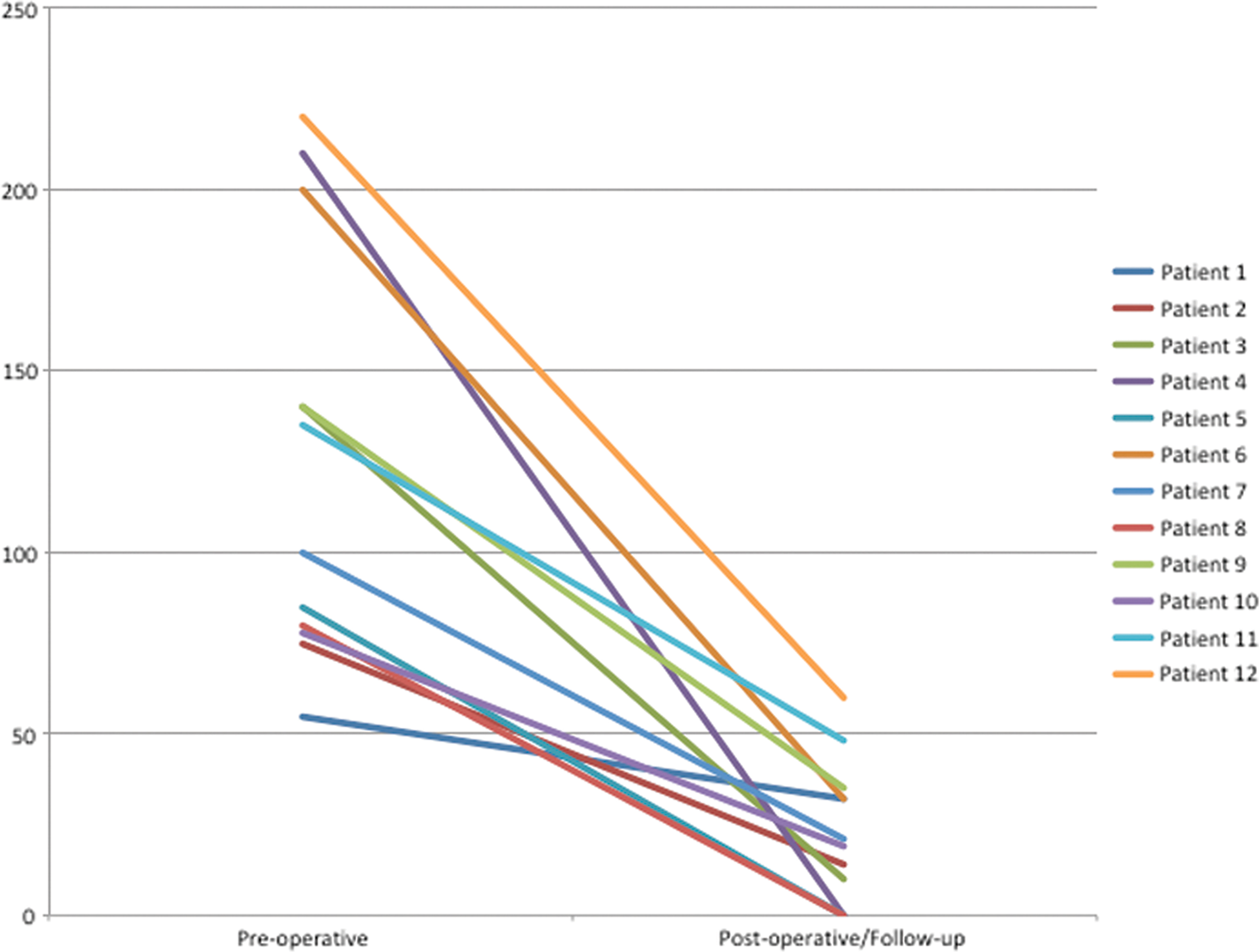
Daily insulin requirement. Preoperative daily insulin requirement saw a statistically and clinically significant improvement among all patients who followed up (n = 12). Color images are available online.
Discussion
T1DM and T2DM are two different pathologies, in that they have different etiologies and clinical courses. The former commonly arises in adolescence and occurs as a result of autoimmune destruction of beta islet cells of the pancreas. As a result, patients have inadequate insulin concentrations, with uncontrolled hyperglycemia, leaving these patients prone to complications such as diabetic ketoacidosis. Treatment is aimed at replacing insulin in an attempt to control glycemic levels and avoid long-term neurovascular complications related to chronic hyperglycemia.14,15 T2DM often arises in middle age, associated with obesity and/or other metabolic syndrome-related comorbidities. The underlying pathophysiology is due peripheral insulin resistance followed by exhaustion of pancreatic beta islet cells—due to the constant demand of insulin. The goal of treatment is to lower glucose concentrations and to re-establish insulin sensitivity in peripheral tissues.14,15 The latter pathology has been proven to improve or else completely resolve in response to bariatric surgery.1–4 Some studies have shown improvement in glycemic control, among patients with T1DM, after bariatric surgery—but persistent response has been variable.16,17 Studies from the Diabetes Prevention Trial (DPT-1) suggests that some patients with T1DM do not simply have a linear decline in beta cell mass but have a relapsing and remitting progression of beta cell mass dysfunction. Also, other factors such as the development of insulin resistance can alter the timing of clinical presentation of this pathology. Therefore, this mixed response may be due to the variability in residual beta cell function in different patients, as well as the subsequent effect of obesity-related insulin resistance on remaining beta cell mass. 18
We analyzed the response of 13 individuals, with T1DM, to bariatric surgery. A significant and sustained reduction in weight was appreciated. Resolution rates of obesity-related conditions, in our cohort, did not see comparable rates to what has been published in the literature. Rates may have improved, but there were cases lost to follow-up; therefore, there may have been patients who had resolution that went unreported. We hypothesize that the lack of improvement, of dyslipidemia in particular, suggests that glycemic control can impact the management of patients' lipid profile. There was significant improvement in glycemic control, as measured by improvement in mean HbA1c and daily insulin requirements. The significant improvement in mean HbA1c levels saw a plateau after 6 and 12 months. There was an overall lack of power (i.e., inadequate sample size) at 18- and 24-month follow-up visits. Even with significant improvement in daily insulin requirement, the majority of patients' still required daily insulin to control their serum glucose levels. As mentioned earlier, T1DM is an autoimmune disease with destruction of nonregenerative cells. A decrease in daily insulin requirement is, therefore, clinically significant. A very important point of consideration is the fact that according to data from a “placebo-controlled populations in clinical interventions trials” suggest that some patients with T1DM will have persistent beta cell function even years after diagnosis. 18 This may explain that a small subset of patients with T1DM will have resolution of their diabetes after weight loss surgery.
Patients with T1DM require continuous exogenous insulin not only for the distribution of the blood glucose but also to prevent the formation of ketoacids and subsequent development of DKA. DKA can be triggered when insulin is held or reduced in the context of a patient with no oral intake or reduced intake in the perioperative period or when minimal carbohydrates are being ingested in the first few postoperative days. 19 In our cohort there were four of cases of DKA, with three occurring in the immediate postoperative period (within 30 days), and with one case presenting further out (∼7 months postoperatively). This exemplifies the need to maintain very strict glucose control during the perioperative period.
Our study shows that bariatric surgery can lead to significant sustained weight loss, improvement in metabolic profile, and better glycemic control—in specific patients with obesity and T1DM. This improved metabolic profile may potentially help facilitate better medical management of T1DM in the setting of obesity and obesity-related conditions.
Conclusion
This study demonstrates that bariatric surgery can be an effective adjunct in the management of T1DM, in association with obesity. The results of our investigation revealed sustained improvement in weight, significant short-term improvement in HbA1c, and significant reduction in daily insulin requirements. Larger prospective randomized controlled studies will need to be done to confirm these findings and to evaluate if these improvements are sustained.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.