
Abstract
Background:
Despite rising rates of obesity among human immunodeficiency virus (HIV)-positive individuals, the safety and tolerability of surgery in this population have not been established. The primary aim of this study was to examine the safety of bariatric surgery and rate of in-hospital postoperative complications in morbidly obese patients with HIV.
Materials and Methods:
The U.S. Nationwide Inpatient Sample database was queried between 2004 and 2014 for discharges with codiagnoses of morbid obesity and bariatric surgery. The primary outcome was in-hospital mortality. Secondary outcomes included length of stay, hospitalization costs, and multiple categories of complications, including systemic complications, surgical complications, and nutritional and behavioral complications.
Results:
Among 267,082 patients with discharge diagnoses of morbid obesity and bariatric surgery, 346 (0.13%) were diagnosed with HIV. On multivariable analysis, HIV did not influence in-hospital mortality (p = 0.530). HIV was not associated with increased risk of renal failure (p = 0.274), thromboembolism (p = 0.713), myocardial infarction (p = 0.635), sepsis (p = 0.757), hemorrhage (p = 0.303), or wound infection (p = 0.229). Other measured surgical complications were not significantly different (p > 0.05). Notably, HIV-positive patients had an increased risk for postoperative pneumonia (p = 0.002), pancreatitis (p = 0.049), and thiamine deficiency (p = 0.016).
Conclusion:
Bariatric surgery among HIV-positive patients appears to be acceptably safe with the risk of postoperative complications comparable with non-HIV patients.
Introduction
Human immunodeficiency virus (HIV) infection has seen a radical shift in management strategy and treatment efficacy within the last 3 decades. 1 The advent of antiretroviral therapies in the 1990s led to a reduced incidence of acquired immunodeficiency syndrome (AIDS)-defining opportunistic infections, thus improving life expectancy and overall survival. 2 Within the last decade alone, the life-expectancy of HIV-positive patients was found to approach that of non-HIV-infected populations, likely due to a combination of less toxic antiretroviral drugs, improved adherence, prophylactic measures, and management of comorbidities. 3 However, as further development and innovation of potent antiretroviral therapy have improved HIV disease outcomes, clinicians face new challenges associated with caring for the HIV population. 4
One of these challenges lies in the recognition and management of obesity among a population that previously struggled with malnutrition and undernourishment. Obesity among HIV-positive patients is more prevalent than previously estimated and demonstrates a rising trend comparable with the general population.5,6 Among the general populace of the United States, obesity has reached pandemic levels and is estimated to be present in more than 35% of adults. 7 According to a recent National Health and Nutrition Examination Survey, obesity among HIV-positive patients is common, affecting 40% of HIV-infected women and 20% of HIV-infected men. 6 As such, HIV-positive patients are prone to a myriad of comorbid issues associated with obesity and its sequelae.
While weight gain was traditionally viewed as a coveted goal for HIV-positive patients, weight gain predisposing to obesity and metabolic syndrome is not desirable and may pose substantial, unintended adverse outcomes. Excessive weight gain and morbid obesity lead to an overall increase in morbidity (i.e., cardiovascular disease, type 2 diabetes mellitus, and cancers) and all-cause mortality. 8 Predisposing to this general trend of obesity among HIV populations is the evolution of clinical care and role of effective antiretroviral therapy. Treatment with combined antiretroviral therapy has been associated with weight gain and multiple metabolic problems such as dyslipidemia, lipodystrophy, insulin resistance, and increased risk of vascular disease.9–11
Concurrent with the rising incidence of obesity among HIV-positive patients, investigating potential weight loss strategies relevant to this patient population is important. Although bariatric surgery has been proven to be the most effective and durable weight loss option for the general population, bariatric intervention in the HIV population may be more challenging given concerns regarding the absorption and efficacy of antiretroviral therapies postprocedure.12,13 Bariatric surgery among the HIV-positive patient population has not been extensively investigated, and no specific study has evaluated immediate, in-hospital postoperative complications. Therefore, the primary aim of this study was to examine the safety and in-hospital postoperative complications of bariatric surgery on morbidly obese HIV-positive patients. We hypothesized that bariatric surgery would be a safe procedure among morbidly obese patients with HIV and would be associated with similar postoperative outcomes compared with the general population.
Materials and Methods
Data source and study population
The study sample originated from the Nationwide Inpatient Sample database, which includes hospitalized patients in the United States during the 2004 to 2014 period. This registry is part of the Healthcare Cost and Utilization Project, sponsored by the Agency for Healthcare Research and Quality. The Nationwide Inpatient Sample is a database of hospital inpatient stays derived from billing data submitted by hospitals to statewide data organizations across the United States. Inpatient data include clinical and resource use information typically available from discharge abstracts. Each discharge is coded with a principal diagnosis for that specific hospitalization in addition to the potential for 14 secondary diagnoses and 15 associated procedures. The Nationwide Inpatient Sample is the largest U.S. inpatient care database encompassing hospitals from a total of 46 states, which serve 97% of the U.S. population.
Inclusion and exclusion criteria and bariatric surgery assessment
Patients were included if they had a primary or secondary diagnosis of morbid obesity and bariatric surgery. These conditions were identified using the International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) codes. Patients were then classified based on their HIV-positive or -negative status. HIV was defined based upon ICD-9-CM codes 042, 043, 044, V08, and 079.53, as previously validated. 12 Morbid obesity was defined by ICD-9-CM codes 278.01, V85.35, V85.36, V85.37, V85.37, V85.38, V85.39, V85.40, V85.41, V85.42, V85.43, V85.44, and V85.45 in accordance with prior studies.14,15 Among the included patients with morbid obesity and HIV, hospitalizations with a history of prior bariatric surgery (Roux-en-Y, gastric band, and sleeve gastrectomy) were identified using the following ICD-9-CM codes: laparoscopic or open Roux-en-Y gastric bypass (ICD-9-CM 44.31, 44.38, and 43.39), laparoscopic adjustable gastric band (ICD-9-CM 44.95), and laparoscopic sleeve gastrectomy (ICD-9-CM 43.82).14,15
Covariates and outcome measures
Demographic and clinical characteristics were compared between patients with and without a history of bariatric surgery. The covariates included demographic data (age, gender, and race/ethnicity) as well as characteristics related to metabolic syndrome and obesity-related outcomes. Hospitalization data such as day of admission (weekday or weekend), route of admission, mean length of hospital stay, hospitalization charges, and primary payer source were also included. The primary outcome of this study was to assess the safety of bariatric surgery among HIV-positive patients, as determined by mortality between the two cohorts. Secondary outcomes included clinically relevant, in-hospital, postweight loss surgery complications. Postoperative bariatric surgery complications were classified into broad categories: systemic complications, surgical complications, and nutritional and behavioral complications.16,17
Systemic complications included renal failure, thromboembolism, pneumonia, sepsis, pancreatitis, cellulitis, esophagitis, myocardial infarction, pulmonary compromise, and urinary tract infections. Surgery-specific complications related to hemorrhage, wound infection, need for ostomy, need for reoperation, marginal ulcer formation, gastric perforation, stricture or fistula formation, and bowel obstruction or incarceration. Nutritional complications included anemia, thiamine and zinc deficiency, malnutrition, failure to thrive, and dumping syndrome. Behavioral complications included alcohol use, anorexia, and bulimia. Details on the covariates are highlighted in Appendix Table A1.
Statistical analyses
Categorical variables are presented as counts and proportions, and differences tested using Pearson's chi-square test. Continuous variables are presented as mean (standard deviation), and differences between groups were tested using the t-test. The age-adjusted mortality rate was calculated for each year of study by summing the product of age-specific mortality rates by the age-specific weights. For population trends, the total number of cases was standardized per 100,000 based upon the total population derived from the U.S. census data for a specific year (2004–2014). 15 The weights used in the age adjustment of data were the proportion of the year 2000 standard U.S. population within each age group. 16
Secular trends in mortality rates were assessed using linear Poisson regression models. The models were used to investigate the effect of the period of diagnosis (independent variable) on the in-hospital mortality rate (dependent variable) while controlling for other variables (i.e., adjusting for age, sex, race, income, insurance status, type of admission, and modified Elixhauser comorbidity index, including hypertension, coronary artery disease, hyperlipidemia, cerebrovascular accident, congestive heart failure, and polycystic ovarian syndrome). Risk estimates and 95% confidence intervals (CIs) were calculated for all independent variables in the final model. Poisson regression with robust (Huber–White) standard errors was also used to determine incident risk ratios (IRRs) for predictors of in-hospital mortality. Before our analysis, we tested the Poisson models for overdispersion using a Pearson goodness-of-fit test. Models were not overdispersed; thus, Poisson regression was then used to determine IRRs for clinical outcomes in patients with HIV and bariatric surgery compared with those without HIV who underwent bariatric surgery.
All the analyses accounted for clustering and sampling weights. The Healthcare Cost and Utilization Project Nationwide Inpatient Sample has a two-stage cluster design incorporating clustering at the hospital level and discharge level. The weighting of discharges is based on the hospital type and volume of discharges relative to the sampling region. Analyses were performed using Stata, version 15.0 (Stata LP, College Station, TX). All p-values were based on two-sided tests and were considered statistically significant at p-value <0.05. According to the data user agreement, any individual table cell counts of 10 or fewer cannot be presented to preserve patient confidentiality. In such instances, data are suppressed and labeled as information suppressed.
Results
Demographic and patient population characteristics
A total of 267,082 patients with discharge diagnoses of morbid obesity and bariatric surgery were included in our study, of which 346 (0.13%) were diagnosed with HIV infection. Patients with HIV, morbid obesity, and bariatric surgery were younger compared with patients without HIV infection (mean age of 42.9 ± 8.6 years vs. 44.3 ± 11.7 years, respectively; p < 0.001). A majority of included patients in this study, both with and without HIV infection, were female, although a higher percentage of women with HIV underwent bariatric surgery (p < 0.001). Racial/ethnic differences were significant as well among the cohorts (p < 0.001). For HIV patients, the length of hospital stay was significantly shorter (2.28 ± 1.84 days vs. 2.31 ± 3.1 days; p < 0.001), although hospitalization cost was higher ($45,206 ± $31,198 vs. $42,650 ± $36,381; p = 0.002, respectively). Study characteristics and baseline demographic and hospitalization characteristics of patients, by HIV-positive and HIV-negative status, are further presented in Table 1.
Characteristics of Hospitalized Patients with Morbid Obesity and Bariatric Surgery
Data are counts (percentage). According to the data user agreement, any individual table cell counts of 10 or fewer cannot be presented to preserve patient confidentiality. In such instances, data are suppressed.
HIV, human immunodeficiency virus; IS, information suppressed.
With regard to several comorbidities, patients with bariatric surgery and HIV were significantly different from non-HIV patients (hypertension: 52.0% vs. 51.8%, p = 0.008; coronary artery disease: p = 0.55; polycystic ovarian syndrome: p = 0.42; cerebrovascular accident: p = 0.03, and congestive heart failure, p = 0.03, respectively).
Bariatric-associated mortality and systemic complications
Based upon the decade of study, HIV did not appear to play a significant factor in overall postbariatric surgery complications. Associations with common, systemic postoperative complications, including acute renal failure and thromboembolism, were similar between HIV and non-HIV patients (p = 0.274 and p = 0.713, respectively) (Table 2). While the risk of postoperative pancreatitis was significantly higher among HIV-positive patients (0.29% vs. 0.04%; p = 0.021), myocardial infarction and pulmonary compromise postbariatric surgery were similar among the two cohorts (p = 0.635 and p = 0.357, respectively).
Mortality and Complications Among HIV-Positive Patients with Bariatric Surgery Versus HIV-Negative Patients with Bariatric Surgery
According to the data user agreement, any individual table cell counts of 10 or fewer cannot be presented to preserve patient confidentiality. In such instances, data are suppressed.
IRR adjusted for age, sex, race, income, insurance status, type of admission, and modified Elixhauser comorbidity index, including hypertension, hyperlipidemia, and coronary artery disease.
CI, confidence interval; ETOH, alcohol use; IRRs, incident risk ratios.
With regard to postoperative infections, the rates of cellulitis and urinary tract infections were similar among the two groups (p = 0.827 and p = 0.090), respectively. Despite this similarity, postoperative pneumonia was significantly higher among HIV-positive patients compared with non-HIV bariatric surgery patients (2.02% vs. 0.62%; IRR 3.21; 95% CI 1.53–6.75; p = 0.002). Although the risk of pneumonia was higher for HIV patients, risk of sepsis was not significantly different (0.58% vs. 0.46%; p = 0.757). Mortality rates between the two cohorts, morbidly obese patients with and without HIV infection, were nonsignificant (p = 0.530). Among patients with HIV, no mortality events during hospitalization were reported in our study. Patients undergoing bariatric surgery without HIV demonstrated an in-hospital mortality rate of 0.11%. Additional overall complications were nonsignificant and are highlighted in Table 2.
Surgical complications
Bleeding and surgical complications were also measured as components reflecting overall safety of bariatric surgery. Risk of hemorrhage, wound infection, ostomy, and need for reoperation were not different among HIV-positive and HIV-negative individuals (0.58% vs. 1.18%; p = 0.303, p = 0.229, p = 0.801, and p = 0.483, respectively) (Table 2). On further exploration, postoperative measures, including the risk for marginal ulcer formation or gastric perforation, were also similar among groups (p = 0.766 and p = 0.935, respectively). Additionally, bowel complications, including stricture and fistula formation as well as bowel obstruction and incarceration, were not significant (p = 0.564, p = 0.058, p = 0.217, and p = 0.165, respectively).
Nutritional and behavioral complications
Among a variety of nutritional complications associated with bariatric surgery, only in-hospital thiamine deficiency was noted to be significantly different among HIV patients (0.58% vs. 0.10%; IRR 5.55; 95% CI 1.38–22.9; p = 0.016) (Table 2). The risk for anemia and zinc deficiency as well as malnutrition and failure to thrive was similar (p = 0.290, p = 0.591, p = 0.0.875, and p = 0.901, respectively). Dumping syndrome was also not significant among HIV and non-HIV patients (p = 0.744). Alcohol use, anorexia, and bulimia were not different (p = 0.557, p = 0.889, and p = 0.0.757, respectively).
Trends in obesity and bariatric surgery use
Trends of obesity surgery among HIV patients compared with the total number of bariatric surgeries as adjusted for the proportion of discharges demonstrated an annual percent change of +0.02% from 2004 to 2014 (Fig. 1). The overall number of bariatric surgeries in morbidly obese HIV patients increased ∼6.3 times the previous number of procedures performed from 2004 (n = 12) to 2014 (n = 76) (Table 3).
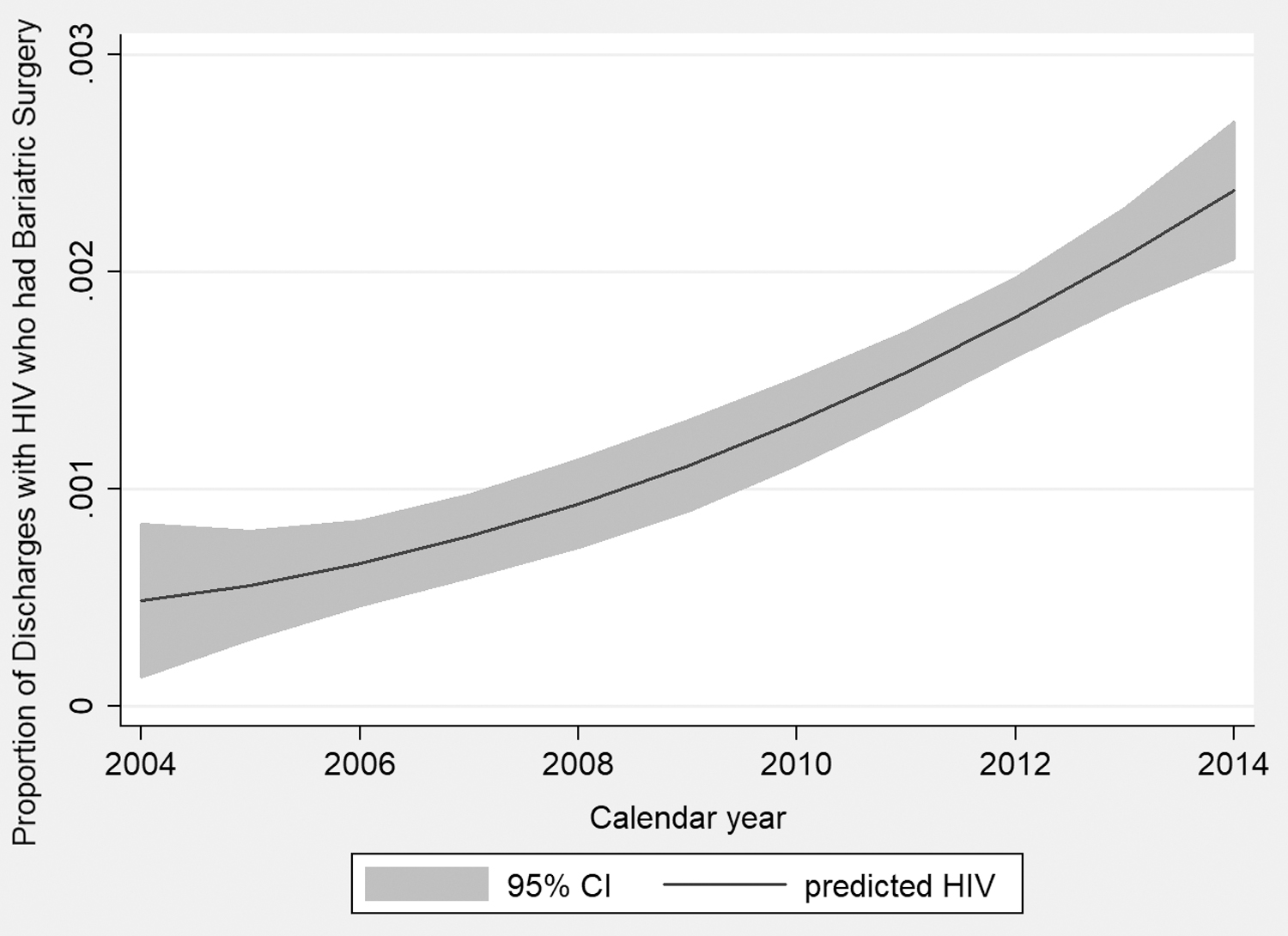
Proportion of discharges in patients with HIV and bariatric surgery, 2004–2014. HIV, human immunodeficiency virus.
Trends in Bariatric Surgery Among Patients with Morbid Obesity with and without HIV
According to the data user agreement, any individual table cell counts of 10 or fewer cannot be presented to preserve patient confidentiality. In such instances, data are suppressed.
Discussion
Using the U.S. Nationwide Inpatient Sample database, we found that bariatric surgery is an acceptably safe procedure among morbidly obese patients with HIV. Despite having many similar postoperative outcomes, our analysis of more than 267,082 discharges found bariatric surgery among HIV patients to be an uncommon practice—only 0.13% of all bariatric surgeries were in HIV patients. Moreover, although HIV causes many systemic problems for patients, HIV-positive individuals appear to have rates of postoperative complications and procedure-associated mortality rates similar to the general population.
Weight loss strategies
Alleviating the effects of obesity in any patient, HIV positive or not, traditionally falls into three general categories: lifestyle modification, pharmacotherapy, and bariatric surgery. 18 Lifestyle modifications, such as diet and exercise, are first-line measures in reducing excess weight, but have challenges with durability. 19 This may be even truer in HIV-positive patients, who have pharmacological reasons for increased weight gain. Pharmacotherapy for obesity has led to modest reduction in excess weight, with substantial side effects. 20 Bariatric surgery, on the other hand, has been shown to be a safe and effective treatment modality for obese individuals. 21 Currently, bariatric surgery provides the highest level of excess weight loss compared with other presently available methods.22–25
A few case series and case reports have reported the safety of bariatric surgery in morbidly obese patients with HIV, but these reports are limited by their small sample size. Large-scale studies and comparative studies evaluating the trends and outcomes of these novel procedures in obese HIV patients are lacking. In the first retrospective review ever published, six HIV-infected patients underwent roux-en-Y gastric bypass and had outcomes comparable with the general population. 26 All other case series that followed reiterated the safety and efficacy of bariatric surgery in obese HIV patients.27–30 A retrospective review in 2016 reported that bariatric surgery is safe in stable HIV-positive individuals on multidrug therapy. They further added that bariatric surgery had no negative effect on viral suppression. 31 A propensity-matched, comparative retrospective analysis by Sharma et al. also reported bariatric surgery as a safe and feasible procedure in HIV-infected patients, who are well controlled on antiretroviral treatment, with short-term surgical and metabolic outcomes comparable with HIV-negative patients. 32 Our study is consistent with these prior reports in further supporting the role of bariatric surgery for obese HIV patients. Bariatric surgery, which has been generally accepted as the most effective therapy for morbid obesity, should be a reasonable option for many at-risk patients, including those with HIV infection. 21
Safety and complications of bariatric surgery
Overall, our study demonstrates bariatric surgery to be a reliably safe weight loss procedure among a population of HIV-infected individuals. Our primary endpoint of in-hospital mortality was not significantly different between patients with and without HIV infection (p = 0.530). This study complements previous literature to support bariatric surgery in HIV-positive patients.26–29 Additionally, a vast majority of postprocedure complications were also similar among the two cohorts of sample patients, further suggesting a role for bariatric surgery. Systemic complications such as renal failure, thromboembolism, urinary tract infection, and myocardial infarction were all similar between HIV and non-HIV populations. Furthermore, despite some concerns regarding immune status and recovery postprocedure, we found no differences in surgical complications, including wound infection, hemorrhage, or need for repeat surgical procedures. The same is true for a majority of the behavioral and nutritional complications among the two groups. It should be noted that HIV-positive patients were found to have a higher risk of postoperative pneumonia and pancreatitis. Patients who undergo bariatric procedures are at risk of multiple micronutrient deficiency such as vitamin D, calcium, zinc, folate, and vitamin B12. 33 In this study, we noted that the HIV-positive patients who underwent bariatric surgery were at higher risk for thiamine deficiency. Currently, there are no pathophysiologic, virologic, or immunologic measures to explain these specific findings. Nevertheless, providers may need to be cautious during the postoperative period and watch for these potential postbariatric surgery complications.
Strengths and limitations
While these results are important and suggest a potential role for bariatric surgery among this specific patient population, it is important to note that our study is not without limitations. This study's design, retrospective and observational in nature, contributes to several limitations in generalizability and adoption in clinical practice. As this database is based upon discharge diagnoses, our results are only able to record complications that occurred during one inpatient hospital stay. Information on long-term outcomes upon discharge is unavailable in this inpatient database and may underestimate short-term postoperative complications. Furthermore, in this study, it was not possible to differentiate between specific types of bariatric surgeries and complications specific to individual procedures, as well as the impact of antiretroviral therapies. Additionally, there remains the possibility of residual confounding as some important weight loss and HIV-specific covariates (i.e., body–mass index, CD4 count, and viral load) were not available within the database. While body–mass index and HIV disease characteristics are critical factors to determine complications, the inherent limitations of the dataset do not allow us to determine the efficacy of individual bariatric surgeries as well as assess treatment with antiretroviral therapy.
Despite these limitations, our study has several strengths. First, this study relies upon previously validated literature using ICD-9-CM codes that previous studies have used for HIV, morbid obesity, and bariatric surgery populations.34–37 Additional strengths of this article include reproducibility of previously published data. Our primary outcome of mortality was not different between the two groups, suggesting a role for bariatric surgery. Our study found an overall bariatric mortality rate of 0.11%, which is similar to a prior Nationwide Inpatient Sample database study of 0.12%. 38 This is incredibly important as we found no in-hospital deaths among our cohort of HIV patients. Moreover, while we were unable to assess body–mass index and specific HIV disease characteristics, nonmodifiable risk factors such as age, gender, and history of congestive heart failure were reported, all of which have been demonstrated to be predictive factors of mortality in bariatric surgery. 38
Conclusion
In summary, based upon a national U.S. database and results spanning over a decade, bariatric surgery is a safe procedure for patients with HIV infection. Effective weight management strategies, specifically bariatric procedures, are pivotal given the increasing incidence of obesity among HIV-positive patients. Our results suggest that bariatric surgery is associated with similar postoperative complications compared with the general population. Although the rate of surgery on HIV-infected individuals increased over time, it has not kept pace with the soaring incidence of obesity in this patient population. Future studies to evaluate the impact of percent weight loss, change in body–mass index, and HIV-specific virologic and immunologic responses are suggested to better elucidate which HIV patients may be ideal candidates for bariatric surgery.
Footnotes
Authors' Contributions
T.R.M., P.S., and B.N. were involved in study concept and design. T.R.M., P.S., and A.L. were involved in article preparation. B.N. performed the statistical analysis. T.R.M., P.S., A.L., J.N.N., A.D., and B.N. were involved in critical revisions. All authors approved of the final version of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by NIH 5 T32 DK 7356-37 (B.N.).
Appendix Table A1. International Classification of Diseases,Ninth Edition,Clinical Modification Codes Used to Define Conditions
| Diagnosis | ICD-9 codes |
|---|---|
| Baseline comorbidities | |
| Diabetes mellitus | 249.00–249.31, 249.40–249.91, 250.00–250.33, 250.40–250.93 |
| Hypertension | 401.0, 401.1, 402.00, 402.01, 402.10, 405.0, 405.01, 405.09, 405.11, 405.19, 405.91, 405.99 |
| Coronary artery disease | 410.0–410.9 |
| Cerebrovascular accident or transient ischemic attack | 434.91, 435.9 |
| Hyperlipidemia | 272.0–272.4 |
| Obstructive sleep apnea | 327.23 |
| Polycystic ovarian syndrome | 256.4 |
| Outcomes | |
| Overall | |
| Renal failure | 584.5–584.9 |
| Malnutrition | 263.0, 263.1, 263.8, 263.9, 579.3 |
| Pneumonia | 480.0–488.0 |
| Sepsis | 995.91 |
| Respiratory failure | 518.51, 518.52, 518.53, 518.81 |
| Urinary tract infection | 599.0 |
| Pancreatitis | 577.0 |
| Surgical | |
| Wound infection | 998.59 |
| Hemorrhage | 998.11 |
| Obstruction | 560.0–560.9 |
| Strictures | 560.9 |
| Fistula | 569.81 |
| Nutritional | |
| Anemia | 280.0–285.0 |
| Thiamine deficiency | 265.0–265.1 |
| Zinc deficiency | 269.3 |