
Abstract
Background:
Helicobacter pylori (HP) infection has an association with postoperative complications after bariatric surgery, but the relationship between them is controversial in the literature. The aim of this meta-analysis is to investigate the influence of HP infection on postoperative outcomes in patients undergoing bariatric surgery.
Materials and Methods:
We performed a literature search in the PubMed, EMBASE, Web of Science, and the Cochrane Library to identify eligible articles published from inception up to October 1, 2019. Study quality was assessed using the Newcastle-Ottawa scale.
Results:
Twelve studies involving 257,331 patients were finally included in the study. The summary results showed that there was no significant influence of HP infection on postoperative complications (odds ratio 1.87; 95% confidence interval [CI] 0.69–5.03; p = 0.22). However, sensitivity analysis showed that a decreased percentage excess weight loss (%EWL) at 1 year was detected in HP-positive patients (mean difference −3.41; 95% CI −5.90 to −0.92; p = 0.007).
Conclusions:
This meta-analysis has demonstrated that no significantly adverse association was found between HP infection with postoperative complications. A decreased %EWL at 1 year after bariatric surgery might be associated with HP infection.
Introduction
Since it was discovered by Drs. Warren and Marshall in 1984, 1 Helicobacter pylori (HP) has been significantly correlated with development of several gastroduodenal diseases, such as gastritis, peptic ulcers, and gastric cancer.2,3 HP is prevalent in 44.3% of the global population, 4 and a high prevalence of HP infection has been reported in obese patients.5,6 Current evidence suggests that HP infection is closely related to gastritis and malignancy, but the association between HP infection and outcomes of bariatric surgery is controversial.
Bariatric surgery has a highly effective role in achieving sustained weight loss with a beneficial effect on obesity-related comorbidities, especially for the improvements in type 2 diabetes mellitus. 7 A high incidence in bariatric patients with concomitant HP infection has been reported,8,9 and a possible relationship between HP infection and postoperative complications has often been raised.
A number of studies have clarified HP as a potential cause of postoperative complications including marginal ulcers, leak. Contrastingly, some studies have failed to confirm this, even indicating that the higher risk persisted for marginal ulcers even if the pathogen had been eradicated. 10 Comparable rates of bleeding, leak, hospital length of stay (LOS), and excess weight loss (EWL) between HP-positive and HP-negative groups were stated in a recent meta-analysis by Mocanu et al., 11 whereas HP was found as the largest independent predictor of marginal ulceration after Roux-en-Y gastric bypass (RYGB). However, only one study with postoperative marginal ulcers was included. Whether HP is associated with the adverse outcomes of bariatric surgery remains controversial.
In this study, we conducted a systematic review and meta-analysis to evaluate the influence of HP infection on postoperative outcomes in patients undergoing bariatric surgery.
Materials and Methods
Search strategy
We systematically searched the following literature databases from their dates of inception to October 1, 2019: PubMed, EMBASE, Web of Science, and the Cochrane Library. The search strategies (Table 1) included keywords related to Helicobacter pylori, bariatric surgery. The same kind of terms was connected by the Boolean operator “OR” and different kinds of terms were connected by “AND.”
Study Keywords in Search Strategy
#1 AND #2
Inclusion criteria
Age ≥18 years old
Randomized controlled trials, case-matched studies, and prospective and retrospective cohort studies
Patients undergoing bariatric surgery and with HP detection.
Exclusion criteria
Abstracts, letters, case reports, reviews, or nonhuman studies
Studies with insufficient data
Patients with preoperative HP eradication
Studies were not written in English.
Data extraction and quality assessment
Data extraction was carried out by one author and a second author checked for accuracy. After primary selection, the full texts were reviewed more thoroughly by both authors using the same criteria. If disagreement occurred, two authors discussed and arrived at consensus with the senior author. For each study, the following items were recorded: first author, year of publication, study design, ethnicity, type of surgery, and HP diagnostic method. Patient characteristics including age, gender, body mass index (BMI), comorbidities (diabetes, hypertension, sleep apnea, etc.) were assessed. The primary outcome we focused on was total postoperative complications, and the second outcomes included postoperative foregut symptoms, stricture, bleeding, leak, marginal ulceration, abscess, readmission, intraoperative blood loss, operative time, hospital LOS, and percentage excess weight loss (%EWL) at 1 year.
The methodological quality and bias of the included studies were assessed using the Newcastle-Ottawa scale (NOS) for non-randomized trials. 12 Stars awarded for each quality item serve as a quick visual assessment. The NOS consists of three parts: (1) selection of study groups (4 points), (2) comparability of groups (2 points), and (3) ascertainment of exposure and outcomes (3 points) for case control and cohort studies. NOS scores of 6 were assigned as high-quality studies.
Statistic analysis
Outcomes assessed in the meta-analysis included total postoperative complications, foregut symptoms, stricture, bleeding, leak, marginal ulceration, abscess, readmission, intraoperative blood loss, operative time, hospital LOS, and %EWL at 1 year. A pheterogeneity <0.10 or I2 > 50% suggested significant heterogeneity in the literature and a random-effect model was used. Otherwise, the fixed-effects model was adopted. A two-sided p < 0.05 was considered statistical significant. All the statistical analyses were performed using RevMan 5.3 software obtained from the Cochrane website and STATA statistical software version 15.0 (STATA, College Station, TX).
Results
Study characteristics
The process of articles selection is shown in the flow diagram (Fig. 1). We screened a total of 2093 articles after identifying duplicates. After titles and abstracts screening, 49 studies underwent full-text review. Out of these, 12 studies with a total of 257,331 patients were finally enrolled in our meta-analysis.10,13–23 The methodological quality of the included studies ranged from moderate to good, indicated by the NOS scale. Only one study demonstrated that outcome of interest was not present at the start of study. Six studies had a low risk of bias in outcome assessment. Seven studies had a low risk of bias in long enough follow-up for outcomes to occur. Similarly, seven studies had a low risk of bias in adequacy of follow-up of cohorts. All details are shown in Figure 2. Table 2 gives an overview of the characteristics of the included studies.
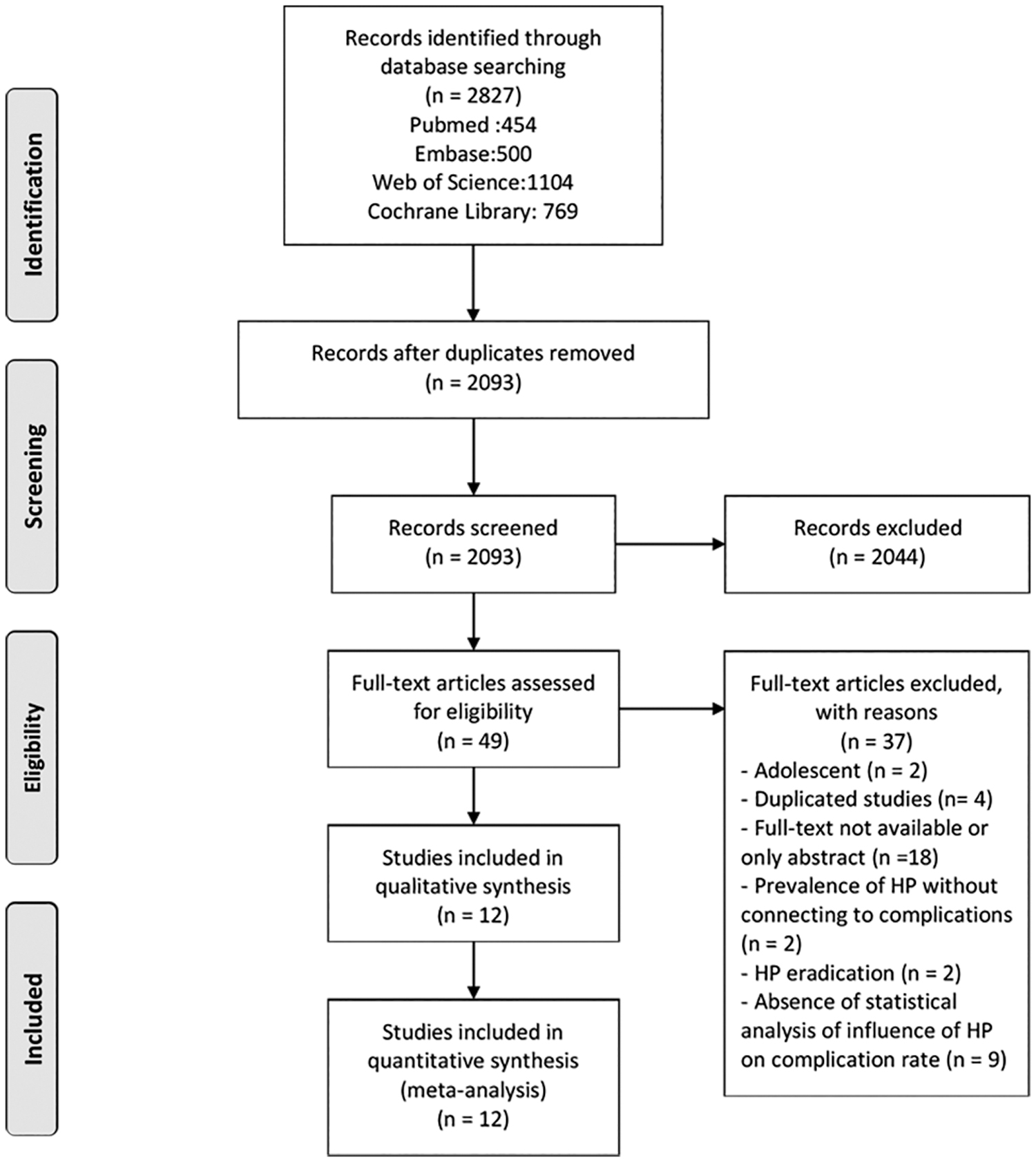
PRISMA flow diagram.
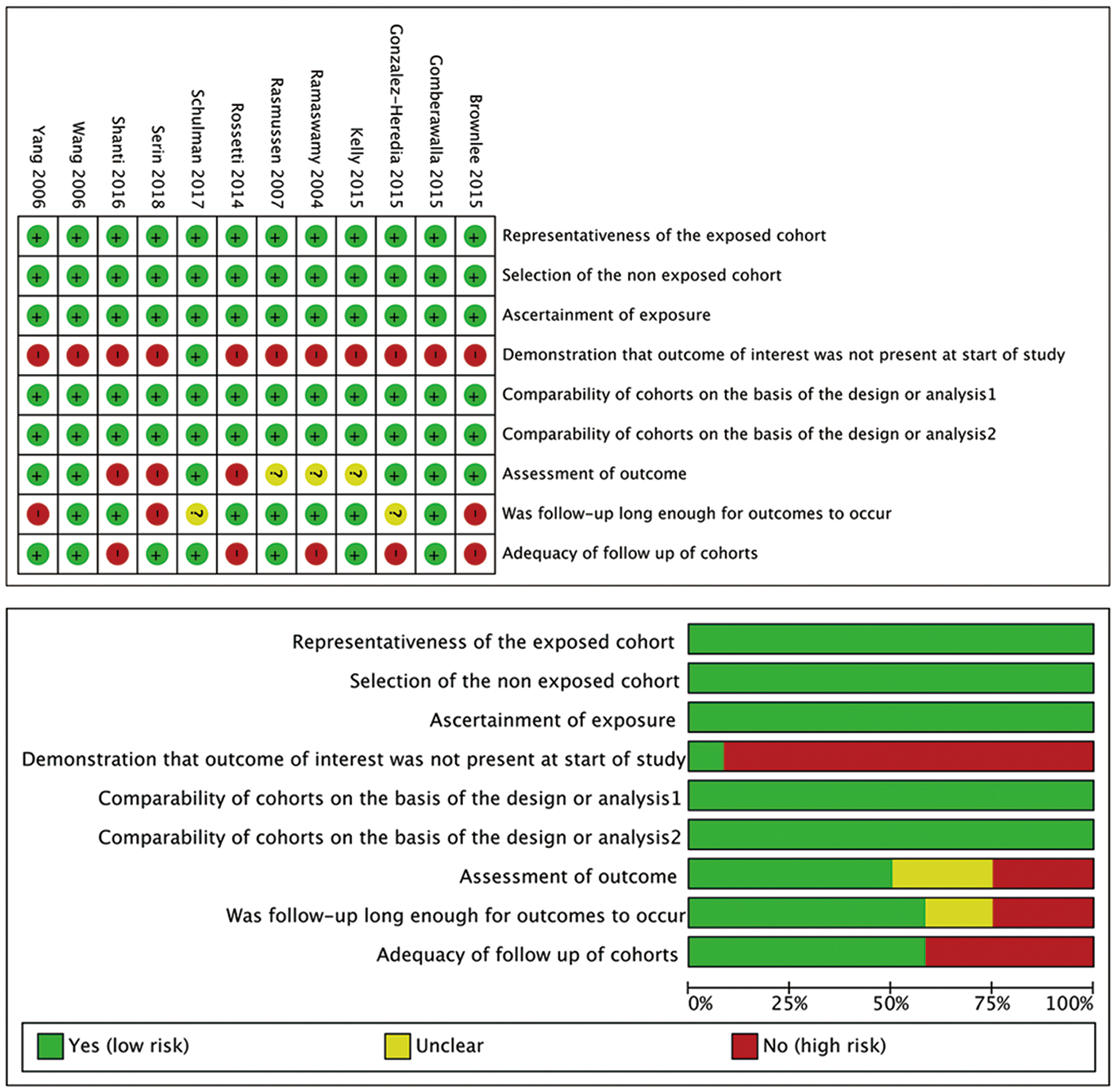
Risk of bias graph and summary. Green for low risk of bias, yellow for unclear risk of bias, and red for high risk of bias. The top (risk of bias graph) shows an overall risk of bias of each domain. For example, the length of green rectangle means the number of studies being assessed as low risk of risk. The bottom (risk of bias summary) indicates the risk of bias of each domain in each study. Color images are available online.
Overview of Included Studies
BMI, body mass index; GB, gastric bypass; HP, Helicobacter pylori; RYGB, Roux-en-Y gastric bypass; SG, sleeve gastrectomy; VBG, vertical banded gastroplasty.
Outcomes
No significant difference was observed between HP-positive and HP-negative groups for basic characteristics. The prevalence of HP ranged from 0.13% to 43.20%. In HP-positive patients, total postoperative complication rates ranged from 0% to 57.14%, complication rates of foregut symptoms ranged from 3.17% to 47.62%, stricture ranged from 0% to 9.52%, marginal ulceration ranged from 4.55% to 31.18%, bleeding ranged from 0% to 4.76%, leaks ranged from 0% to 1.92%, abscess ranged from 0.67% to 1.92%, readmission ranged from 3.17% to 23.81%, operative time of sleeve gastrectomy (SG) ranged from 63.2 to 77.5 min, hospital LOS ranged from 2.7 to 5.3 days, and %EWL at 1 year ranged from 24.2% to 75.2%.
In contrast, for HP negative patients, total postoperative complication rates ranged from 0.30% to 33.28%, complication rates of foregut symptoms ranged from 3.17% to 20.75%, stricture ranged from 0% to 4.62%, marginal ulceration ranged from 3.87% to 32.00%, bleeding ranged from 0% to 1.12%, leaks ranged from 0% to 2.68%, abscess ranged from 0% to 1.17%, readmission ranged from 2.8% to 6.74%, operative time of SG ranged from 65.6 to 86.2 min, hospital LOS ranged from 2.9 to 6.5 days, and %EWL at 1 year ranged from 28.3% to 78.3%.
Meta-analysis
Primary outcome
The primary outcome we focused on was total postoperative complications. There was no statistical significance in total postoperative complications (odds ratio [OR] 1.87; 95% confidence interval [CI] 0.69–5.03; p = 0.22) between HP-positive and HP-negative groups (Fig. 3).
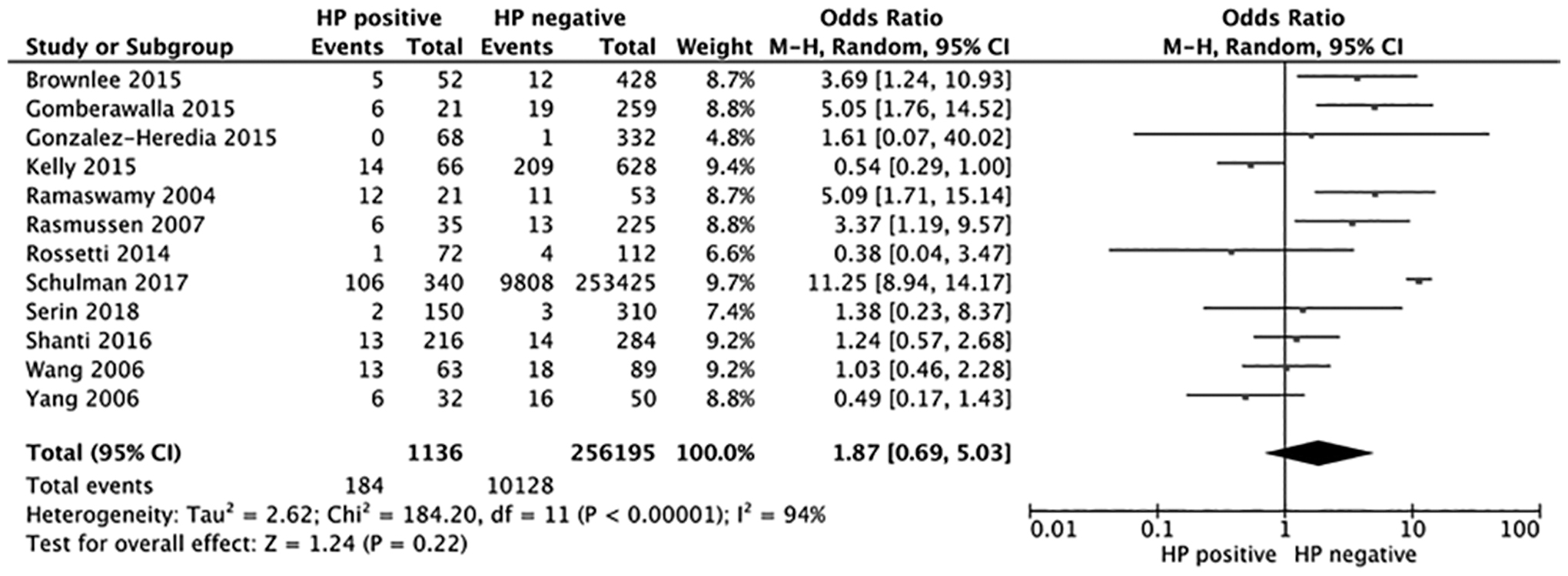
Forest plot of the primary outcome. Meta-analysis of the association between HP and postoperative complications. HP, Helicobacter pylori.
Secondary outcomes
Figures 4 and 5 show a meta-analysis of the studies reporting on postoperative foregut symptoms, stricture, marginal ulcers, bleeding, leak, abscess, readmission, operative time, hospital LOS, and %EWL at 1 year, and no statistical significance was observed between both groups. Meta-analysis could not be performed for intraoperative blood loss due to the lack of studies assessing these outcomes. Heterogeneity was found to be significant for marginal ulceration, readmission, operative time, hospital LOS, and %EWL at 1 year.

Forest plot of the secondary outcomes.
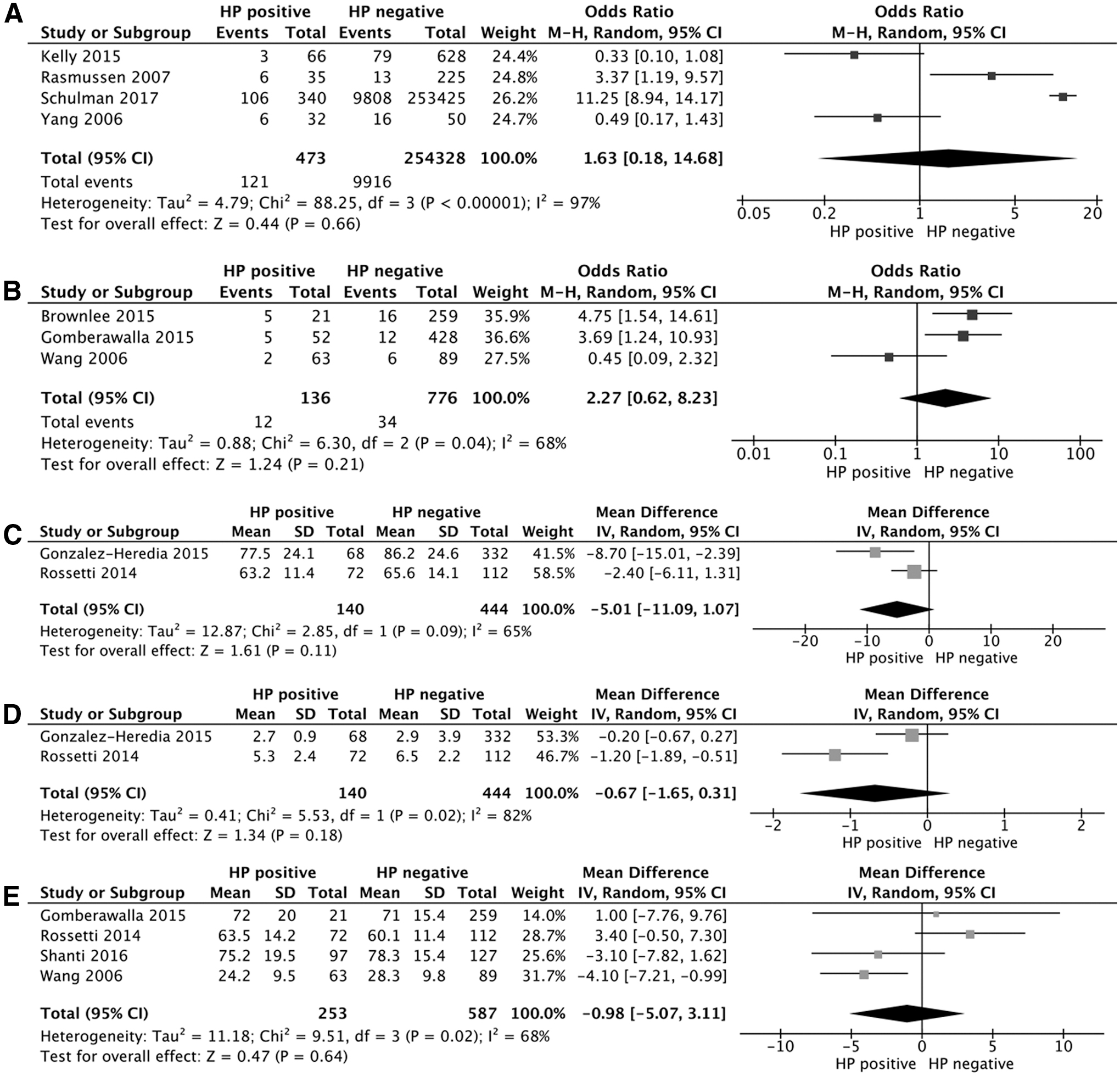
Forest plot of the secondary outcomes.
Foregut symptoms did not differ significantly between groups in four studies (OR 1.22; 95% CI 0.77–1.94; p = 0.4) (Fig. 4A). Four studies found no statistical significance for stricture (OR 0.94; 95% CI 0.15–5.8; p = 0.68) (Fig. 4B). Likewise, five studies did not find statistical significance for bleeding (OR 1.08; 95% CI 0.38–3.01; p = 0.89) (Fig. 4C). Leak (seven studies, OR 1.45; 95% CI 0.51–4.08; p = 0.48) was also similar between cohorts (Fig. 4D). And comparable rate of abscess was found between groups (OR 2.73; 95% CI 0.52–14.20; p = 0.23) (Fig. 4E).
Meta-analysis concerning the rate of marginal ulcers showed no significant difference between two groups (OR 1.63; 95% CI 0.18–14.68; p = 0.66) (Fig. 5A). Three studies examined readmission, and no statistical significance was observed for both groups (OR 2.27; 95% CI 0.62–8.23; p = 0.21) (Fig. 5B). Two studies found comparable operative time (MD −5.01; 95% CI −11.09 to 1.07; p = 0.11) (Fig. 5C) and hospital LOS (MD −0.67; 95% CI −1.65 to 0.31; p = 0.18) (Fig. 5D) between groups. Four studies found %EWL at 1 year (MD −0.98; 95% CI −5.07 to 3.11; p = 0.64) was also similar between cohorts (Fig. 5E).
Subgroup analyses
Substantial heterogeneity (I 2 = 94%) was detected in the outcome of postoperative complications. Therefore, we conducted multiple subgroup analyses to examine the relative influence of HP positive versus HP negative stratified by ethnicity, study design, and surgery type. There was an increased risk for postoperative complications among patients undergoing SG, although no statistical difference was found (OR 2.02; 95% CI 0.98–4.15; p = 0.06). There were also no differences in complications based on ethnicity and study design (Table 3).
Summary of the Meta-Analysis Results
95% CI, 95% confidence interval; N, number of studies; OR, odds ratio; ph, p-values of Q test for heterogeneity test.
Sensitivity analysis
Sensitivity analyses were performed for outcomes with high heterogeneity. After the deletion of any single study from the overall pooled analysis, we could not see any statistically significant association change between HP infection and postoperative complications (Fig. 6).

Sensitivity analysis of the association between HP infection and postoperative complications.
Owing to significant heterogeneity in %EWL at 1 year, a sensitivity analysis was performed by excluding the study of Rossetti et al., which demonstrated a decreased %EWL at 1 year (MD −3.41; 95% CI −5.90 to −0.92; p = 0.007) in patients with HP infection, as compared with no HP infection.
Discussion
Mounting studies have reported the outcomes of HP infection patients after bariatric surgery, whereas the influence of HP on postoperative outcomes was inconsistent and inconclusive. Therefore, we reviewed the published studies and took a meta-analysis to assess its influence. In general, 11 key themes for patients with and without HP undergoing bariatric surgery were calculated, including total postoperative complications (16.20% vs. 3.95%), postoperative foregut symptoms (8.47% vs. 11.95%), stricture (3.51% vs. 3.30%), marginal ulceration (25.58% vs. 3.90%), bleeding (0.77% vs. 0.76%), leaks (0.47% vs. 0.39%), abscess (0.99% vs. 0.68%), readmission (8.82% vs. 4.38%), operative time of SG (70.15 min vs. 80.00 min), hospital LOS (4.04 days vs. 3.81 days), and %EWL at 1 year (58.91% vs. 64.03%).
The present meta-analysis performed for postoperative complications showed no statistical difference between HP-positive and HP-negative groups. Subgroup analyses found no differences in complications based on ethnicity, study design, and surgery type. Sensitivity analysis revealed a decreased %EWL at 1 year in patients with HP after surgery.
Preoperative HP eradication in bariatric surgery, although investigated, is still controversial. Authors advocating eradication consider that HP is etiologically associated with gastritis and peptic ulcer. Moreover, HP has been classified as “group 1 carcinogen,” which increases the risk of cancer after surgery.24,25 Those against eradication argue that HP is associated with not only hypochlorhydria that could impair the absorption of several nutrients, but also suppressor effects of HP on ghrelin. Ghrelin is an orexigenic hormone that promotes food intake, decreases energy expenditure, and increases weight gain. 26 Eradication could result in increased hunger, food consumption, weight gain, and BMI.27,28
In this study, a decreased %EWL at 1 year after surgery was shown in patients who tested positive for HP. Similar to our finding, Goday et al. also demonstrated that HP-treated patients had a greater reduction in BMI at 3 months after laparoscopic sleeve gastrectomy (LSG) than HP-negative subjects, and the average of BMI is lower in the HP-treated group over time, whereas no difference was found between the two groups. 29 One possible explanation for our finding has been presented in the literature. Leptin is an anorexigenic hormone that suppresses food intake and increases energy metabolism, and leptin is strongly correlated with BMI due to adipose, and adipose is the major source of leptin. 30
Both in children and adults, lower concentration of leptin in patients with HP infection has been reported.26,31 In addition, both leptin and leptin receptor have been detected in the human stomach.32,33 Roper et al. found that circulating leptin levels were lower in HP-positive subjects than in HP-negative subjects, they suggested that HP can inhibit circulating leptin levels by inducing atrophic changes in leptin-producing tissues and modulating gastric cytokine function. 26 Romo-González et al. also reported lower leptin level in children with HP infection, they noted that leptin was involved in acute phase responses to inflammation during HP infection, and the leptin may be mediated through interaction with proinflammation cytokines.31,34
In our meta-analysis, although the incidence of postoperative complications was higher in the HP-positive group, no significant relationship was found between HP infection and postoperative complications. Adverse influences have been reported after bariatric surgery in patients with HP. Of those studies enrolled in our review, Ramaswamy et al. also noted that the incidence of postoperative foregut symptoms was high in the HP-positive group as compared with that of the HP-negative group (48% vs. 19%), and HP infection was found to be associated with postoperative foregut symptoms (OR 3.6; 95% CI 1.1–11.8). 13
Gomberawalla and Lutfi did not find the HP infection could increase the risk of major postoperative complications or affect weight loss, but longer hospitalization and higher readmission rates were shown in the HP-positive group. 18 In addition, some studies dispute the correlation between HP and adverse outcomes. Wang et al., Kelly et al., and Shanti et al. found no statistical difference between HP-positive group versus HP-negative group for postoperative foregut symptoms of nausea, vomiting, pain with eating, etc.14,20,22 Other complications such as leak, bleeding, stenoses, and abscess were also reported not increasing in patients with HP infection.16,19,20,22,23
In our meta-analysis, there was no significant difference for marginal ulcers between HP-positive and HP-negative cohorts in the presence of significant heterogeneity. Several authors have reported a higher rate of marginal ulcers in patients with preoperative HP infection after bariatric surgery. Schulman et al. reviewed a retrospective cohort study for the relationship between HP and marginal ulcers after bariatric surgery using the National Inpatient Sample database, marginal ulcers was observed in 31.20% in HP-positive group, compared with 3.87% in the HP-negative group. After multivariate logistic regression, HP infection was found to be the largest independent predictor of marginal ulceration with a 10-fold increase as compared with patients without HP infection (OR 11.09; 95% CI 6.5–18.9). 21 Similarly, Rasmussen et al. conducted a retrospective analysis of 260 patients undergoing bariatric surgery for factors predicting marginal ulcers and found that the incidence of preoperative positive HP status was higher in the marginal ulcer group than in the nonulcer group (32% vs. 12%, p < 0.02). 10
As was reported, increased acid exposure and mucosal ischemia at the anastomosis could promote the development of marginal ulcer, and HP could worsen it by the effects of HP on the gastric epithelium. 35 In contrast, Yang et al., based on preoperative HP status in a large series of 636 patients, reported no difference in rates of marginal ulcer formation. 15 A similar result was demonstrated by Papasavas et al., who noted that HP status had no effect on the marginal ulcer. 36 Kelly et al. even found that HP colonization seems to protect against the postoperative marginal ulcer. 20 Furthermore, HP organisms preferentially survive on and congregate along mucosa of the stomach antrum and body, whereas the most marginal ulcers are located on the jejunal side of the anastomosis and rarely the gastric after RYGB. Although HP is thought to incite an inflammatory response of gastric mucosa with proinflammatory cytokines, which can cause gastritis, intestinal metaplasia, and ultimately ulcer formation,37,38 some authors believe that marginal ulcers are more likely attributed to surgical procedure, other than HP infection.15,39 Besides, smoking, preoperative hypertension, nonsteroidal anti-inflammatory drugs, steroid or nonsteroidal inflammatory drug use, and absence of proton pump inhibitor therapy after surgery can also increase the rate of marginal ulcers.40,41 Those studies suggest that HP may have no correlation with development of marginal ulcers in patients undergoing bariatric surgery.
There are several limitations in this study. First, the number of eligible studies was small and all were nonrandomized studies. Second, 10 in the included studies were retrospective in design, which may reduce the intensity of causal evidence. Third, variability in the diagnosis of HP across studies leads to diagnostic bias. Besides, this study was also constrained to studies published in English language only, so publication bias cannot be excluded. Finally, heterogeneity across the included studies in marginal ulceration, readmission, operative time, and hospital LOS could not be eliminated, the pooled results should be treated with caution.
Overall, no statistical significance was observed for postoperative complications, including foregut symptoms, stricture, marginal ulcers, bleeding, leak, abscess, and readmission, operative time, and hospital LOS between HP-positive and HP-negative patients after bariatric surgery. However, sensitivity analysis suggested that %EWL at 1 year was lower in patients with HP infection. In summary, this meta-analysis demonstrated that a decreased %EWL after bariatric surgery might be associated with HP infection.
Conclusions
In this systematic review of the influence of HP infection on postoperative outcomes in patients undergoing bariatric surgery, no adverse association was found between HP infection with postoperative complications. However, sensitivity analysis showed a decreased %EWL at 1 year in HP-positive patients. Our results suggested that screening and treating for HP infection after bariatric surgery may need to be taken into account. More well-designed and large-scale studies are needed to assess the role of HP in bariatric patients.
Footnotes
Authors' Contributions
All authors read and agreed with the contents of the article. X.Y.Q. and Y.G. conceptualized the study. Data curation was done by X.Y.Q. and Y.W.J. Formal analysis was performed by X.Y.Q. L.M.T acquired funding. Investigation was done by X.Y.Q. and Y.Z. X.Y.Q., J.Z., and S.L. were involved in methodology. Project administration was performed by Y.G. and J.Z. Resources were taken care of H.J.Y. and J.Q. Software was taken care of X.Y.Q. and X.H.C. Original draft of the article was by X.Y.Q. L.M.T. reviewed and edited the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Natural Science Foundation of Jiangsu Province (Grant No. BK20181155) and the 333 Project of Jiangsu Province (Grant No. BRA2017109).